
The purpose of this study was to retrospectively collect health statistical data from the Mondaña Health Clinic in Mondaña, Ecuador (Figure 1). The clinic is a project of the Foundation for Integrated Education and Development (FUNEDESIN), a non profit non-governmental organization (NGO) based in Quito, Ecuador. The Mondaña clinic receives support from MAP International (a non-profit Christian relief and development organization) via USAID funding.

Figure 1: The Mondaña Health Clinic, Ecuador.
In 1992, FUNEDESIN began community development and educational outreach in the Napo Province along the Napo River. Its field headquarters is located in the community of Mondaña, located two hours (by motorized canoe) from the nearest main port of Misahuallí. There are no access roads, electricity, or telephones in the region. The Mondaña Clinic opened in October of 1997 and in 2000 served more than 3000 people in communities along the Napo River. The population base of the Mondaña Clinic service area is primarily Indigenous Quichuas and a number of colonists who have migrated from the highlands and coastal regions of the country.
The project was been funded by private, corporate, and non-profit foundation donations1.
Although accurate data have been tabulated since the inception of the clinic, there have been no attempts at collecting, organizing, and analyzing these data. Data generated from such analysis could prove useful to the physicians as well as to the funding organizations. These health data provide a baseline measure of the major health diagnoses in the clinic, which facilitates comparison with other regions of the Amazon. Furthermore, the data analysis of patient visits provide preliminary estimates of the epidemiology of the major diseases of patients seen at the clinic. A number of authors have demonstrated the usefulness of such data in describing the specialty of family practice and other primary care professions2-4. It is hoped that the present study will do the same in the Amazon region. The current study also undertook a brief comparison of data with that from the USA to demonstrate the considerable differences in activity in these two health systems.
Methods
An Microsoft Access database was designed to enter data collected from daily patient reports, which were transcribed by the physicians while documenting more detailed information in patients' charts. The variables collected and entered in the database include: date of consultation; age; sex; community; patient's name and health record number; diagnoses; and diagnosis cluster. The local physicians helped clarify and categorize certain diagnoses.
Data were collected from daily health reports between January and September 1999 (n = 765 patients). The period was less than a full year due to limitations on the study time in Mondaña. To ensure the validity and reliability of the data, the clinic numbers and names were filtered and matched to ensure consistent data in terms of patient ages and home communities. Inconsistencies were followed up by direct reference to patient health records.
The diagnostic clusters were adapted from Schneeweiss, Cherkin, Hart et al.3 and Williams, Philbrick, Becker et al.4; however, small adjustments were made to accommodate the international context. For example, because of the high prevalence of parasitic infections (rather than infectious diseases), a specific category recognizing parasitic infections as a sole independent category was created. Dagnostic clusters were also used to help facilitate a general overview, without sacrificing detail of the diagnoses clusters. As Schneeweiss and Hart wrote: 'Diagnostic clusters capture the great majority of ambulatory patient visits and result in a more manageable number of clinically related entities'5.
Data were analyzed by creating queries in Microsoft Access and creating specific categories to filter the data (i.e. sex, disease category, and domicile). Due to a shortage of time, home community data were not collected for all patients. EPI Info 2000 (WHO software) was used to analyze the data by generating frequencies and means. Microsoft Excel 97 was used for further calculations of percentages and creating pie charts and histograms. Fisher's Exact Test was performed to compare data between males and females using Analyze-It Software.
Results
There were 765 patient visits with at least one diagnosis in the months of January 1999 to September 1999; 175 patient visits had 2 diagnoses. The demographic distribution (Table 1, Figure 2) found that of the 765 patient visits (some were repeat visits), 319/753 (42%) were made by males and 434/753 (58%) were made by females; 66% patient visits were made by those under the age of 25 years old. In most age groups, females outnumbered males for patient visits but this was not statically significant. However, there were more male patients in the 46-50 years and greater than 51 years age group. Diagnoses were always made on the basis of the patient's history and physical examination. In some cases, rudimentary laboratory tests (eg urinalysis, stool ova and parasites, and hematocrit) were used to supplement the clinician's diagnostic capabilities.
Table 1: Age and sex distribution of Mondaña Clinic patients, Ecuador, January-September 1999
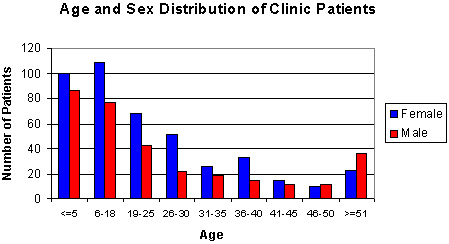
Figure 2: Age and sex distribution of Mondaña Clinic patients, Ecuador, January-September 1999
The major differences and similarities in diagnoses between the sexes for patient visits is shown (Table 2). For both males and females, the two most frequent diagnoses clusters were acute upper respiratory tract infection (URTI) and parasitic infection. However, despite these similarities, males patient visits had a higher frequencies of URTI (24.7%) and parasite infection (19.7%) than female patient visits (17.3% for both). Female patient visits had pregnancy care ranked third in frequency (14.8%), urinary tract infection ranked fourth (13.6%), and lacerations, abrasions, and contusions ranked fifth (5.4%; Figure 3). Male patient visits due to lacerations, abrasions, contusions (9.7%) ranked higher than for females; fungal infections were fourth ranked (8.4%), and dermatitis ranked fifth (6.0%; Figure 4). Gastritis ranked higher in females than in males.
Table 2: Major differences between and similarities in diagnoses for male and female patient visits to Mondaña Clinic, Ecuador, January-September 1999: 15 most frequent diagnoses
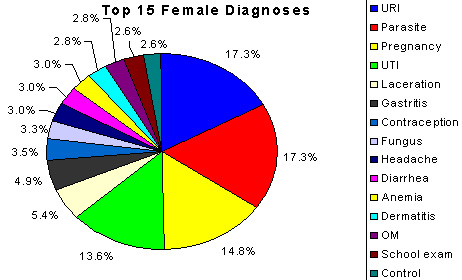
Figure 3: Female patient visits to Mondaña Clinic, Ecuador, January-September 1999: 15 most frequent diagnoses.
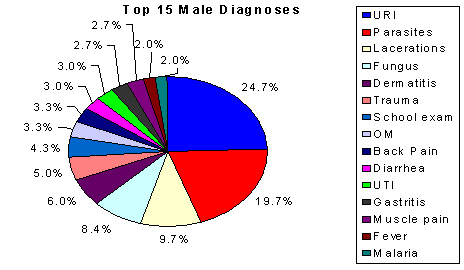
Figure 4: Male patient visits to Mondaña Clinic, Ecuador, January-September 1999: 15 most frequent diagnoses.
Using Fischer's Exact test, three diagnoses-clusters were found to be statistically significant. Male patient visits had 24.7% visits due to acute URTI compared with 17.3% for females (p = 0.0457). Also, female patient visits had a fourfold higher frequency of urinary tract infections compared with male patient visits (13.6% vs 3.0%, p<0.001). Finally, male patient visits had a twofold higher frequency of being for fungal infections compared with female patient visits (8.4% vs 3.3%, p = 0.008).
There were minimal differences between patient visits for male and female children in regards to the five most frequent diagnostic clusters (Table 3). Again acute URTI and parasite infections were the major diagnoses but in this case, male patient visits had higher rates than did female patient visits for acute URTI (42.5% vs 36.4%) and female patient visits had higher rates in the parasite infection category (29.9% vs 21.9%). Female patient visits had higher rates of diarrhea (diarrhea not otherwise specified - most parasitic infections cause diarrhea) than did male patient visits (13.0% vs 8.2%). But male patient visits (15.1%) had higher rates of fungal infection than did female patient visits (not among five most frequent, but at 3.7%). Male and female patient visits had dermatitis as fourth most frequent, but male patient visits had higher rates than female patient visits (12.3% vs 11.7%).
The patients' home community is shown (Table 4). Mondaña had the highest frequency of patient visits to the clinic because the clinic is located in Mondaña. However, the distance from the clinic does not predict patient visit rates. For example, Yuralpa Izquierda is farther away from Mondaña than 30 de Agosto, but still had more patient visits to the clinic.
Table 3: Five most frequent diagnoses for children aged 5 years and younger at Mondaña Clinic, Ecuador, January-September 1999
Table 4: Greatest frequent of visits to Mondaña Clinic, Ecuador, by patient home community, January-September 1999
Discussion
There were some significant differences in patient visits to the Mondaña Health Clinic between males and females. For example, 58% of the patients visiting the Mondaña Health Clinic were female, compared with 42% males. When compared with the most recent US data on ambulatory visits, women represented 60.3% of all patient visits to primary care physicians compared with 39.7% male patient visits6.
There are also major differences in the age distribution of patients at the Mondaña Health Clinic, compared with US population ambulatory visits. For example, 66% of Mondaña Clinic patients were 25 years old or younger. In the US data, 17.6% of the patients were less than 15 years old and 8.6% of the population were 15-24 years old. If the latter two categories are combined, this equals 26.2% of the population, which is considerably less than the 66% of 25 years old or younger at Mondaña. One reason for this difference is the lower life expectancy in the Amazon region. For example, although there are no statistics for the life expectancy of people living in the Amazon region, in Quito, life expectancy is 68.8 years (66.4 for males and 71.4 for females)7.
There were major differences in diagnoses between males and females visiting the Mondaña Health Clinic. Many of these differences are due to the many reasons for women's use of the clinic, including prenatal care and deliveries, and that males used the clinic only in acute emergency situations. For example, males visited the clinic for acute injuries more frequently than did females, which is consistent with the type of physical labor that men do in that area (ie agriculture). However, women used the clinic to deliver their children and to seek prenatal and postnatal care. Interestingly, normal pregnancy was the second most common diagnosis for females in the US, while in the Mondaña Clinic, it ranked third behind URTI and parasite infections.
Women also had more patient visits for gastritis compared with men (4.9% vs 2.7%). The higher rates of gastritis in women may be due to higher rates of Chicha (alcoholic beverage of the native people) consumption because women are traditionally the producers of Chicha, which originates from fermented yucca root/manioc. In regards to the US data, surprisingly the most common diagnosis cluster was acute URTI at 4.1% of all patient visits (females 3.7% and males 4.8%)6. Similarly, the Mondaña Health Clinic patient visits for males and females ranked highest for acute URTI; similarly to the US data, males had higher rates than females for patient visits for URTI (24.7% vs 17.3% p 0.0457).
Another major significant finding was the fourfold difference between female and male paient visits for urinary tract infections (UTI)(females 13.6% vs 3.0% p <0.001). Although UTI did not rank in the 15 most frequent diagnoses in the US data, there is evidence to suggest that females have a 50% higher risk of UTI than do males in the US8. The higher rates may be due to a combination of poor hygiene aggravated by a more humid climate. Also the different rates in males and female can largely be attributed to the anatomical juxtaposition of the GU and GI tract termini in the human female. Finally, male patient visits had a two-fold higher frequency of fungal infection diagnosis compared with female patient visits (8.4% vs 3.3% p = 0.008). The major diagnoses in the USA were not ranked in the top 15 major diagnoses in Mondaña (ie essential hypertension, diabetes mellitus, malignant neoplasm, ischemic heart disease).
These data will be of importance for those interested in working in the Mondaña Health Clinic. Visiting physicians will be able to prioritize resources and funding agencies will be able to use this information to compare to other sites in the region as well as a baseline against future preventive public health interventions.
Some limitations to the data are the validity of the diagnosis. For example, although gastritis is a pathologic diagnosis based on lab tests and endoscopy, this diagnosis was made entirely on the basis of the patient's history and physical examination. Also, parasitic and fungal infection diagnoses were made without confirmatory laboratory procedures. Furthermore, the lack of separation of the children and adults into separate groups may skew the data and lead to selection bias because children are more prone to develop certain diseases. Moreover, although the comparison between patients in Mondaña and the USA demonstrated differences in health systems, the fact that the social, political, economic, and geographic differences are extensive deemed this comparison invalid. However, one of the reasons for the comparison was that the US statistics are easily accessible.
Future studies should compare Mondaña to other South American or other developing countries. Also, the fact that our study period was 9 months rather than 12 months limits the validity of our study because this does not take into account seasonal variation over 12 months. The reason for collecting data for 9 months was time limitation.
Acknowledgements
Rodney Samaan was the principle investigator for this study. Dr Karl Seydel was involved in the preparation of the manuscript as well as the design of the graphs and calculation of the statistics. Seth Crockett and Alison Nemes were involved in the review of the manuscript. Dr Matheny and Dr Pearce provided guidance for this study and manuscript. The authors would like to thank Douglas McMeekin for his hard work and perseverance in creating FUNEDESIN. Our thanks also goes out to Claire Boswell and Marci Stoterau from MAP International, whose support was constant. The staff of the Mondaña Clinic was invaluable and incredible. We also want to thank Dr Peli Grosa from the University of Kentucky for help in editing this manuscript. Finally, our gratitude goes out to University of KY Basic Research Foundation who funded the trip to Ecuador.
References
1. FUNDESIN (Foundation for Integrated Education and Development). (Online) http://www.fundesin.org Accessed 23 November 2001.
2. Marsland DW, Wood M, Mayo F. Content of family practice. Part I. Rank order of diagnoses by frequency. Part II. Diagnoses by disease category and age/sex distribution. Journal of Family Practice 1976; 3: 37-68.
3. Schneeweiss R, Cherkin D, Hart G et al. Diagnosis clusters adpated for ICD-9-CM and ICHPPC-2. Journal of Family Practice 1986; 22: 69-72.
4. Williams B, Philbrick J, Becker D, McDermott A, Davis R, Buncher P. A patient-based system for describing ambulatory medicine practices using diagnosis clusters. Ambulatory Medicine 1991; 6: 57-63.
5. Schneeweiss R, Hart G. Diagnostic content of ambulatory primary care: implications for resource utilization. Journal of Ambulatory Care 1988; 11: 13-22.
6. Woodwell D. National Ambulatory Medical Care Survey: 1998 Summary. Advance Data, No. 315, 19 July 2000, US Department of Health and Human Services. Atlanta: Centers for Disease Control and Prevention.
7. Ecuador: Health in the Americas, Volume II, pp 240-257. (Online) 1998. Availabe: http://www.paho.org/english/HIA1998/Ecuador.pdf
8. Isselbacher K, Braunwald E, Wilson K et al. (Eds). Harrison's Principles of Internal Medicine, 13th edn. New York, NY: McGraw Hill, 1994.
Published 2 December 2003; style modified 23 July 2003.