



Introduction
This article is the first in a series describing the establishment of an Oral Health Program for the Indigenous community serviced by Pika Wiya Health Service Inc. The purpose of this article is to describe the coming together of interested parties, the formation of partnerships, and the planning and implementing of the first stage of the Program that was to be a dental clinic and dental service for Indigenous adults.
Background
Historically, Indigenous Australians have had low levels of oral disease1. Examination of Aboriginal skull remains from pre-colonisation found low levels of dental caries among adults, and no identifiable dental caries in infants and children1. Studies by Campbell in the 1920s and 1930s of Aboriginal communities in South Australia and the Northern Territory, Australia, demonstrated increasing levels of dental caries in communities who had adopted a Western diet2-6.
The oral health of Indigenous Australians has continued to deteriorate. Aboriginal children now have higher levels of dental caries than non-Aboriginal children7,8, recently reported as more than twice the caries rates in the deciduous dentition and almost twice as high in the permanent dentition, with higher proportions of untreated disease9. Periodontal disease has become a significant problem for Indigenous adults, with periodontal health being worse than in the non-indigenous population10.
Numerous Aboriginal communities in South Australia were surveyed between 1982 and 1985, and the results reported by the Aboriginal Health Organisation of South Australia in 198811. The recommendations from this report included that a regular dental service be made available to Aboriginal people in all areas, and that Aboriginal Health Workers be trained in dental health education. To the authors' knowledge, these recommendations for the Port Augusta region from over 10 years ago have not been actioned in any systematic way.
The Aboriginal Community of South Australia's mid-north consists of more than 5000 people in a regional centre (Port Augusta) and surrounding remote areas (extending to Leigh Creek, Copley, Nepabunna and Marree) (Fig 1). Over half of this population is under 25 years of age12 and the Indigenous unemployment rate is 14.9%. Aboriginal communities in this region have identified dental health as one of the top health priorities for their respective communities through the 'First Step' document13, which outlines regional plans identifying the health and health-related priorities for the Aboriginal communities in each region, as identified by the Aboriginal people consulted in that region.
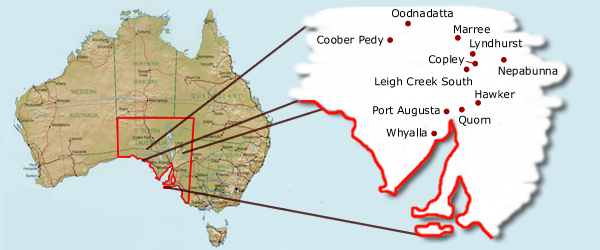
Figure 1: Map of the study area in South Australia.
The oral health issues of the Indigenous people in the region are believed to arise from a combination of the general problems of remote locations and the specific problems of Aboriginal communities, including socioeconomic disadvantage and the fact that Indigenous people are the least healthy sub-population in Australia, including low birth weight, shorter life expectancy compared with non-Indigenous Australians, high infant mortality, high rates of and poorer outcomes associated with cardiovascular disease, respiratory disease and diabetes14. Problems also stem from Aboriginal communities having poor access to dental services in general15. Where these services are available they tend to be 'dentist-centred' rather than employing strategies that are sensitive to and meet the cultural needs of the Aboriginal community10.
There have been several relatively unsuccessful attempts over the years to address the issue of sub-optimal access and utilisation of available dental services by the Aboriginal community in Port Augusta. Also, Pika Wiya Health Service had, on more than one occasion, expressed concern that cultural barriers prevent some of their clients from fully accessing available services. These barriers include issues such as affordability, distance, the availability of transport, language barriers and the cultural appropriateness of service delivery16.
The Setting
Port Augusta is situated 322 km north of Adelaide, the capital city of South Australia (SA), at the head of the Spencer Gulf. Port Augusta's population is approximately 13 500 of which 15% (2040) are of Aboriginal or Torres Strait Islander descent17. It was reported after the 2001 Census that despite a 5.2% decrease in Port Augusta's population from 1996 to 2000, the Indigenous population had increased by 6.5%18. Port Augusta's Indigenous community represents many cultural groups from different parts of Australia. As well as Indigenous people who reside in Port Augusta, a portion of the Aboriginal community can be described as transient, with Aboriginal people travelling to and from Port Augusta from many areas of Australia to visit family and friends, and for cultural, social, legal and religious reasons19.
Pika Wiya Health Service was first formed as an Aboriginal Medical Service in 1974 with funding from the Council of Churches in Geneva, Switzerland and supported by Redfern Aboriginal Medical Service, New South Wales, Australia. Pika Wiya Health Service became incorporated under the SA Health Commision Act in 1984. Now incorporated under the Aboriginal Services Division of the Department of Human Services, Pika Wiya Health Service Inc has close affiliations with the South Australian Aboriginal Health Council and is represented on the National Aboriginal Community Controlled Health Organisations board by the Chief Executive Officer. Pika Wiya Health Service Inc operates from recently renovated and modern premises in Port Augusta and has 5572 active Aboriginal and Torres Strait Islander clients20.
Pika Wiya Health Service has four service locations; Port Augusta, Davenport, Copley and Nepabunna. The Port Augusta Service combines a medical service and programs ranging from women's health, sexual health and children's health to diabetes education and social and emotional wellbeing programs. PIKA (meaning 'sickness') WIYA (meaning 'no'), is derived from the Pitjantjatjara language. The mission statement of PWHS is to:
...provide a culturally appropriate service to Aboriginal and Torres Strait Islander people, addressing preventative, promotive and curative aspects of health, which encourages our community to achieve greater dignity and quality of life equal with all Australians.
This first stage of the Oral Health Program focuses on Pika Wiya's Port Augusta and Davenport communities.
Forming a working group
Pika Wiya Health Service CEO and the Manager of Special Projects, approached the South Australian Centre for Rural and Remote Health (SACRRH), The University of Adelaide Dental School and the South Australian Dental Service (SADS), requesting assistance to address the issues of oral health within the community, with particular focus on underutilisation of services. As a result of the request by PWHS, a group of interested parties came together to plan possible responses. The group formed a working party and included representatives from the following bodies.
- Pika Wiya Health Service Inc (PWHS): Port Augusta's local Aboriginal Health Service, being an Aboriginal Medical Service and has Aboriginal community members appointed to the Board for a period of 2 years who are representative of the diversity of the Aboriginal Community. All service and program proposals must be approved by the Board.
- SADS: providers of publicly funded dental care and oral health programs in South Australia.
- SACRRH: established in 1997 as one of ten University Departments of Rural Health (UDRH) across Australia. The UDRH are key players in the Commonwealth Government's response to increasing the number of health professionals in rural areas and improving the health and service delivery needs of rural communities.
- Adelaide University Dental School: which has a long history of involvement in Indigenous oral health and has recently become involved in several projects addressing oral health needs in Southern and Central Australia.
The key issues identified by the working party were:
- Lack of appropriate facilities and trained staff.
- Lack of acknowledgement of the central role of Aboriginal Health Workers in provision of health care in Aboriginal communities.
- Limited range of culturally sensitive education and health promotion resources and programs.
- No base from which to offer primary care services.
- No locally available training programs for staff.
The working party examined a number of possible responses to issues identified including possible location, service structure, staff availability and training.
The service model
The vision for the project was to establish a culturally sensitive, quality oral health program that catered to the oral health needs of the Indigenous community serviced by the PWHS. Specifically, a service that provided emergency and routine dental care, preventative services and community oral health promotion, and would have the capacity to adapt to address the specific needs of the community.
The partners, however, acknowledged the need for a comprehensive program to be implemented in stages; the first being the establishment of a dental clinic within PWHS, Port Augusta town clinic, and a service for eligible Indigenous adults. With anticipated success of this first stage, further integrated programs, preventative services and health promotion could be developed and implemented.
The resultant service model was developed to address the first key issues as a priority and to provide a base to further develop the service capacity to progressively address all the key needs identified.
Staffing
The following staff were recruited for the service:
- A dentist: a new graduate from The University of Adelaide, SA, and originally from the local area was recruited as a joint appointment between PWHS, the SADS and SACRRH.
- A dental assistant: recruited locally from the SADS to work with the dentist on clinical days.
In the first six months following establishment of the dental service reception, administration and transport support were provided for dental patients through existing services already offered by PWHS. These services were later augmented by the recruitment of an Aboriginal Health Worker to the program.
A full time Aboriginal Health Worker joined the program in October 2001, 6 months after the clinical service began. The role of the health worker included reception duties, research assistance, health promotion, client recruitment and follow up and program development.
Infrastructure
A room was allocated in the newly developing PWHS building for a single-chair dental clinic and office. Although funded by PWHS, the clinic was established as a SADS clinic, ensuring some uniformity in terms of infrastructure, technical support and policies.
Service structure
The initial dental program consisted of an adult clinical service 2 days per week for eligible clients of Aboriginal and Torres Strait Islander descent, and health promotion at PWHS Open Day and local school festival.
PWHS has supplemented its existing patient transport service to include a transport service for patients to the Radiology Department of the Port Augusta Hospital for dental x-rays and/or the local pharmacy to collect medication related to the dental service. This service is provided primarily to elderly, ill patients or those with small children or other issues affecting their means to access public transport. It is, however, acknowledged that other patients also have difficulty accessing private vehicles and funds for public transport or taxis.
Launch
The dental clinic was officially opened on 1 May 2001. The launch coincided with the SA Indigenous Oral Health Workshop, held at Pika Wiya.
Outcomes
The community acceptance of the service has been better than anticipated. The high demand for services was evident almost immediately, necessitating booking of appointments well in advance. Appointments were predominantly for relief of pain and, in the first instance, attendances for pain were allocated priority to manage the level of demand.
The number of adult patients seen in the first fully operational financial year (July 2001 to June 2002) was 229 individuals, with a total of 467 visits, and 1375 treatments. In addition, 63 children were provided a total of 207 treatments. These were predominantly children receiving emergency care, or those who attended when their parents also had an appointment.
Acceptance was further exemplified by the observation that even clients who did not use Pika Wiya's Medical Service were still making appointments at the dental clinic. Based on demand and utilisation, the management of PWHS assessed as successful this first stage of implementation of a more comprehensive program.
Strengths of the service
Factors believed to have contributed to the success of the sevice, through observation by the authors and others involved with the service, experience and ongoing consultation and reflection include:
- The location of the clinic within the main health centre premises, promoting dental care as an integral part of general health care.
- A resident dentist employed by the health service.
- The enthusiasm and commitment of stakeholders.
- A team approach utilising each stakeholder's area of expertise.
- The allocation of an Aboriginal Health Worker to the program team.
- The recruitment of staff who did not have rigid and preconceived ideas on the way the service should be organised and delivered.
- The ability of the program to be flexible and adapt with feedback from the community.
- Including local staff in decision-making, seeking opinions and including them in the development of the program - this has been vital in ensuring continued positive relationships between local organisations and staff.
- The employment of local staff living in the community.
- The acceptance of cultural diversity and its impact on clinical service.
Learnings observed
Areas which have been identified as key learnings by stakeholders and staff include:
- The need for acceptance and acknowledgment of the time needed to develop policies and procedures.
- The need to have an Aboriginal Health Worker as a core staff member in the early stages of program development and establishment.
- A need for culturally specific support staff.
- A need for support staff specifically allocated to the dental program, to prevent additional pressure on already busy staff, and associated resentment towards a new program.
- Recognising the need for further discussion and acceptance within the community before decisions made by stakeholders can be implemented.
- Acknowledging that in a small community with a small staff pool, a change for PWHS can have significant implications for other local services and staff and, hence, the need for consultation and inclusion to foster positive relationships.
A significant and ongoing issue for the efficient operation of the clinic is the rate of failure to attend scheduled appointments. In some instances demand did not translate into attendance. In the period June 2001 to July 2002 there were a total of 301 failed appointments. Numbers of failed appointments affects clinical productivity, impedes the timely delivery of treatment plans and impacts on clinical service time available to other patients. In many instances failure to attend scheduled appointments can be justified by family and social obligations21. In others, patients may not realise the value of and need for dental care in terms of their general health. It is hoped that progressive implementation of a more comprehensive system of coordination of dental appointments with other health programs will address some of the attendance issues.
Program areas for further development
Now that the program is demonstrating high levels of demand, utilisation and acceptance by the community, an important next step is to secure on-going funding for the service. In addition, it is also apparent that expansion of the service may be required to enable patients to have all their treatment needs met, and to move towards a routine and preventative rather than an emergency care only clinical service.
Implementation of a school dental program as well as health promotion programs to increase awareness of dental health are also required and are in early stages of development. These will be discussed in future articles.
Relationships with the Australian Institute of Health and Welfare Dental Statistics and Research Unit and the SADS Evaluation and Research Unit are being developed to ensure that all relevant and appropriate data is recorded for the program, and is consistent with that being recorded nationally. Collection of data will not only contribute to a nation-wide data set, but will also provide baseline data on disease rates and attendance patterns from which to evaluate the impact of the service and oral health programs.
The issue of inadequate clinical and health promotion services in more remote areas serviced by PWHS needs to be addressed. Patients have been known to travel in excess of 3 hours to Port Augusta for dental treatment. PWHS in collaboration with the University of Adelaide Dental School and SACCRH have been awarded a National Health and Medical Research Council grant to evaluate the need for and suitable approaches to delivering oral health programs for these areas. Training of Aboriginal Health Workers in disease prevention and health promotion strategies will also be essential to ensuring long-term improvements in the knowledge and oral health of the community and for building capacity of the health service and its workers. The use of PWHS as a base from which to provide training is under consideration.
PWHS has solid relationships with the SACRRH for student placements, including medical students, nursing and allied health students. With the partnership already in place for the dental program, it is anticipated that dental students will be involved in clinical service delivery, health promotion and research.
Summary and conclusion
The partnership between PWHS, the SACRRH, the SADS and the University of Adelaide Dental School has enabled the successful implementation of a dental service for the Port Augusta Indigenous community, employing its own dentist and dental health worker and operating from within PWHS premises. In its first 12 months the service treated a total of 229 patients over 467 visits, providing more emergency-type treatments than routine and preventative, including 222 emergency or 'limited' oral examinations and 184 tooth extractions, in comparison with 61 comprehensive oral examinations and 165 preventative services, such as oral hygiene instruction and removal of calculus. The service has many opportunities for further program development. It is anticipated that this is the first of many significant steps towards addressing the oral health needs of the Indigenous community in the mid-north of South Australia.
Acknowledgements
The authors would like to acknowledge Cephas Stanley (CEO, PWHS), PWHS staff, Maria Calyun, Aboriginal Health Worker, David Clark (Director, Statewide Dental Services, SADS), SA DS management and local staff, Dianne George (SADS Dental Therapist and Pika Wiya Dental Assistant) who have all played crucial roles in the planning, establishment and continuing activities of the Pika Wiya Dental Service. Spencer Gulf Rural Health School is an initiative of The University of Adelaide and the University of South Australia and is supported by the Commonwealth Department of Health and Ageing.
References
1. Campbell TD. The dentition and palate of the Australian Aboriginal. Adelaide: University of Adelaide Publications, no 1, 1925: 72-78.
2. Campbell TD, Lewis AJ. The Aborigines of South Australia: Dental Observations recorded at Ooldea. Australian Journal of Dentistry 1926; 30: 371-376.
3. Campbell TD. Observations on the teeth of Australian Aborigines, Hermanssburgh, Central Australia. Australian Journal of Dentistry 1937; 41: 1-5.
4. Campbell TD. Observations on the teeth of Australian Aborigines, Cockatoo Creek, Central Australia. Australian Journal of Dentistry 1938; 42: 41-47.
5. Campbell TD. Observations on the teeth of Australian Aborigines, Mt Liebeg, Central Australia. Australian Journal of Dentistry 1938; 42: 85-89.
6. Campbell TD. Observations on the teeth of Australian Aborigines, River Diamentina, South Australia. Australian Journal of Dentistry 1938; 42: 121-124.
7. Davies MJ, Spencer AJ, Westwater A and Simmons B. Dental Caries among Australian Aboriginal, non-Aboriginal Australian-born, and overseas-born children. Bulletin of the World Health Organisation 1997; 75: 197-203.
8. Cooper MH, Schamschula RG, Craig GG. Caries experience of Aboriginal children in the Orana Region of New South Wales. Australian Dental Journal 1987; 32: 292-294.
9. Roberts-Thomason K. Oral Health of Aboriginal Australians. LAustralian Dental Journal 2004; 49: 151-153.
10. Commonwealth Department of Health and Ageing. National Aboriginal and Torres Strait Islander Oral Health Workshop Report. Canberra: Commonwealth Department of Health and Ageing, 2003.
11. Chryssides H. A report of the dental survey and treatment of Australian Aborigines in the North-west communities of South Australia, Port Augusta (and surrounds), Ceduna, Yalata (and surrounds). Adelaide: Aboriginal Health Organisation of South Australia, 1986.
12. Employment and Skills Formation Directorate. Department of Education, Employment, Science and Technology. Employment and skills formation regional profile (northern). Canberra: Department of Education, Employment, Science and Technology, 2004.
13. Aboriginal Health Council of South Australia. South Australian Aboriginal Health Regional Plans: The first step..... 1998. Dulwich, SA: Aboriginal Health Council of South Australia, 1998.
14. Australian Indigenous Health InfoNet. Summary of Indigenous Health, June 2003. (Online) 2004. Available: www.healthinfonet.ecu.edu.au (Accessed 6 April 2005).
15. Meihubers S. Dentistry in remote Aboriginal communities. Alice Springs, NT: Nganampa Health Council, 2001.
16. Trewin D, Maddern R. The Health and Welfare of Australia's Aboriginal and Torres Strait Islander Peoples 2003. AIHW Cat. No. IHW-11. Canberra: Australian Institute of Health and Welfare, 2003.
17. Australian Bureau of Statistics. Basic Community Profile and Snapshot: Port Augusta. Canberra: Australian Bureau of Statistics, 2001.
18. Anon. City's population down 5.2 percent, Aboriginal population up 6.5 percent. Transcontinental Newspaper, 19 June 2002, p 3.
19. Spencer Gulf Rural Health School. Working with Aboriginal People in Rural and Remote South Australia; a cultural awareness handbook for people working in the health professions. Whyalla: Spencer Gulf Rural Health School, 2001; 28.
20. Office of Aboriginal and Torres Strait Islander. Pika Wiya Health Service 2003/2004 Health Service Activity Report. Canberra: Office of Aboriginal and Torres Strait Islander, 2004.
21. Social Justice and Country Division, Department of Human Services SA. Working with Aboriginal People: A cultural guide for community-based Health and Home Care Services in South Australia. Adelaide: Social Justice and Country Division, Department of Human Services SA, 2003.
Published 27 April 2005; Acknowledgements modified 7 June 2005.