full article:
Introduction
Regular participation in physical activity reduces the risk of developing chronic health issues, such as cardiovascular disease, obesity, diabetes, cancer and depression1,2. For children, physical activity plays an essential role in their physical, social and mental development3,4. To attain these health benefits, the Australian Physical Activity Guidelines recommend that children aged between 5 and 17 years should participate in at least 60 minutes of moderate-to-vigorous physical activity daily3,5. Unfortunately, an increasing number of children seldom meet these recommendations, particularly children with a disability6,7, and children without a disability who live in rural or remote areas8,9.
While there are no specific recommendations for physical activity participation for children with a disability, evidence suggests that children with a disability are not participating in the recommended amount of physical activity and, as a result, may not be reaping the associated health benefits10-15. Numerous studies have described barriers to participation in physical activity faced by children with a disability10,11,13,16. These barriers include a lack of capacity for physical activity15,17, the child’s own fear and anxiety toward participation16, and negative attitudes toward people with a disability from peers, educators, health professionals, and the wider community15,17. Other barriers that have been reported include inadequate facilities, and a lack of appropriate physical activity programs for children with a disability18. Further, a limited understanding of the health benefits that physical activity provides for children with a disability17,19, financial difficulties20, and a lack of time from parents to facilitate their child’s participation in physical activity13,16,17.
Similarly, children without a disability who live in rural or remote areas of Australia are generally not meeting the recommendations for physical activity8. These children face several barriers to physical activity participation specific to residing rurally. These barriers include a lack of facilities and infrastructure8,21-23, poor public transport, vast geographical distances to travel to facilities, as well as financial and time constraints22,23. Additionally, rural environments are more likely to have climatic extremes, which may further limit physical activity participation21.
Currently, there is a dearth of literature investigating the physical activity participation of rurally residing children with a disability. One study reported that rurally residing children with a disability were not participating in the recommended amount of daily physical activity and suggested that this population group faced additional barriers to participation24. That is, they encounter the same barriers to participation that are common to all children with a disability in combination with the additional barriers specific to living in a rural or remote area. This study, however, was a preliminary pilot study and as such this topic warrants further investigation. Therefore, an in-depth, qualitative investigation of physical activity participation in this population was undertaken. It was anticipated that this would assist with the provision of funding and development of support services. Further, it was thought that a thorough investigation of this topic area would inform parents, educators and health professionals in the design, development and delivery of strategies that would more effectively facilitate the physical activity of these children15,20. Given the limitations of the current literature, the aims of this study were to investigate rurally residing parents’ perceptions of physical activity participation of their child with a disability, and to explore the factors that serve as barriers or as facilitators to participation in physical activity.
Methods
Study design
This study was a qualitative investigation that utilised semi-structured focus group interviews to explore barriers and facilitators to physical activity participation by gathering detailed accounts from rurally residing parents in the state of New South Wales, Australia who had a child with a disability.
Participant recruitment
Participants were recruited to this study if they were rurally residing parents or carers of a child with a disability. Parents or carers were required to be 18 years of age or greater, and each child with a disability aged between 5 and 18 years. To ensure inclusivity, the authors did not define the nature of the parent or carer relationship to the child, nor the child’s disability. Instead, if the parent or carer self-identified as parenting a child with a disability the researchers deemed this sufficient to be included in the study. The parents or carers, and their child with a disability, needed to reside in a rural or remote area, in accordance with the Modified Monash Model (MMM) classification of rurality and remoteness25. Participants were required to be sufficiently proficient in the English language to participate in the focus groups. Participants were recruited through a local allied health private practice and a database from a large rural disability service. Parents or carers indicated their interest in participating in a focus group as part of a survey completed during a previous study24 or were informed about the study by staff members of a private practice who were not involved in the study. Potential participants were provided with information about the study and provided informed consent. Participants were then contacted by telephone by one member of the researcher team (TR), and focus group sessions were organised at a mutually convenient time. These were arranged so each participant could be involved in only one focus group interview.
Data collection
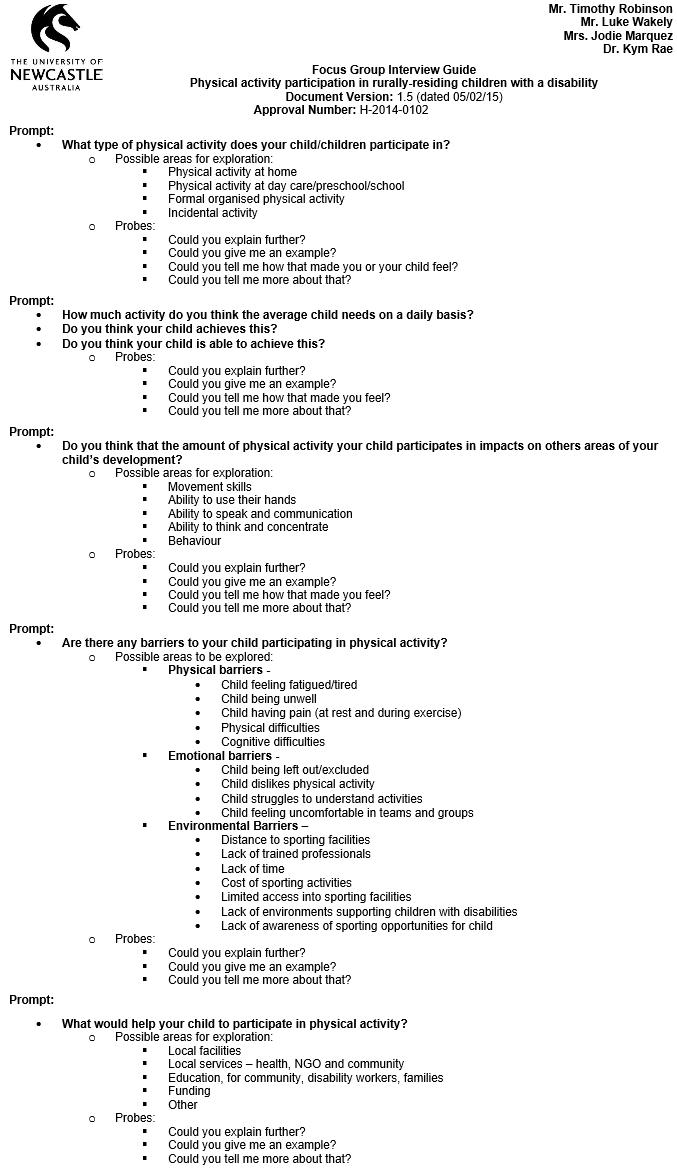
In 2015, one researcher (TR) conducted the focus group sessions at the University of Newcastle Department of Rural Health in rural New South Wales, Australia. At the commencement of each session, the researcher explained the purpose of the study, and collected demographic information relevant to the participants, their children with disabilities, and their family construct. Discussions within the sessions were facilitated with the aid of an interview guide (Appendix I) that was informed by data from a previously administered questionnaire24. Each focus group session was audiotaped and transcribed verbatim. Detailed field notes were recorded during and after the conclusion of each session in order to capture non-verbal information. To enhance the credibility and dependability of the findings of this study, a process diary and reflection diary were kept throughout the study period, providing an audit trail and allowing the researchers to reflect upon their own pre-conceptions during data collection and analysis.
Data analysis
Qualitative data were analysed inductively using qualitative content analysis 26,27. Transcripts and field notes were initially read to re-capture a sense of the whole meaning behind the participant’s comments. Subsequently, individual statements were re-read and assigned to categories. Categories were then reflected on and formulated into themes. Throughout this process, transcripts and field notes were reviewed, to ensure the emerging categorical and thematic ideas were reflected in the data and to search for any statements that may contradict the emerging analysis. To enhance credibility, findings were discussed with all members of the research team to allow various interpretations of the data to be considered, and to minimise individual biases or preconceptions from having undue influence on the outcome28. Data management, coding and analysis were facilitated using NVivo 10 software (QSR International; http://www.qsr.com). Participants were from rural areas with proportionately lower population densities than metropolitan areas, and were often parenting children with relatively rare conditions or diagnoses. For this reason, demographic data were reported in broad, descriptive categories in order to protect participants’ identities. Data collection continued until no new themes were emerging from the analysis.
Ethics approval
Ethics approval was granted by the University of Newcastle Human Research Ethics Committee (reference number H-2014-0102).
Results
Participants
There were 23 potential participants who indicated their interest in participating in the study. Of these, 20 were recruited via the survey of a previously reported study 24, and three from the rural private practice. Thirteen potential participants were unable to attend a focus group during the study period due to a lack of time (n=6), excessive travel distance (n=4) or needing to attend medical appointments (n=3).
Each participant was asked to attend one focus group. With the aim of providing the majority of potential participants with the opportunity to contribute, four focus group sessions were conducted at a variety of times over a period of 4 months. A total of ten participants attended a focus group session, the median number of participants in each focus group was 2.5 participants (interquartile range (IQR) 1.5–3.5 participants), and the median duration of each session was 65 minutes (IQR 63–76 minutes).
Participant characteristics
The median age of the participants in this study was 41.5 years (IQR 36–45 years), and the majority were female (n=7). The demographic information of the participants is presented in Table 1. One participant was the parent of two children with a disability, thus demographic data were collected for 11 children. The median age of the children was 11 years (IQR 8–16 years). Participants families resided in a range of rural areas within New South Wales, with 73% of participants residing in an MMM Category 3 area, and 27% from an MMM Category 5 area25. The nature of the children’s disabilities, as described by the parents, were primarily behavioural (n=7, 64%), neurological (n=5, 45%), or genetic (n=3, 27%), although these categories were not mutually exclusive. The effects of the disabilities on the children captured in this study were diverse, and a number of the participant’s children had been diagnosed with multiple disabilities. The characteristics of the participants’ children with a disability are presented in Table 2.
Table 1: Demographic data for parents (n=10)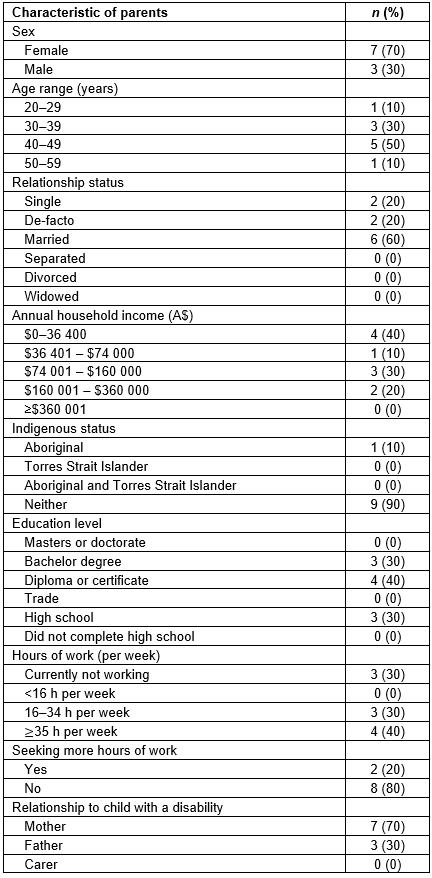
Table 2: Demographic data for children (n=11)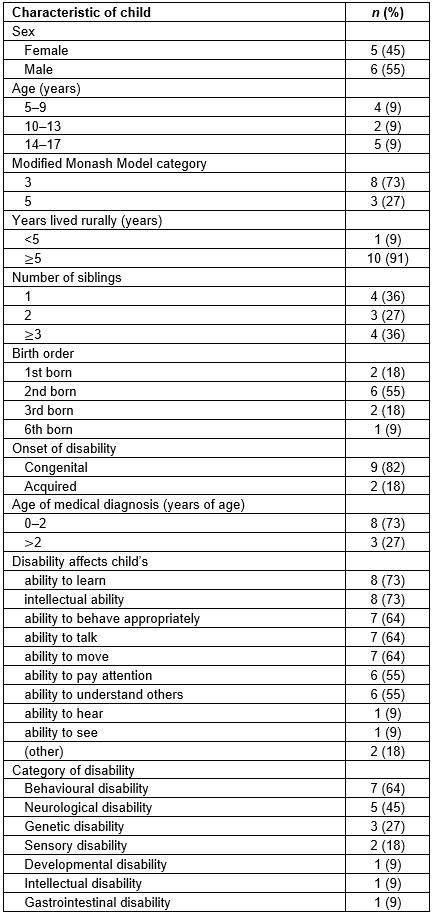
Thematic analysis
Analysis of focus group transcripts and field notes was performed with a strong orientation to the aims of this study: to explore physical activity participation of rurally residing children with a disability, barriers that limit participation, and factors that facilitate such participation. From the analysis, the overarching description surfaced: surviving, not thriving. Within this description, three themes emerged: (1) a parent’s predicament, (2) barriers to participation and (3) facilitators to participation. Within each of the themes, a number of subthemes appeared (Fig1).
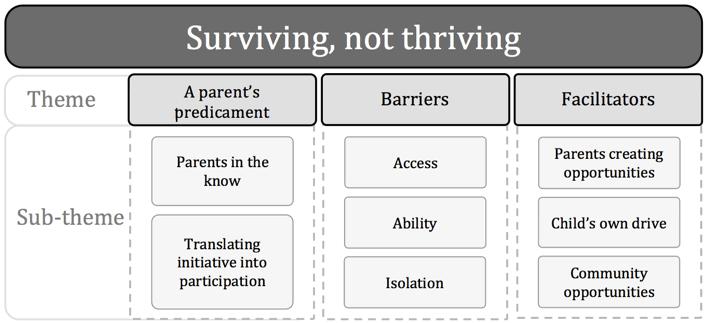 Figure 1: Thematic analysis of qualitative data.
Figure 1: Thematic analysis of qualitative data.
Surviving, not thriving: This described the participants’ overwhelming desperation to support the health of their child with a disability. It stemmed from a great frustration that their child did not have the same opportunity to grow, develop and prosper as their peers, which appeared to be magnified in rural areas. One mother of a 14-year-old girl with a disability described this desperation: ‘You’re down, and you don’t know where to turn, so our kids get pushed further and further back. Here, in rural country towns, it’s a thousand times worse’. Another participant, the mother of an 8-year-old boy with a disability, expressed her frustration: ‘It would be nice for [our children] to have every opportunity that every other child has. But we have to prove so much that our kids deserve it’.
Theme 1 – a parent’s predicament: This was a recurring notion throughout the focus groups. This theme described the perpetual struggle that parents of a child with a disability faced when attempting to facilitate their child’s participation in physical activity. In general, parents demonstrated knowledge and understanding of the health benefits of physical activity, yet struggled to convert this knowledge into greater participation for their child with a disability. This occurred for a range of reasons, which led to the emergence of two subthemes: (1) parents in the know and (2) translating initiative into participation.
Subtheme – parents in the know This subtheme describes the participants’ astute understanding of the health benefits derived from participating in sufficient amounts of physical activity. When asked about the amount of physical activity their children should be undertaking, participants were not only able to consistently provide accurate descriptions of this discussion point, but also to demonstrate an in-depth understanding of the broad range of health benefits that physical activity offers. Participants spoke about the ways physical activity specifically benefited their children. One mother of a 10-year-old girl with a disability described the benefits for her daughter:
[Physical activity] helps with her speech, her cognitive skills. You can tell the difference, and you can see her mood improve … it’s a huge benefit.
Another participant, the mother of a 16-year-old girl with a disability, explained further:
I believe [physical activity] is very beneficial. It clears their head […] helps them to develop, and even tuckers them out so they have a good sleep at night.
This level of understanding of the benefits of physical activity was commonly demonstrated by the participants across the focus group interviews.
Subtheme – translating initiative into participation This subtheme describes the struggle parents faced as they strived to enhance their child’s health, with particular regard to their participation in physical activity. Despite the participants’ knowledge of the recommendations and health benefits of physical activity, it was commonly reported that their children were seldom meeting the recommendations. One mother of a 17-year-old girl with a disability stated:
I know [my daughter] should do a hell of a lot more [physical activity], but I don’t have the capacity to facilitate it with everything else going on with her.
Another participant, the father of a 5-year-old boy with a disability, suggested that this struggle was more intense in rural areas:
I know there are physical activity guidelines, but I just don’t see how kids with a disability can meet those guidelines, especially in the country. It’s all too hard.
Unfortunately, parents’ knowledge and understanding failed to result in the children satisfying the physical activity recommendations, keeping them from reaping the subsequent health benefits. This fuelled deep discussion into the conditions that were inducing this phenomenon. As a result, the second main theme pertaining to physical activity participation emerged: barriers to participation.
Theme 2 – Barriers to participation: Discussions regarding this theme dominated the focus group sessions, forming a powerful motif spanning across the interviews. This theme described the range of factors that parents perceived to be preventing their child from receiving the health benefits associated with sufficient amounts of physical activity participation. While some of the barriers were reported to be common to all children with a disability, others were viewed as specific to the rural setting. Within this theme, three subthemes emerged: (1) access, (2) ability and (3) isolation.
Subtheme – access This describes the difficulties that participants faced when attempting to access appropriate physical activity programs, facilities and resources for their child. This was perceived as particularly difficult in rural areas, with participants most commonly reporting barriers pertaining to geographical distances, a paucity of trained professionals, limited programs appropriate for the child, time constraints and financial barriers. Participants often expressed how issues of accessibility affected their ability to support their child’s physical activity. One mother of an 11-year-old boy with a disability stated:
The only way we could access [a hydrotherapy pool] would be to drive for an hour and a half!
Another participant, the father of a 17-year-old boy with a disability, stated:
In a town like this, we don’t have the staff that could facilitate instructing kids with major disabilities to do activities.
Subtheme – ability This describes a child’s personal barriers to participating in physical activity. Participants often reported that the amount and type of physical activity that the children could engage in was heavily dependent on their child’s individual ability to move, sustain movement, socialise appropriately or process sensory information. Participants frequently illustrated how these issues restricted their child’s capacity to participate in physical activity. One father of a 14-year-old boy with a disability said:
My son’s slow, and he can’t keep up with his peers. In team sports, he just gets so overwhelmed by it all […] he simply can’t process quickly enough.
Another participant, the mother of a 9-year-old boy with a disability, stated:
[My son] doesn’t know how to get along with the other kids, and [he is] scared to participate because he gets tormented.
Subtheme – isolation This describes the social disconnection experienced by children with a disability. Participants frequently reported that negative attitudes toward disability had a profound influence on the child’s desire to participate in physical activities. One participant, the mother of an 8-year-old boy, poignantly expressed this:
When you’re the last one to be picked, it’s demoralising. My son goes, ‘Nobody wants me. I may as well go and sit under a tree and watch.’ So then [my son] thinks, ‘I’m not as good as them’. Then, ‘Why the hell was I born like this? Why didn’t you just let me die at birth?’
The perception of another participant, the father of a 14-year-old boy, suggested these feelings of isolation were influenced by a lack of understanding of disability in regional communities:
It’s obvious that in the country, people don’t think these kids are good enough to participate [in physical activity]. They think they’re sick, and therefore should be resting.
Overall, participants felt that their child’s potential to thrive was hampered by a multitude of barriers. However, despite the overwhelming barriers, participants did describe some factors that served to enable their child to participate in physical activity. From these discussions the third main theme emerged: facilitators to participation.
Theme 3 – Facilitators to participation: Discussion regarding this theme recurred across the focus groups. This theme described a range of factors that parents perceived to enable their child’s participation in physical activity. In general, participants expressed a sense of hope that their capacity to support their child’s health would improve. Within this theme, three subthemes emerged: (1) parents creating opportunities, (2) the child’s own drive and (3) community opportunities.
Subtheme – parents creating opportunities This describes the ‘facilitator’ role that parents assume in order to enhance their child’s participation in physical activity. Through positive support, the creation of opportunities and their desire for their child to thrive, parents reported that they personally enhanced their child’s engagement in physical activity. Participants commonly believed that they were the principal drivers of their child’s involvement in physical activity, which was viewed as particularly important in rural areas. For instance, one mother of an 11-year-old boy with a disability stated:
We have to facilitate his participation in physical activity. It’s primarily up to us, especially in the country.
This was reiterated by another participant, the father of a 17-year-old girl with a disability, who went on to describe his role as the ‘facilitator’ of his daughter’s physical activity participation:
It means encouraging [my daughter] to go [swimming], sussing out the facilities, getting the gear, transporting her there, and supervising her. All those things are down to us.
While the parents’ role as facilitators is significant it became clear that the children themselves were also an important facilitator to physical activity.
Subtheme – the child’s own drive This describes the positive impact the children had on their own participation in physical activity. The child’s motivation, enjoyment of the activity and personal desire to succeed were perceived to be particularly important facilitators of the children’s participation. One mother of an 8-year-old boy with a disability described:
… when they play tips you have to crawl like [my son]. It means their abilities are equal. It’s a real motivator for him, and now he likes playing.
This demonstrated how simply modifying an activity to suit her son’s capabilities resulted in increased enjoyment of physical activity.
Subtheme – community opportunities This describes the opportunities available within the community that enabled the children to participate in physical activity. Appropriately modified programs, inclusive activities and routine engagement in physical activity were perceived to be of particular benefit. One mother of a 14-year-old boy with a disability stated:
Our dance [studio] is the only one in town that adapts the dances so that all the children are involved. It’s great and they all like to do it too.
Another participant, the mother of a 9-year-old boy with a disability, expressed her appreciation of newly introduced physical initiatives at her son’s school:
[The school] has a walking time every morning, and he just loves the continuity of doing it all the time, and I love it too.
Participants commonly communicated how these group opportunities motivated their child’s enjoyment of participating in physical activity.
Participants generally perceived there was a range of factors facilitating their child’s participation in physical activity. However, parents felt the facilitating factors for participation were insufficient to overcome the multitude of barriers their children faced. As a result, the health status of this population may be suboptimal, potentially hampering their child’s potential to thrive.
Discussion
The account of emergent themes for participants clearly indicates that parents felt their children with disabilities faced a multitude of barriers to participating in physical activity, including difficulties related to accessing appropriate facilities, the children’s health issues limiting their ability to participate, and social isolation. Parents also reported that, despite this, several factors facilitated the physical activity participation of this population, including the creation of opportunities for physical activity by the children themselves, their parents and the wider community. Participants were committed to supporting the health of their children, yet struggled to facilitate sufficient amounts of physical activity for their children in order to attain the associated health benefits. This is concerning as this may have adverse effects on the health of children already dealing with pre-existing health issues.
Participants in this study provided detailed accounts of factors they perceived to be influencing their children’s participation in physical activity. Some of the barriers reported by participants were common to all children with a disability, regardless of rurality, such as social isolation, negative attitudes toward people with disability and barriers specific to the child15,17. Several of the barriers discussed in this study, however, were specific to all children living in a rural area, regardless of whether the child had a disability. These included difficulties in accessing appropriate facilities, programs and resources due to geographical distances; financial barriers22,23; and a lack of infrastructure for physical activity in rural communities8,21-23. This suggests that rurally residing children with disabilities face similar barriers to participation as all children with a disability, yet are also confronted by additional barriers that are specific to living rurally. Prior to this research, only one small exploratory study had investigated the barriers that limit the physical activity participation of rurally residing children with a disability24. The results of the current study expand on the findings presented by the previous study, providing a more in-depth understanding of the barriers that limit the physical participation of this population.
In the present study and the study by Wakely et al24, participants perceived that their children seldom met the Australian Physical Activity Guidelines recommendation. It is therefore possible that the functional development and health of these children may be hindered not only by their pre-existing health conditions, but also by insufficient participation in physical activity1-3. The present study also provides insight into the factors that served to facilitate the physical activity of rurally residing children with a disability. These included the motivation of both the children and their parents to create opportunities for the child through the development of new programs or through the appropriate modification of existing structures to enable individual participation. These factors were perceived to have a greater impact when guided by trained professionals, and when physical activity participation was a routine engagement.
A strength of this study was that the participants’ characteristics were diverse, representing a wide range of education levels, family constructs, employment and socioeconomic statuses as well as residence across different rural areas. Similarly, the characteristics of the children discussed in this study were heterogeneous, including a broad range of disabilities that impacted the children in a variety of ways. The use of focus groups in this study facilitated the collection of rich, vivid and experiential accounts of the experiences of participants. The semi-structured nature of the focus groups allowed the participants to discuss aspects of their experience important to them while allowing the interviewer to probe to explore emerging areas of experiential meaning.
Caring for a child with a disability is demanding, emotional and time-consuming29. This is one limitation of the study and was reflected in the difficulty of scheduling suitable times for participants to attend a focus group session, as well as the need to reschedule a number of planned sessions as the demands of caring for their child understandably took precedence over the interview. This meant not all potential participants were able to participate in the focus groups, which may have limited the breadth of data collected; however, given the demands of parents with children with disabilities, the researchers were unable to capture more participants within the timeframe of this study. As a result, the perceptions of those who attended a session may have differed to those who did not. In addition, it is possible that the ‘group-think’ phenomenon, which is inherent to all group discussions, could have occurred during the focus group interviews30. This was minimised by encouraging participants to express their own opinions and perspectives at the commencement of each session and throughout the focus group discussions. Another possible limitation of this study is that only one parent or carer per household participated in the focus group interviews. If more than one household member had been captured in this study, it is possible that different perspectives may have emerged. Similarly, interviews with other key stakeholders, such as the children themselves, disability services or service providers of physical activity programs may have produced alternative perspectives.
Future studies should explore the concepts found in this study across a range of rural and remote areas and should include various stakeholders. Research exploring the factors that facilitate physical activity participation in rural areas for these children would be beneficial to inform the development of more effective strategies supporting physical activity participation.
Conclusions
This study provides new insight into parents’ perceptions regarding the physical activity participation of rurally residing children with a disability. It is evident that these children face similar barriers to participation as all children with a disability, and are confronted by additional barriers specifically associated with living in a rural area. While this study found a range of factors that facilitated the physical activity participation of this population, participants still struggled to augment their child’s actual participation. This may have a range of adverse effects on the health of children already dealing with other significant health issues. Service providers working with this population should consider the findings of this study to develop and implement more effective strategies aimed at supporting the physical activity participation of these children. Furthermore, rural communities need to consider strategies to make physical activity more accessible and inclusive for children with a disability.
Acknowledgements
The authors thank the Northcott Society for their assistance in participant recruitment.
Appendix I: Focus group interview guide.