
Introduction
Disability is a complex, dynamic and multidimensional concept that remains vehemently contested1. Historically, definitions of disability focused on the nature of the impairment and how bodies align with or deviate from a socially constructed norm, with people with disabilities being thought of as ‘tragic victims of failed biology’2. These medically perceived vulnerabilities were used as justification for the segregation and silencing of people with disabilities3. In the late 1970s, scholars and activists began speaking out about the negative implications of segregation on people with disabilities, proposing that the limitations and challenges associated with disability were not rooted within the body but rather within the sociopolitical reality of exclusion, stigma and discrimination4. While several social and political milestones have been achieved in recognising the rights of people with disabilities, current models of understanding leave little room for personal narratives to emerge, suggesting that, for many, their experiences continue to be denied, and their voices muted.
Research into the experiences that people with disabilities have with their environment has historically focused predominantly on physical barriers to access, with limited attention paid to ways in which place and space frame lived experience. Niemandt suggests that there is a growing ‘crisis of place’ (p. 2) that has been influenced by both globalisation and international economic recession5. This crisis of place has resulted in growing disparities between urban and rural populations. These inequities may be exacerbated for people with disabilities living in rural areas who experience loss both physically and emotionally through restricted access to place and space.
While inherently linked, the notions of place and space are distinctly different concepts. Gieryn suggests that place has physicality and refers to a unique, geographical location that has clear boundaries6. He proposes three defining features of place, which include ‘location, material form and meaningfulness’ (p. 465). This implies the formation of emotional, cultural and sentimental bonds resulting in feelings and experiences being associated with a specific geographical location. In contrast, space ‘is what place becomes when the unique gathering of things, meanings and values are sucked out’ (p. 466)6. It therefore follows that place and space highlight the micro- and macro-politics of rurality7.
Research into the ways in which space and place influence lived experience has been limited, and has failed to adequately consider the ways in which environmental constraints and social demands impact on the physical and emotional spaces in which individuals live and function8. Current understandings of disability are further influenced by the fact that many people with disabilities continue to be excluded from participating in research projects about them and their experiences. Most research into the lived experience of disability relies on proxy accounts9,10. Where research has included the voices of people with disabilities, individuals who live in geographically remote areas, those with cognitive and communicative impairments, and those who are illiterate or who do not speak English have often been excluded11. The silencing of these voices has resulted in a limited understanding of the life experiences of people with disabilities, and has impacted on the development of policies and practices designed to meet their needs.
Thus, while it is well recognised that people with disabilities have been systematically muted through discriminatory and exclusionary practices7, research that focuses on first-person accounts without taking context and location into account may lead to a misrepresentation of individuals. Place and context enable power, and while places have the potential to bring people together, they may also represent the location of ‘loneliness, segregation, social control, withdrawal, detachment, isolation, fear and mental illness’ (p. 466)6. For people with disabilities living in rural areas, these experiences, coupled with food insecurity, a lack of service provision, barriers to accessible services, poor infrastructure, stigma, and social exclusion1, further silence their voices and create challenges to inclusion into mainstream activities. In addition, the spread of communicable diseases, together with high burden of chronic illnesses, increases the vulnerability of persons with disabilities in rural areas. Communicable diseases such as HIV and tuberculosis are known to disproportionately affect vulnerable groups12, with risk factors for infection including poverty13, lack of formal education14 and poor access to information15. Factors such as sexual abuse16, limited access to health care17, gender inequality18 and gender-based violence19 create a deepened sense of isolation and strengthen the relationship between disability and disempowerment. These experiences further marginalise and isolate people with disabilities from mainstream community life, and, consequently, poverty and social exclusion are seen to increase the severity of impairments10.
South Africa provides a unique setting in which to study the ways in which context influences the narratives of lived experience. South Africa’s history of legalised racism and segregation resulted in the notion of space being contested. Apartheid created geographical and psychological division among the country’s inhabitants, producing structures that prioritised certain voices over others. Today, 26 years post-democracy, South Africa is still dealing with the challenges imposed by inequality, deprivation and extreme spacialisation of poverty, making it one of the most unequal countries in the world20. Niemandt suggests that South African politics about land, space and place are not only political and economical in nature, but also deeply emotional, and that the spaces and places where people live may be reflective of sacrifice, hardship, suppression, disenfranchisement and loss5.
For people with disabilities, particularly in rural settings, the combination of impairment, poverty and contextual deprivation renders them vulnerable to a variety of forms of discrimination, perpetuating a sense of uncertainty in their lives, and impacting their ability to access basic services and make autonomous life choices21. In acknowledgement of the vulnerability of people with disabilities, many societies have adopted and instituted policies aimed to ensure that basic human rights are upheld. These include the World Programme of Action Concerning People with Disabilities22, the United Nations Rules on the Equalization of Opportunities for Persons with Disabilities23 and the United Nations Convention on the Rights of Persons with Disabilities24. The South African Government has established a Ministry on Women, Children and People with Disabilities, and has also adopted additional policies for the protection of its citizens. These include the White Paper on an Integrated National Disability Strategy25, the African Charter on Human and People’s Rights26, the Patient Rights Charter27 and the Batho Pele Principles28. The South African Constitution29 is considered to be one of the most inclusive constitutions in the world, with specific attention paid to protecting the rights of vulnerable populations. The Constitution is complemented by the South African Bill of Rights30, which mandates the right to non-discrimination, education, information, safety and housing. Furthermore, the National Health Plan for South Africa31 undertakes to provide free health care to people with disabilities. The Department of Social Development offers several support grants. These are issued monthly on the basis of a means test and being able to produce a South African identity document, and include disability grants, child support grants and old-age pensions32.
Narrative inquiry offers a valuable means of gaining insight into the plurality of lived experience that cannot be arrived at through other means33. Clandinin et al assert that people construct stories in order to make sense of their experiences, to integrate disparate roles, values and skills, and in this way to organise the past, present and future into a meaningful pattern34. This is supported by Fox, who claims that narrative inquiry has the potential to illuminate the ways in which intractable traces of the past are felt on people’s bodies and perceived through the moral fabric of their social relations35. Important in narrative inquiry is the way in which physical and emotional spaces influence the structure and composition of narratives, with Hermans (p. 259) claiming that ‘space is not simply outside the self but also within the self’36. This concept is supported by Clandinin et al who highlight the importance of understanding the metaphoric space within which stories are constructed and told34. These include the physical and topographical boundaries, social conditions and the temporal orientation that frame narratives. This concept is reflective of Niemandt’s notion of ‘storied places’ (p. 4)5. While some research has been conducted on the ways in which urban places and spaces are constructed6, there is limited research into the way in which rural places are created and this impacts on our understanding of the ways in which narratives are told within these contexts. This is particularly true for people with disabilities.
The data presented in the article were collected as part of a bigger study exploring the narrative articulations of lived experience among adults with disabilities living in a rural area37. This article aims to provide a detailed account of the ways in which physical and emotional spaces influence the ability of adults with disabilities to make sense of their lived experiences, by posing the question, ‘How do place and space influence the lived experience of adults with disabilities living in a rural area?’ In order to answer this question, the following objectives were identified:
- Explore the physical and emotional dimensions of exclusion as described by adults with disabilities living in a rural area.
- Explore the physical and emotional dimensions of inclusion as described by adults with disabilities living in a rural area.
Methods
Setting
Data were collected in 12 rural villages in the Nkomazi East Municipality, located within the Southern Lowveld area of the Mpumalanga Province, approximately 560 km east of the capital, Pretoria. The Nkomazi East Municipality continues to be one of the poorest municipalities in the Mpumalanga Province38. Access to education and health care is limited, with a high burden of communicable and non-communicable diseases. This is compounded by high rates of unemployment, malnutrition, dehydration and poor supply of basic service provision38. Currently, no published data exists on the numbers of people with disabilities residing in the Nkomazi East Municipality.
Research design and considerations for working cross-culturally and cross-linguistically
A qualitative design underpinned by the principles of narrative inquiry, participant observation and researcher reflexivity was employed. During data collection, the author demonstrated a sustained presence in the field and, in so doing, observed the participants in a variety of everyday contexts. Narrative interviews were conducted in SiSwati (one of South Africa’s 11 official languages) by a research mediator. The mediator and researcher had worked together previously both in a clinical and research capacity and both the researcher and mediator were known to the community. Being a local resident with a physical disability as well as the community-based rehabilitation worker, the research mediator had a shared history with a number of the participants. The research mediator took on the role of cultural and linguistic broker, assisting the researcher in identifying potential participants, accompanying the researcher to their homes, navigating the process of informed consent, conducting the interviews, and providing insight into elicited narratives and observed events.
Participants
Thirty participants comprising 15 males and 15 females (Table 1) with a variety of impairments were sampled using snowball sampling. All participants were over the age of 18 years. No measures were put in place to control for factors such as length of time since onset of disability, cause of disability and gender. Similarly, no criteria were put in place to ensure that only rich data were elicited, heeding the caution by Frank (1995) that, for some people, chaos, exclusion and uncertainty may only be voiced in the silences that speech cannot penetrate39. For this reason, participants were visited several times during the process of data collection and a triangulation of methods was employed to ensure accurate representations of participants’ experiences. Of the 30 participants, seven had congenital disabilities, while 23 had acquired disabilities, ranging from 5 months to 43 years from time of onset. Given the nature of the participants’ impairments and that several participants had received minimal if any formal education and were therefore not competent readers, consent was obtained verbally, following the Declaration of Helsinki guidelines40. Participants were approached by the research mediator and provided with written and verbal information about the nature of the study. All participants were given time to think about whether they wanted to participate or not and were contacted telephonically 2–3 days later by the research mediator, in order to determine whether they wanted to participate or not. While cognisance was taken of the imperative not to rely on proxy accounts, where participants presented with cognitive or linguistic impairments, family members were also consulted prior to interviewing the participant.
At the time of data collection only one participant’s home had direct access to a tarred road, with participants living an average distance of 5.1 km from the closest tarred road. Twelve participants had access to clean running water on their property, with the remaining participants having to travel up to 6.9 km to collect water. Sixteen participants had access to electricity in their homes (one home had an illegal connection), while the remaining 14 participants relied on gas, fire and candles for cooking, warmth and light. Twenty-one participants were recipients of disability grants and one participant received an old-age pension. The remaining eight participants relied on their families and the community to support them financially.
Table 1: Summary of participant demographics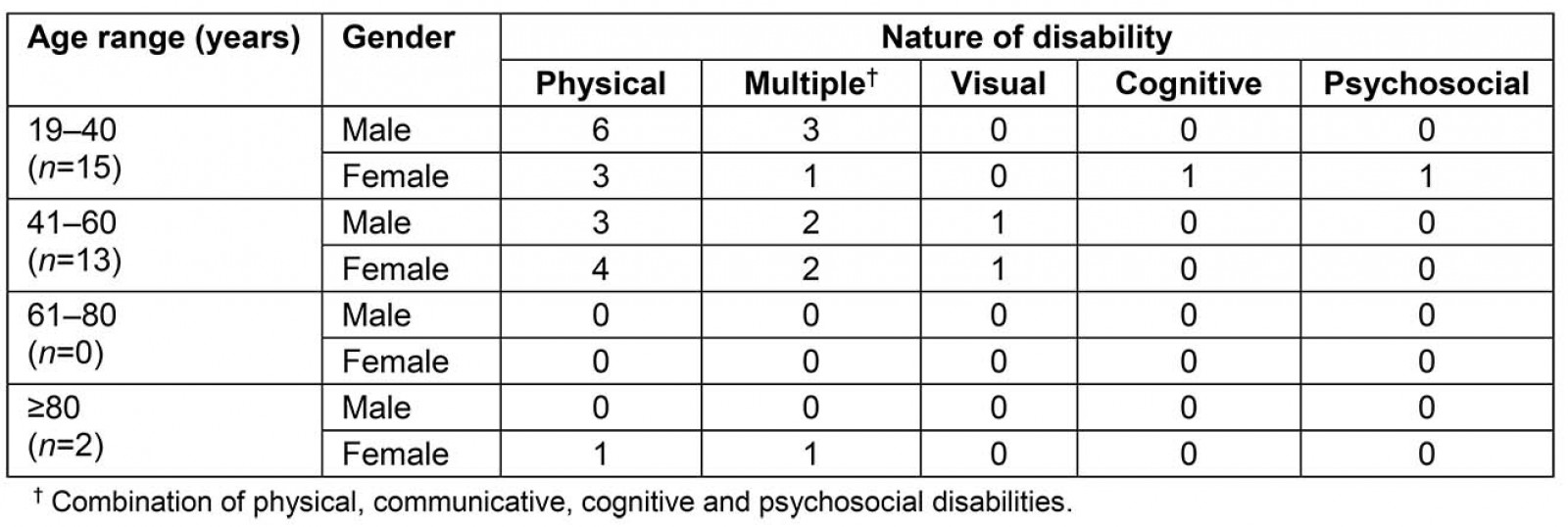
Methods of data collection and analysis
Data collection took place over a period of 3 months. Participants were visited in their homes over a period of 2–3 hours on a minimum of two occasions and were asked to ‘tell their story’. Based on the themes that emerged, Flick’s approach to guiding questions was adopted41.
Narratives were transcribed and translated from SiSwati into English by a SiSwati first-language research assistant and back-translated by a second research assistant in order to ensure accuracy. Data were analysed following Braun and Clarke’s guidelines on inductive thematic analysis42.
Table 2: Generative and guiding questions used during data collection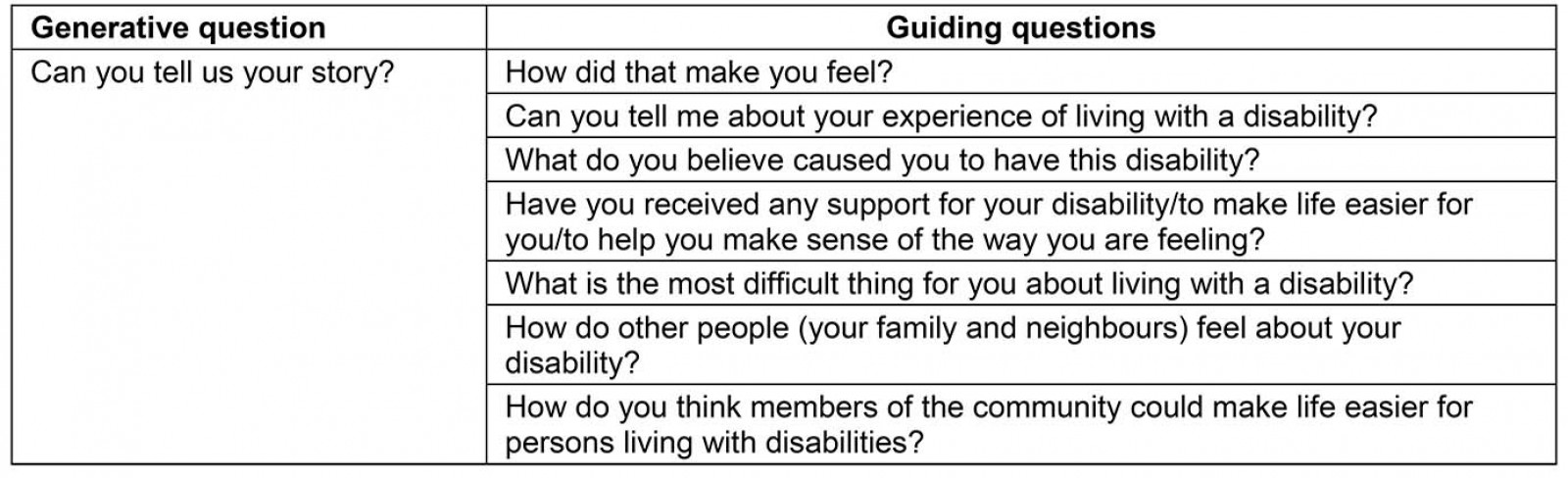
Rigour
Rigour was ensured by employing a local research mediator who was familiar to a number of the participants, sustaining a prolonged presence in the field prior to, during and post-data collection; triangulating data collection methods; member checking of transcribed interviews, using audit trails in the form of reflective journalling and audio-recorded reflective conversations between the researcher and research mediator; as well as using verbatim quotes in documenting the findings.
Ethics approval
Ethics clearance was granted through the University of the Witwatersrand Non-Medical Ethics Committee (protocol number H090612). Data collection, analysis and write-up of findings were done in accordance with the standards stipulated in the Declaration of Helsinki40, as well as by taking into account local and international recommendations for conducting research with vulnerable populations43,44.
Results
The findings of this study provide insight into the ways in which space and place influence the narratives that adults with disabilities tell about their experiences.
During the process of data collection, several homes experienced the death of a family member. At times, interviews were set up, but days later when we arrived, the participant had died, while in other instances locations of interviews had to be changed because of a death in the family. As a researcher, I found myself questioning how I could continue with data collection amid such pain and suffering. Despite these circumstances, the participants appeared keen to be interviewed and suggested changes in times and/or venues. Thus, data collection took place under the imminent presence of death, which, although only spoken about incidentally, seemed to contextualise the narratives. Based on this, the notion of uncertainty emerged as a prominent theme. Furthermore, given that most of the participants presented with acquired disabilities, the notions of place, time and the body appeared to be unreliable constructs, implying that both bodies and lives may be changed without warning, and thus life trajectories could neither be anticipated nor relied upon. Within this context, two main findings emerged: the spatial dimensions of exclusion and the construction of ‘safe places’ and their impact on inclusion.
Spatial dimensions of exclusion
While exclusion on the basis of disability is not a new phenomenon10 the findings of this study highlight the overlap between physical, social and emotional arenas of exclusion, and how the concepts of time and place, and space, are woven into reflections on exclusion. These emerged as a complex web of physical and socioemotional barriers to participation, and included the effects of reduced mobility, as well as limited access to assistive devices, support, education, health care and social support grants.
Exclusion on the basis of physical mobility: Several participants with physical disabilities were confined to their homes. While these participants were not necessarily hidden from the community, the nature of their disability, together with limited access to assistive devices, meant that they were restricted to their homes and isolated from mainstream society. An example of this was seen with participant 1, a man aged 50 years with a physical disability who had been confined to his home for more than 40 years. As a result of his disability, as well as the distance from the local hospital, he did not have any assistive devices, and consequently was confined to a bed in a small room, and dependent on his sister for help with activities of daily living. The physical confines in which he lived appeared to restrict the emotional space in which the narrative was told:
It is difficult for me, especially when I am thinking that I am not walking, not going outside, always in the house like a dead person. These difficulties in life can make you unhappy, sometimes thinking that you must rather die. (participant 1)
Several other participants appeared to share this sentiment:
Life is really difficult. In the day I am always alone. I look around me and there is no one, looking at my neighbours but there is no one, just quiet, then I urinate there in wheelchair, until they come back and help me, washing me and my clothes. (participant 18)
To move from the sun to shade is really difficult. I had to wait until the others were back from school, just sitting there while the sun was burning me. (participant 4)
These quotes highlight the ways in which the embodied experiences of physical and spatial constraints are transformed into psychosocial forms of exclusion.
Health care, education and social services as sectors of exclusion: Government facilities, specifically the social welfare offices where disability grants are applied for and issued, were commonly discussed as physical spaces in which people with disabilities did not have access to adequate information and where they were excluded from mainstream society. Examples of this type of exclusion were portrayed as follows:
I don’t receive the grant. I go to the doctors, they fill the forms, but when I go to the social work offices to check, they say ‘sorry, it failed’. They don’t explain to me what is happening. (participant 7)
The problem is that I applied several times for the grant but every time it failed. I don’t know why. (participant 20)
I [was] delayed in getting my ID book. I don’t know why. Those that applied after me got it before me. The problem is if you are disabled you are nothing. You are the last thing to think of. Even ID people don’t follow up because they think, woooo, here is a disabled person and he will get a grant and I can’t. (participant 2)
These examples highlight how exclusion occurs within physical locations such as the social welfare offices, and how the emotional effects of this type of exclusion impact on an individual’s socioeconomic stability.
The education sector was another physical arena where many participants experienced exclusion. An example of this is seen where a female aged 44 years with paraplegia as a result of polio during childhood, recalled how her lack of a wheelchair initially prevented her from attending school. She recalled how her mother approached the school principal requesting that she be admitted, but the principal responded, saying:
No, this is a school for normal children, not for disabilities. She can’t come to this school because she doesn’t have a wheelchair. (participant 30)
In a similar example, a female aged 28 years with a congenital absence of her upper and lower limbs reported:
I couldn’t go to school because I didn’t have a wheelchair, so my sisters were teaching me when they came home from school. (participant 25)
In these examples, exclusion resulted in a spatial restriction for participants, creating a situation where they were unable to leave their homes or to engage in mainstream activities. Several other participants commented on their experiences within mainstream schools, suggesting that even where they were able to access mainstream schooling, physical barriers and discrimination limited their access to education:
But that first day at school was so bad for me. Some were laughing, some were pointing. At the classroom, there was a step, so I had to leave the wheelchair and crawl to the desk, and the children were laughing like it was a show. (participant 30)
To be at school with normal people was stressful. I was always sitting at the back and eating alone, feeling afraid, like I was not a human being. (participant 21)
In the classroom it was bad because when the teacher was asking questions and I failed to know the answer, he would just say ‘you cripple! I taught you yesterday but now you forgot’. Then the students would just laugh at me and I felt embarrassed. (participant 22)
An additional area of exclusion, impacted by poor accessibility and the effects of poverty, was the healthcare sector. This was especially evident among women who had borne children. Their narratives revealed barriers associated with physical access, as well as barriers created as a result of nurses’ perceptions of women with disabilities:
I had a problem going for check-ups because my mother was dead and she was the one assisting me to go to the hospital. (participant 6)
So I was always asking my neighbour to help me, to push me to the clinic for check-ups because there is no public transport from my home … but oh! It was embarrassing for me to be pregnant. I was afraid of myself, the way I was, and the nurses were asking ‘who did this to you?’ Like as a disabled person I was not supposed to sleep with a man, like I looked like an animal. (participant 3)
These narratives highlight the relationship between physical barriers and societal stigma that contravene the individual’s rights to reproductive health, resulting in healthcare encounters being fraught with uncertainty and anxiety.
Exclusion from the employment sector: The employment sector was revealed to be an area where people with disabilities felt significantly excluded. The desire to work was linked to culturally assigned gender roles, the importance of being productive and being able to contribute financially to the family’s wellbeing, and to identity development more broadly. However, all the participants felt that their disabilities prevented them from being viewed as potential employees. Desire to work is evident where participant 2 said ‘I wish I could work, even if I can be a general worker, it doesn’t matter as long as I maintain my family’ and participant 4 said ‘It’s just that I want to work. That is all.’ Similarly, participant 14 said ‘Life is not ok. It is painful for me now because I’m not working. My wife wakes up in the morning and leaves me behind with the child. That is not the way [it] should be.’
Significantly, several participants felt that they were discriminated against as a result of their disabilities:
So as you know that here in South Africa we are oppressed a lot. They said we are supposed to work in all offices, but they don’t appoint us. (participant 2)
Other people work, but a person like me being disabled, where can I work? (participant 9)
Furthermore, it emerged that both family members and community members did not believe that people with disabilities should strive towards financial independence but that they should be content to live off a disability grant:
When I’m looking for a job other people ask why because I am getting disability grant. (participant 14)
So I was trying to sell fruit on the side of the road but then other people came and were fighting with me, saying why am I selling fruit when I am disabled? I must get the grant and leave the work for them. (participant 20)
These quotes highlight how, in the context of poverty, challenges associated with unemployment are magnified, especially for people with disabilities, and how this sense of exclusion impacts not only on financial security but also on resilience and sense of identity.
Exclusion from participation in socio-cultural activities: Exclusion was also reported in terms of participation in socially and culturally acceptable events. An example of this is seen, where participant 30 described her hesitance to attend weddings within her community:
People in the community, they look at you like you are an animal, laughing and pointing like it is the nonsense thing, like a show. So when you are going to a party, like a wedding, all of them are looking at you. So me, I am not comfortable going there. (participant 30)
The most common form of emotional exclusion was through the loss of friendships as a result of disability. While this did not appear to be a significant factor for all participants, a number reported that they had either lost friends or that the nature of friendships had changed after onset of the disability:
It is no longer the same like the past because they ignore me, saying ‘what can they do with a person that can’t walk, not active anymore?’ Nothing. (participant 4)
Since my friends heard that I am injured they never came to visit me. (participant 6)
My friends are still coming to visit me, but not all of them. Even though they visit me, it is not the same as before. (participant 10)
These experiences of altered friendships and social relations appeared to create a sense of isolation and marginalisation amongst participants. This is evident in participant 1’s statement that ‘Most of the time I am alone’, and for participant 6 ‘I am used to being alone now.’
These descriptions provide insight into the dimensions of exclusion that serve as boundaries within which people with disabilities make sense of their experiences and the spaces and places within which they create and tell stories about their lives. Thus, despite renewed calls locally and internationally for inclusion, people with disabilities continue to face a complex combination of physical barriers and stigma, affecting equitable access to participation.
‘Safe places’ and the physical and emotional dimensions of inclusion
Despite the restrictions imposed by the spatial and emotional dimensions of exclusion, the fact that all participants, regardless of the nature of their disability or their life experiences, were able to tell their stories implies that they were able to create a spatial and emotional context in which they felt safe.
Churches and informal disability support groups within the communities appeared to be the primary physical locations where participants felt safe to live out their stories. Examples of inclusion and the experience of equality were evident as follows:
At church they treat me well, even giving me a chance to be master of ceremonies. (participant 7)
For me, I am feeling comfortable when I go to church. But even at church, some people are making me to feel depressed, saying ‘shame, shame’, but others are just saying ‘hello, how are you’ treating me like a normal person. (participant 30)
In several villages, informal disability centres had been started up by people with disabilities. Evidence of a sense of inclusion and group identity emerged in several narratives:
At home, most of the people don’t want to stay with a disabled person, but here we sit together and share ideas. They put ideas in my mind and teach me new skills and encourage me to live the life that I want. (participant 4)
This group built a lot of things in our minds, and now we are able to help other people like us. Although we have different challenges, we all benefit. … There was a time when it was difficult for me to attend the centre because there was no one to push my wheelchair. Then one woman lent me her grandson to push me every day. Since then I am coping and enjoying life. So now, each of us who are getting the pension pays R20 [approximately A$1.70] per month to pay for food, and we are even able to pay the one who is cooking. (participant 3)
Participant 3’s statement demonstrates how physical places have the ability to contribute towards individual freedom, and in so doing create a sense of group identity and belonging. This suggests that the physical settings and the emotional context in which the interviews took place created a place for detailed personal accounts to emerge. While some participants revealed relatively little about themselves, most of the participants provided insight into their challenging life circumstances and experiences of trauma in a pragmatic way. This can be attributed to the fact that the participants were interviewed in their home language and that the research mediator was known to them and shared similar life experiences.
Conclusion
This article highlights the ways in which spatial boundaries, the places in which people live, as well as the physical location of the interviews, impact on the narrative content shared. The stories in this study were woven into wider narratives about gender roles and expectations, the communities’ perceptions of disability and of people with disabilities, and the uncertainty of living in a community ravaged by the effects of communicable diseases and high mortality rates. The many contextual challenges contributed to a sense of vulnerability among participants, giving rise to unpredictability of bodies, experiences and life trajectories. These vulnerabilities and challenges highlighted obstacles to access, which are problematic for all people living in rural areas. These challenges are, however, magnified for people with disabilities whose access to education, information, health care and employment is further hampered by physical and/or cognitive-communicative impairments.
Narrative inquiry proved to be a useful means to gaining insight into the complexities of lived experience, with the findings giving rise to questions regarding how people living in rural communities search for and assign meaning to their worlds. Importantly, the focus on space and place in narrative construction provided detailed insight into the ways in which physical locality creates barriers to access, and how these barriers are particularly problematic for people with disabilities. In addition, stigma and discrimination against people with disabilities were revealed to negatively impact upon their sense of belonging. In contrast, physical and emotional safe places were shown to be empowering and transformative.
The findings of exclusion and discrimination call for social activism and for communities to confront the anxieties, silences, prejudices and injustices that exist in healthcare consultations and community engagements. This would involve mobilising the local community and other stakeholders to fight for the rights of people with disabilities and to draw attention to the power inequalities that hinder equitable service provision45. Campbell (p. 2) further emphasises that social activism in the form of supportive social networks may be seen to promote the likelihood of community mobilisation through the provision of ‘safe social spaces’45. This highlights the need for a more detailed exploration into the existing networks of informal support within rural communities in terms of what makes these networks possible and what the drivers for success entail.
While the findings from this study may be useful in providing a sociocultural understanding of the ways in which spatial confines influence lived experience, the limitations of collecting data cross-linguistically and analysing it from an etic perspective cannot be ignored. While there were commonalities between the mediator and the participants’ life experiences that led to the emergence of detailed and personal stories, the notion of mediator bias needs to be considered. Although these restrictions cannot be denied, they do need to be weighed against the importance of providing participants with an opportunity to tell their stories in their language of choice. The value of this approach was captured in the phrase used by five of the participants where they described their friendship with the research mediator by saying, wati bonke buntima bami, which in English can be translated to ‘She knows me in my darkest places.’ This phrase implies a sense of shared knowledge that could not have been forged through an interview with an unfamiliar person or in a language in which the participant did not feel confident or competent. This finding aligns with both Temple and Young’s (2004) and Squire’s (2008) support for cross-cultural research in order to avoid narrowing the research field and thereby continuing to disadvantage previously neglected cultural-linguistic groups46,47.
Recommendations for future research include a more detailed exploration into the networks of informal support that exist within rural communities, with a focus on how these relate to both space and place. Furthermore, research could focus on the nature of information available to people with disabilities in rural communities and the nature of information they find most useful. This information may guide the training of social and healthcare professionals as well as educators and in so doing improve the life experiences of people with disabilities.