

Introduction
Oral health is an important component of general health and quality of life, with dental caries impacting on a person's ability to eat, speak or socialise1. Dental caries or tooth decay is an acquired chronic infective disease process caused by the acidic by-products of bacteria inhabiting organised dental plaque or oral bio-film that, if left undisturbed, can dissolve or demineralise the enamel surfaces of the teeth. Despite marked improvements in the oral health of children in many developed countries in the last 20-30 years, evidence suggests that a small proportion of children in such nations carry the highest dental caries burden2. In Australia, Indigenous children are known to be among this disadvantaged group3.
The mid-north region of South Australia contains a high proportion of the state's Indigenous population, with more than 5000 Aboriginal people residing in the regional center of Port Augusta or surrounding areas4 (Fig 1). The Indigenous population in this area is increasing, despite an apparent decrease in the overall Port Augusta population in the last decade5. Port Augusta's Indigenous community represents approximately 23 cultural groups from different areas of Australia. Although most Indigenous people residing in the Port Augusta region are permanent, a small proportion are transient6.
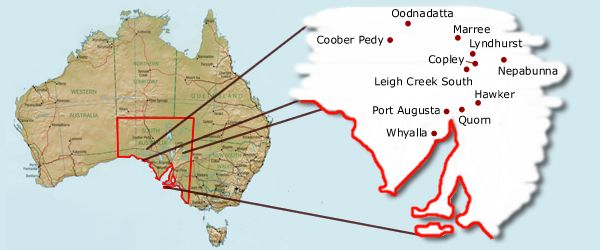
Figure 1: Map of the study area.
Aboriginal communities in South Australia's mid-north region have identified dental health as one of their top health priorities7. In response to this, and following recommendations from the Aboriginal Health Organisation of South Australia that a regular dental service be made available to Aboriginal people in all areas8, the Pika Wiya Health Service Inc. (Pika Wiya), based in Port Augusta, together with the South Australian Dental Service (SADS), the South Australian Centre for Rural and Remote Health and the University of Adelaide School of Dentistry formed an Oral Health Program based in Pika Wiya's Port Augusta clinic, which began operating in 2001. Pika Wiya Health Service is incorporated under the Aboriginal Services Division of the Department of Human Services. Pika Wiya Health Service Inc (http://www.pikawiya.com.au) has close affiliations with the South Australian Aboriginal Health Council and is represented on the National Aboriginal Community Controlled Health Organisations board by the Chief Executive Officer. The dental service is an Aboriginal-only service. A dentist provided oral health care to adults 2 days per week, and was jointly paid by SADS and Pika Wiya. A dental therapist and dental assistant were employed to provide services to children, with the salaries of both being met by SADS. The Port Augusta School Dental Service is a public service funded by SADS. The dental therapist provided clinical services one day per week for the first year of the service, increasing to 2 days per week after demand and utilisation of the service was demonstrated. A transport service was made available to clients, transporting children and parents to and from home or school for their dental appointments and to specialist dental services, if necessary.
The purpose of this article is to compare the socio-demographic and oral health characteristics of children attending for care at the Pika Wiya Health Service Dental Clinic with those of their counterparts (Indigenous and non-Indigenous) attending the general Port Augusta School Dental Service (SDS) from 2001 to 2006. Following evidence from the literature, the hypothesis was that children attending for care at Pika Wiya would have higher levels of dental caries experience in the primary and permanent dentition than their counterparts seeking care through the general SDS.
Methods
Data were obtained from SADS, which routinely-collects socio-demographic and dental information from patients seen through their system. Examinations were conducted by SADS-employed dental professionals. Examiners were not calibrated, but received similar training and used standardised procedures.
A full enumeration of children attending for care at Pika Wiya and the Port Augusta SDS from March 2001 to March 2006 was included. When children received more than one examination during this observation period, information derived from the first examination only was examined. For children who presented at both the Pika Wiya Health Service Dental Clinic and the Port Augusta SDS (n = 32), data from the place of first contact only were included. Surface level tooth data were captured using the EXACT? treatment charting and management information system. Ethical approval for the study was obtained from the University of Adelaide (23 November 2005), the Aboriginal Health Council of South Australia (5 December 2005) and the SADS Executive Committee (8 December 2006).
Socio-economic status index
The Socio-Economic Indices For Areas (SEIFA) were used to determine socio-economic status. The indices use data derived from the 2001 Census of Population and Housing, and employ a range of measures to rank areas based on their relative social and economic wellbeing9. For purposes of this report, the SEIFA Index of Disadvantage (category 2) was used. This index takes into account variables relating to income, educational attainment, unemployment and dwellings without motor vehicles. In particular it focuses on low-income earners, relatively lower educational attainment and high unemployment.
Oral health index
The dmft (sum of decayed, missing and filled teeth in the deciduous dentition) and DMFT (sum of decayed, missing and filled teeth in the permanent dentition) indices were used to assess oral health outcomes. The indices are a cumulative measure of caries experience that express the amount of successfully treated disease (filled teeth), unsuccessfully treated disease (extracted teeth) and untreated disease (decayed teeth). They include a record of the presence/absence of all teeth including presumptive cause of tooth loss. Both measures were used for children aged 6-10 years because in such age groups children have a mixed dentition (both primary and permanent teeth are present). Permanent teeth usually begin erupting at the age of 5 or 6 years.
Caries prevalence (dmft/DMFT>0) and severity (mean dmft/DMFT) were calculated, as well as the Significant Caries Index (SiC) and Significant Caries Index 10 (SiC 10). The SiC is the mean dmft/DMFT of the one-third of the sample with the highest caries score, while the SiC is the mean dmft/DMFT of the one-tenth of the sample with the highest caries score.
Data were analysed using SPSS 13.0 (SPSS Inc; Chicago, IL, USA) and levels of statistical significance, as per convention, were set at p<0.05. The chi-square and Fisher's exact tests were used to measure statistically significant differences between proportions, and Student's t-test when the dependent variable was continuous.
Results
In the 5 year observation period, 760 children were seen at the Pika Wiya Dental Service while over 6800 were seen at the Port Augusta SDS (Table 1). A higher proportion of pre-school children attended for care at Pika Wiya, while proportionally more children aged ≥11 years attended for care at the Port Augusta SDS. More females attended for care at Pika Wiya. Over 85% of children seen at Pika Wiya were Indigenous, compared with 7% at the Port Augusta SDS. Almost all children (99%) attending for care at Pika Wiya lived in the most disadvantaged areas, according to the SEIFA scale.
Table 1: Socio-demographic characteristics of children attending Pika Wiya Dental Service and the Port Augusta School Dental Service, 2001-2006
Children attending for care at Pika Wiya had 3 times the mean number of decayed deciduous and permanent teeth of their counterparts attending the Port Augusta SDS (Table 2). Over three-quarters of the children attending for care at Pika Wiya aged 10 years or less had dental caries experience in the primary dentition, compared with just over 50% of children attending for care at the Port Augusta SDS. Children attending for dental care at Pika Wiya aged 10 years or less had 1.8 times the mean dmft, 1.4 times the SiC and 1.4 times the Sic 10 of their counterparts attending for care at Port Augusta SDS. Over half the children aged ≥6 years who attended Pika Wiya for dental care had caries experience in the permanent dentition, compared with 38% of their Port Augusta SDS-attending counterparts. Children aged ≥6 years who attended Pika Wiya for dental care had 1.9 times the mean DMFT, 1.8 times the SiC and 1.6 times the SiC 10 of their similarly-aged Port Augusta SDS-attending counterparts.
Table 2: Oral health characteristics of children attending Pika Wiya Dental Service and the Port Augusta School Dental Service, 2001-2006
Discussion
Our findings show that children attending for care at the Pika Wiya Dental Service between 2001 and 2006 were more likely to be pre-school aged, female, Indigenous and living in a socially disadvantaged area, in comparison with children attending the Port Augusta SDS. Pika Wiya-attending children had 1.5-3 times the dental caries prevalence and severity in both the primary and permanent dentition of children attending for care at the Port Augusta SDS. A report outlining this information has been disseminated throughout the Port Augusta Aboriginal community.
It is interesting that proportionally more children who were pre-school-aged or female attended for dental care at the Pika Wiya Health Service than the Port Augusta SDS. Staff of the Pika Wiya Oral Health Program actively promoted the service through child care centers, kindergartens, play groups and through immunisation workers. This was to encourage early enrolment in the program, thus enabling timely identification of disease and to implement the appropriate preventative and conservative treatment services. Anecdotal evidence suggests that young children would present for care or be 'recruited' in the waiting room while parents were attending Pika Wiya for other services. In contrast, proportionally less children aged ≥11 years attended for care at Pika Wiya Health Service. Reports from staff involved in the Pika Wiya service suggested that older children were more difficult to locate because of increased independence, and that they may refuse to attend for dental care despite transport being available. There is no obvious reason why more girls than boys would have attended for dental care at the Pika Wiya Dental Health Service.
Our clinical dental findings, while alarming, are supported by literature that suggest that Indigenous children - or those seeking care in Indigenous-organised health services - are more disadvantaged in terms of dental caries experience than non-Indigenous children, or those seeking care in traditional SDS settings10. There are a number of reasons why such disparities might have been observed: dietary choices11, social determinants12, access to services13 and life-course factors14. The higher prevalence of dental caries experience among children attending the Pika Wiya Dental Service indicates the need for culturally-appropriate dental service provision as part of broader oral health programs, with some children having long-standing lesions that had been left untreated for a considerable period because dental service provision was not accessed. It should be noted that Indigeneity in and of itself is not a risk factor or cause for poor oral health, being a biological and social construct only. It is hoped that through the Pika Wiya Dental Service's dedication to increasing Aboriginal child dental service provision participation rates, and health education and health promotion strategies within the local community, the proportion of untreated decay might diminish. This, in turn, would address a priority highlighted in Australia's National Oral Health Plan1.
There was a small proportion of children who accessed dental services at Pika Wiya with 'unspecified' Indigenous status. Numerous logistical constraints faced at the beginning of the dental program's inception at Pika Wiya meant that data collection and use of the computerised data base were not always maintained with a high level of rigour, meaning Indigenous status might have gone unchecked. It is reasonable to assume that children with their Indigenous status unspecified at Pika Wiya were likely to be Indigenous, however, since the Pika Wiya Health Service Dental Program had funding and services to support Aboriginal clients only. Non-Aboriginal children would not be turned away from Pika Wiya, but would be encouraged to access care through the SADS mainstream clinic. The number of non-Aboriginal children receiving dental care at the Pika Wiya Health Service over the five-year period of data collection was very few, that is less than 2%. In contrast, children with their Indigenous status not specified in the main stream SDS in Port Augusta were more than likely to be non-Indigenous.
Limitations of this study
The nature of the study was cross-sectional, thus precluding the ability to draw inferences about causal relationships. The reliance on precise recording of patient information also created opportunities for accuracy loss, for example, the omission of Indigenous status recording. This may have led, in turn, to an underestimation of the true number of Indigenous children seen. An additional cause of bias was that the observers of dental status were not calibrated. It is possible, although unlikely, that staff expected Indigenous children to have more dental problems and so were more careful to look for problems and scored them to demonstrate more problems.
Conclusion
Our findings have highlighted the different characteristics of children attending for dental care between two services located in the same postcode area: Pika Wiya Health Service Oral Health Program and Port Augusta School Dental Clinic. The higher levels of disease experience, untreated disease and social disadvantage of children attending Pika Wiya provides further evidence for the need to address the health inequalities of Indigenous children living in the mid-north region of South Australia. While the Pika Wiya Oral Health Program is attempting to address some of these needs, a much broader focus to address the social and health inequalities will be required to improve the oral health characteristics of this population.
Acknowledgements
The authors are grateful for the assistance of SADS, the staff of the Pika Wiya Oral Health Program, and the Pika Wiya Oral Health Program stakeholders. Funding to establish the Pika Wiya Oral Health Program was gratefully received from the NHMRC. The authors received no funding and have no vested interest in the EXACT? treatment and management information system.
References
1. National Advisory Committee on Oral Health. Healthy mouths healthy lives: Australia's National Oral Health Plan 2004-2013. Adelaide, SA: South Australian Department of Health, 2004.
2. Harris R, Nicoll AD, Adair PM, Pine CM. Risk factors for dental caries in young children: a systematic review of the literature. Community Dental Health 2004; 21: 71-85.
3. Commonwealth Department of Health and Ageing. National Aboriginal and Torres Strait Islander oral health workshop report. Canberra, ACT: Commonwealth Department of Health and Ageing, 2003.
4. Parker EJ, Misan G, Richards LC, Russell A. Planning and implementing the first stage of an oral health program for the Pika Wiya Health Service Incorporated Aboriginal community in Port Augusta, South Australia. Rural Remote Health 5: 254. (Online) 2005. Available: www.rrh.org.au (Accessed 5 March 2007).
5. Australian Bureau of Statistics. Census of population and housing 2001; basic community profile. Canberra, ACT: Australian Government, 2001.
6. Spencer Gulf Rural Health School. Working with Aboriginal people in rural and remote South Australia; a cultural awareness handbook for people working in the health professions. Whyalla, SA: Spencer Gulf Rural Health School, 2001; 28.
7. Aboriginal Health Council of South Australia. South Australian Aboriginal health regional plans: the first step..... 1998. Dulwich, SA: Aboriginal Health Council of South Australia, 1998.
8. Chryssides H. A report of the dental survey and treatment of Australian Aborigines in the north-west communities of South Australia, Port Augusta (and surrounds), Ceduna, Yalata (and surrounds). Adelaide, SA: Aboriginal Health Organisation of South Australia, 1986.
9. Australian Bureau of Statistics. Census of population and housing - socio-economic indexes for areas, Australia. Canberra, ACT: Australian Government, 2001.
10. Endean C, Roberts-Thomson K, Wooley S. Anangu oral health: the status of the Indigenous population of the Anangu Pitjantjatjara lands. Australian Journal of Rural Health 2004; 12: 99-103.
11. Gracey M. Historical, cultural, political, and social influences on dietary patterns and nutrition in Australian Aboriginal children. American Journal of Clinical Nutrition 2000; 72: 1361-1367.
12. Altman J. The economic and social context of Indigenous health. In: N Thomson (Ed.). The health of Indigenous Australians. Melbourne, VIC: Oxford University Press, 2003: 25-43.
13. Kelaher M, Dunt D, Taylor-Thomson D, Harrison N, O'Donoghue L, Barnes T et al. Improving access to medicines among clients of remote area Aboriginal and Torres Strait Islander Health Services. Australian and New Zealand Journal of Public Health 2006; 30: 177-183.
14. Bedos C, Brodeur JM, Arpin S, Nicolau B. Dental caries experience: a two-generation study. Journal of Dental Research 2005; 84: 931-936.
Original Research
Oral health comparisons between children attending an Aboriginal health service and a Government school dental service in a regional location
AFFILIATIONS
1, 2 University of Adelaide School of Dentistry, Frome Road, South Australia
PUBLISHED
2 May 2007 Volume 7 Issue 2
HISTORY
RECEIVED: 18 July 2006
REVISED: 21 December 2006
ACCEPTED: 2 May 2007
CITATION
Parker E, Jamieson L. Oral health comparisons between children attending an Aboriginal health service and a Government school dental service in a regional location. Rural and Remote Health 2007; 7: 625. https://doi.org/10.22605/RRH625
AUTHOR CONTRIBUTIONS
© Eleanor Parker, Lisa Jamieson 2007 A licence to publish this material has been given to ARHEN, arhen.org.au
Abstract
Introduction: Indigenous children in Australia have higher dental caries levels than their non-Indigenous counterparts. Indigenous communities in South Australia's mid-north region have identified dental health as one of their top health priorities. In response to this, an oral health program based at the Pika Wiya Health Service in Port Augusta was established, with a dentist providing care for adults, and a dental therapist providing care for children, 2 days per week each. The purpose of this article is to compare the socio-demographic and oral health characteristics of children attending for care at the Pika Wiya Health Service Dental Clinic with those of their counterparts attending the general Port Augusta School Dental Service (SDS). Both Indigenous and non-Indigenous children were included.
Methods: Data were obtained from the South Australian Dental Service (SADS), which routinely collects socio-demographic and dental information from patients seen through their system. Examinations were conducted by SADS-employed dental professionals. A full enumeration of children attending for care at Pika Wiya and the Port Augusta SDS from March 2001 to March 2006 was included. Surface level tooth data was captured using the EXACT? treatment charting and management information system. The Socio-Economic Indices For Areas (SEIFA) were used to determine socio-economic status, and the dmft (sum of decayed, missing and filled teeth in the deciduous dentition) and DMFT (sum of decayed, missing and filled teeth in the permanent dentition) indices were used to assess oral health outcomes. Both measures were used for children aged 6-10 years because in such age groups children have a mixed dentition (both primary and permanent teeth are present). Caries prevalence (dmft/DMFT>0) and severity (mean dmft/DMFT) were calculated, as well as the Significant Caries Index (SiC) and Significant Caries Index 10 (SiC 10). The SiC is the mean dmft/DMFT of the one-third of the sample with the highest caries score; while the SiC 10 is the mean dmft/DMFT of the one-tenth of the sample with the highest caries score.
Results: In the 5 year observation period, 760 children were seen at the Pika Wiya Dental Service while over 6800 were seen at the Port Augusta SDS. A higher proportion of pre-school children attended for care at Pika Wiya, while proportionally more children aged ≥11 years attended for care at the Port Augusta SDS. More females attended for care at Pika Wiya. Almost all children (99%) attending for care at Pika Wiya lived in the most disadvantaged areas according to the SEIFA scale. Children attending for care at Pika Wiya had three-times the mean number of decayed deciduous and permanent teeth than their counterparts attending the Port Augusta SDS. Over 75% of children attending for care at Pika Wiya aged 10 years or less had dental caries experience in the primary dentition compared with just over 50% of children attending for care at the Port Augusta SDS. Children attending for dental care at Pika Wiya aged 10 years or less had 1.8 times the mean dmft, 1.4 times the SiC and 1.4 times the Sic 10 of their counterparts attending for care at Port Augusta SDS. Over half the children aged ≥6 years who attended Pika Wiya for dental care had caries experience in the permanent dentition compared with 38% of their Port Augusta SDS-attending counterparts. Children aged ≥6 years who attended Pika Wiya for dental care had 1.9 times the mean DMFT, 1.8 times the SiC and 1.6 times the SiC 10 of their similarly-aged Port Augusta SDS-attending counterparts.
Conclusions: Children attending for care at the Pika Wiya Dental Service were more likely to be pre-school-aged, female, Indigenous and living in a socially disadvantaged area, in comparison with children attending the Port Augusta SDS. Pika Wiya-attending children had 1.5-3 times the dental caries prevalence and severity in both the primary and permanent dentition of children attending for care at the Port Augusta SDS. The higher levels of dental caries experience, untreated disease and social disadvantage of children attending Pika Wiya provides further evidence for the need to address the health inequalities for Aboriginal children living in South Australia's mid-north region. While the Pika Wiya Oral Health Program is attempting to address some of these needs, a much broader focus to address the social and health inequalities will be required to improve the oral health characteristics of this population. It is hoped that through the Pika Wiya Dental Service's dedication to increasing Aboriginal child dental service participation rates, the proportion of untreated decay will diminish.
Key words: children, dental caries, Indigenous, Indigenous-controlled health centre.