
Context
The 12-lead electrocardiogram (ECG) is an integral part of the diagnostic tools available for recognising a patient who is experiencing a ST-segment elevated myocardial infarction (STEMI). Consequently, a great emphasis is placed on the rapid acquisition and expert interpretation of the 12-lead ECG in order that the appropriate reperfusion management might be commenced in a timely manner to optimise patient outcomes by preventing further damage to the myocardium. This case report describes the presentation and management of a person experiencing a STEMI in a rural Australian hospital emergency department setting. The discussion highlights the importance of the frontline rural emergency clinicians’ vital role in recognising ECG abnormalities, rather than exclusive reliance on the powerful diagnostic analysis abilities of the modern 12-lead ECG machine and the role of early telemetric ECG transmissions for the initial management of a STEMI.
Issues
A woman aged 50 years with no known past medical history, but a familial history of ischaemic heart disease, woke up at 0400 h with shortness of breath, central chest pain and diaphoresis. The pain did not subside throughout the proceeding hours of the early morning. Choosing not to call an ambulance, the patient was transported by her husband to the nearest district hospital. The hospital was located in a small rural town in New South Wales, Australia, with a population of approximately 1200 people. Classified as a public acute group D hospital1, the small outer regional hospital has 11 aged care beds, 7 acute beds and a single bay emergency department.
Arriving at 0640 h the patient was met by the sole registered nurse on duty and immediately assessed in the emergency department. Despite walking in the front entrance, the patient was noted to be diaphoretic, short of breath, of a dusky pallor, with slow ambulation, anxious appearance, and she reported to the registered nurse that she felt like she was ‘having a heart attack’.
The patient was assigned an Australian Triage Scale category 2 and commenced on the New South Wales Chest Pain Pathway2 treatment protocol. During the primary clinical assessment a 12-lead ECG was promptly performed. The local process is to telemetrically transmit any ECG that the ECG machine identifies as meeting ‘STEMI criteria’ to the on-call cardiologist based at the local health district’s regional referral hospital. This first 12-lead ECG at 0650 h did not fit the diagnostic parameters of the ECG machine that would deem it as meeting STEMI criteria. However, the ECG did show some abnormal ST-segment elevation in leads V2, V3 and V4 (Fig1). The nurse, recognising this ECG anomaly, combined with the clinical picture of this patient, called the local on-call general practitioner, described the acute changes seen on the ECG and requested the general practitioner attend the hospital immediately.
Following the New South Wales Chest Pain Pathway2, the patient was given glyceryl trinitrate 600 µg sublingually and aspirin 300 mg orally. Due to the patient’s oxygen saturation decreasing to below 93%, oxygen at 6 L via simple face mask was applied. Within 10 minutes of the initial call, the general practitioner arrived. Simultaneously, another registered nurse due to start shift also attended the emergency department. Intravenous access was obtained and a second 12-lead ECG was performed. The first troponin via the iStat point of care testing, at 0715 h was 0.07 ng/mL.
The ECG machine interpreted the second trace to be meeting STEMI criteria (Fig2), thus it was transmitted to the on-call cardiologist. The patient remained conscious, morphine was administered intravenously, and clopidogrel 300 mg given. The cardiologist confirmed by telephone the STEMI diagnosis and, given the distance of more 300 km to the nearest percutaneous coronary intervention lab, gave the treating doctor advice to proceed with thrombolysis if not contraindicated.
Patient consent was obtained, no contraindications were identified and the patient was thrombolysed with tenectaplase 50 mg intravenously at 0723 h and commenced on enoxaparin. At 1 h post-thrombolysis, the patient’s ECG showed significant resolution (Fig3), her pain dissipated and her vital signs remained satisfactory. Later that day she was transferred by ambulance to Melbourne, Victoria, for definitive treatment via percutaneous coronary intervention. There, she was found to have a left anterior descending artery occlusion, which required stenting. The patient has since made a full recovery.
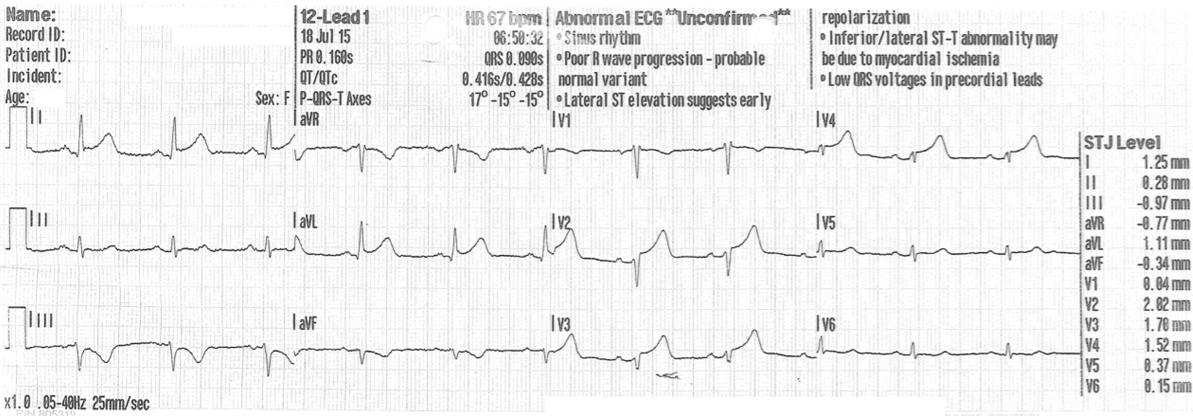 Figure 1: Initial 12-lead electrocardiogram showing evolving ST-segment elevation in leads V2, V3 and V4.
Figure 1: Initial 12-lead electrocardiogram showing evolving ST-segment elevation in leads V2, V3 and V4.
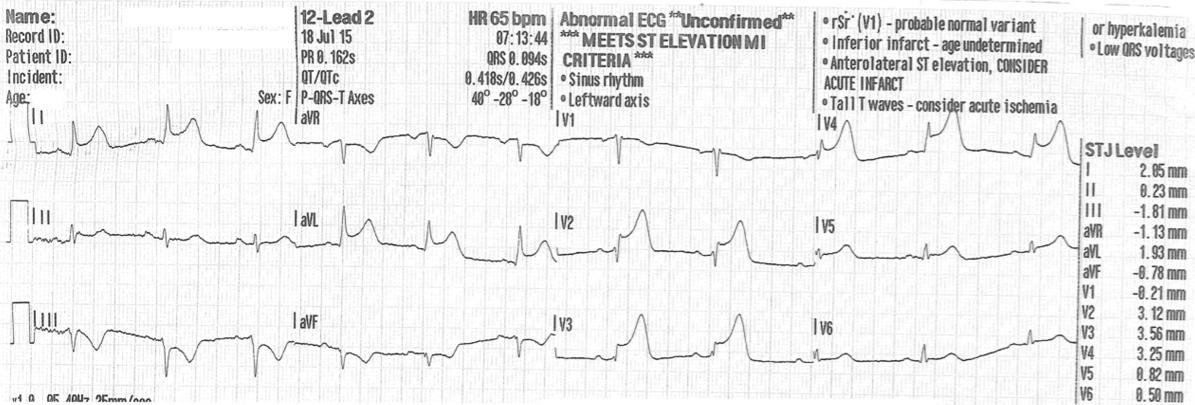 Figure 2: Significant ST-segment elevation in leads V2, V3, and V4 with reciprocal changes in leads I, III and aVL. ECG machine interpretation: ‘meets ST elevation MI criteria’.
Figure 2: Significant ST-segment elevation in leads V2, V3, and V4 with reciprocal changes in leads I, III and aVL. ECG machine interpretation: ‘meets ST elevation MI criteria’.
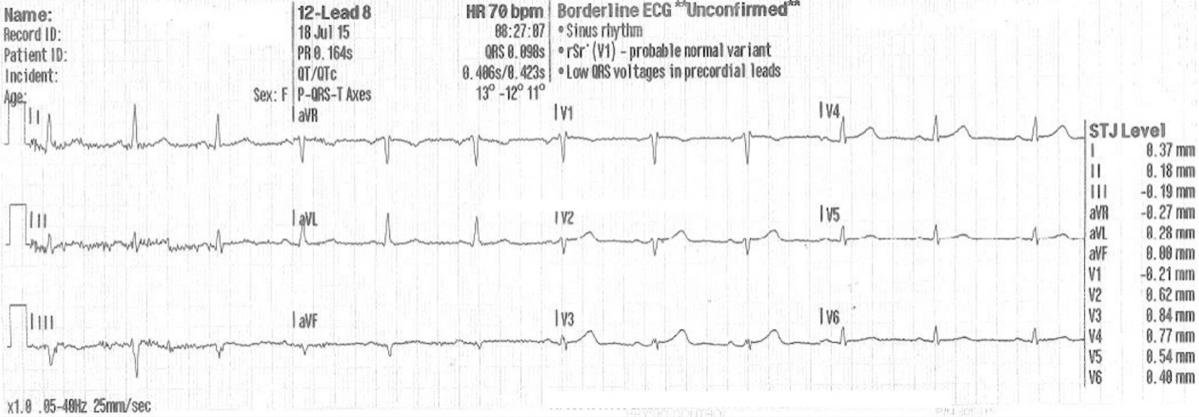 Figure 3: Resolution observed on the 12-lead electrocardiogram post-thrombolyis medication.
Figure 3: Resolution observed on the 12-lead electrocardiogram post-thrombolyis medication.
Ethics approval
This article did not require human research ethics committee approval. Informed written patient consent was obtained prior to the commencement of work on this article.
Lessons learned
This case report describes a fairly classic and somewhat routine management of a STEMI in the context of a rural Australian hospital, albeit with an interesting example of the treating clinician’s ability to detect ECG abnormalities versus reliance on the used technology’s diagnostic powers. This is an important point to consider in the context of health care and the ever-increasing utilisation of technology in diagnosing and treating illnesses, more so in the rural setting where specialist expertise is not always readily available. Advances in healthcare technology that have potential to improve patient outcomes should be welcomed but not without rigorous consideration of how this impacts on the clinician’s capacity and consequently the level of care provided to rural patients. This case report involves two important applications of technology adoption in the rural and remote health context, namely the telemetric ECG transmission and the diagnostically capable 12-lead ECG machine.
Telemetric ECG transmission
The phrase ‘time is muscle’ refers to the now well-established understanding of how the amount of time between symptoms of an acute myocardial infarction and the necessary treatment determines the extent of myocardial necrosis3,4. Consequently, expedient diagnosis and reperfusion treatment of a STEMI is key to improving patient outcomes5-7. Two important factors that contribute to a detrimental time delay in patients receiving treatment are time delays associated with performing an ECG and incorrect initial ECG interpretation6,7. The application of telemetry medicine in rural and remote contexts attempts to address these issues. Telemetry medicine allows patients to receive timely care despite the logistical challenges associated with remoteness and the often large geographical distances between the patient and the necessary expert clinician4. Much of the literature describing the application of telemetry technology for obtaining and transmitting the 12-lead ECGs to an advanced clinician for interpretation and treatment advice reports on the ambulance services’ use in an out-of-hospital setting4,8. Whilst this is not directly applicable to this case report, some of the important points raised are transferrable to rural or remote sites that employ a similar telemetric system. This telemetric process is made possible by the advanced technology of the ECG machine, which incorporates a diagnostic ability for identifying any 12-lead ECG that meets STEMI criteria and subsequently allows for the transmission of that ECG for formal diagnosis and advice of appropriate treatment. The second 12-lead ECG performed in this case report was identified by the ECG machine as meeting STEMI criteria and promptly transmitted to the on-call cardiologist. Evidently, this system enabled a STEMI patient presenting to a small rural hospital to receive timely thrombolysis, with the door-to-needle time being 43 minutes. Furthermore, this case supports existing literature that outlines how delays in treatment can be overcome by appropriate triage allocation so as to obtain an initial ECG in a timely manner and a competent ability to use the supplied technology in order to transmit the ECG data to the on-call cardiologist9.
ECG machine diagnostics
As already mentioned, the utilisation of in-built diagnostic software within the ECG machine is important when considering the role of remote medical assistance in the management of a STEMI case. According to the manufacturer, the in-built computer software program used by the ECG machine in this case has a high sensitivity at a high specificity for detecting all cardiac abnormalities within the 12-lead ECG. More specifically, the detection sensitivity for STEMI was measured at 89.4%. The software analyses the waveforms of each lead to determine if they fulfil the algorithm that interprets the trace as being a STEMI. Interestingly, the analysis software does not apply a direct or exclusive criteria of the universal definition of a STEMI, as described by Thygesen et al10:
… any new ST elevation at the J point in at least 2 contiguous leads of ≥2 mm (0.2 mV) in men or ≥1.5 mm (0.15 mV) in women in leads V2–V3 and/or of ≥1 mm (0.1 mV) in other contiguous chest leads or the limb leads’10,11
If this definition was applied as the sole diagnostic criteria for the ECG software to recognise a STEMI, then the first 12-lead trace would have indicated as such; that is, the STJ levels in leads V2, V3 and V4 are all greater than 1.5 mm (Fig1). However, as confirmed by the manufacturer, the 12-lead ECG analysis program’s interpretive algorithm applies additional filters such as an examination of the ST level in reference to the T-wave amplitude (ST/T ratio) and waveform, to improve STEMI detection accuracy.
Understandably, such advancements and improved accuracy in the science of computerised electrocardiology have delivered on their goal of saving time and improving patient care. However, as demonstrated in this clinical case, exclusive reliance on the ECG machine to diagnose a STEMI would have ostensibly led to a poor outcome for this patient. As seen in Figure 1, despite there being remarkable ST segment elevation in leads V2, V3 and V4, the machine did not deem it as meeting STEMI criteria. This is not a unique occurrence. Loch et al6 refer to such an event as the ‘evolving STEMI’, whereby the STEMI criteria are not met on the initial ECG but the development of a true STEMI ECG occurs whilst the patient is in the emergency department. This was identified as a significant factor that contributed to patients experiencing a prolonged door-to-needle time6. Understanding the pathophysiological process of coronary artery occlusion, as represented on the ECG, is an essential skill for frontline staff in the emergency department. The evolution of a STEMI, as characterised by ECG abnormalities, typically begins with raised T waves and culminates with ST segment elevation as total ischaemia occurs in the myocardium12. At different stages of a STEMI event, ECG changes such as T-wave inversion, ST segment depression and pathological Q waves may be seen12. Despite ECG interpretation being a vital skill in the emergency department, Wood et al13 found that up to 33% of interpretations contained significant errors. Recent research suggests that accurate ECG interpretations centre on perceptual scanning patterns that enable the prompt detection of abnormalities or possible perturbations on the ECG in focus13. Importantly, the registered nurse who made the initial assessment of the patient’s ECG had received prior training in ECG analysis and interpretation as part the New South Wales First Line Emergency Care Course14. Training that aims to develop advanced clinical nurses working in a rural emergency department context can evidently improve patient outcomes14.
Conclusion
Continued advancements in telemetry medicine that improve patient outcomes should be enthusiastically embraced. This case report has shown that competent utilisation of such technology, in this case the ECG machine, requires the clinician to be well trained in the technical use of the equipment, have a thorough understanding of how the technology interacts within the established clinical pathway and be ready to apply its use in a timely manner in order to prevent delays in treatment (ie reperfusion therapy). Furthermore, a reliance on the diagnostic ability of the modern ECG machine in the rural or remote context may potentially lead to poor patient outcomes. Advanced training in ECG interpretation and the maintaining of such competency should be standard among frontline staff in the rural or remote emergency department. Finally, the literature reviewed for the production of this case report predominantly focused on the ambulance service experience of using telehealth technology to transmit early ECGs and subsequently initiate the early management of STEMI patients. There seems to be a paucity in the literature of rural and remote hospitals’ experiences of utilising this technology. Thus, further research is needed to examine the efficacy of telemetric ECG analysis by remote cardiologists servicing rural and remote hospitals for the early management of STEMI patients.