



Introduction
The novel coronavirus disease officially named COVID-19 on 11 February 20201, and declared a pandemic on 11 March in the same year2,3, continues to have a devastating impact on the world. The numbers of confirmed cases and deaths have soared globally, with every country in the world being affected4. This has led different countries to adopt various approaches, such as instituting full or partial lockdowns, declaring a state of emergency, and enforcing the use of facemasks and other non-pharmaceutical approaches to curb the spread of the disease; yet it continues to spread5,6. Studies have shown higher infection rates in urban centres of the world; however, rural areas are also affected by the pandemic and similar control measures adopted to curb the spread in urban areas are enforced in rural areas, which are regulated by the same government7,8. Furthermore, irrespective of the lower infection rates in rural areas6, the disease impact of the pandemic might be more catastrophic in rural areas because of their less developed healthcare systems, and the economic fallout of the pandemic might be more severe on rural dwellers given that they typically have lower incomes9-11.
Contrary to expert views that predicted that Africa would be the hardest hit because of the weak health infrastructures and care services12-14, the continent has recorded fewer cases than expected. It has been speculated that Africa’s young population and warmer climate have contributed to the slow transmission rate; however, there is no strong scientific evidence to support such claims15. Although, Africa might be coming into the pandemic a little slower than other regions, current trends suggest this will probably change16. These low transmission and lower death rates from the pandemic have led to disbelief about the existence of the disease in Nigeria. Many Nigerians are spreading a conspiracy theory, propagated by religious leaders, that records of death are just a ploy by Nigerian politicians to steal public funds and shut down religion in the country17,18; this mistrust has been found to affect precautionary behaviours5.
To avert the looming danger, Sub-Saharan African countries worked together with the World Health Organization (WHO), non-government organisations, and other healthcare institutions to produce a framework for reducing the spread of the disease13. In Nigeria, the federal government closed off the country and cancelled flights, shut down schools, restricted public gatherings, and partnered with state governments and other institutions to create awareness, promote the practice of good hygiene, and provide relief support to indigent citizens19. However, despite these measures, speculation about the existence of the virus still remains, resulting in distrust of the measures instituted to control the spread in Nigeria. Also, the buzzing media certainly provided enough data for the speculations and conspiracy theories20.
This distrust has led to vaccine hesitancy in the country. Many Nigerians are refusing to accept the vaccine because of several myths surrounding the vaccines21. Inspired by religious teachings, some Nigerians believe that the vaccine is a ploy by the government to give them the biblical mark of the beast ‘666’, while others believe it will cause impotency and death within 3 years of being injected with the vaccine21. Experts believe that the hesitancy will prevent Nigeria from achieving herd immunity22; thus, there is a need to continue using non-pharmaceutical measures to protect the people. Debunking the myths surrounding COVID-19 and vaccines, discouraging blatant neglect of set preventive measures, and generally controlling the narrative became imperative for moderating the consequent community spread. This was necessary because knowledge about a disease influences peoples’ attitudes towards protection against the disease23,24. This explains the policy response, and the government and health systems’ intervention.
The policy response and government intervention to curb the infection and reduce the socioeconomic impact have not failed to attract scholarly attention. For example, Onyeji25 and Oginni et al26 commented about how the government swiftly closed international airports, public and private schools, universities, stores, and markets, and suspended public gatherings in major cities. Obiezu27 reported that the lockdown was eased after 5 weeks because of the economic pressure on citizens, while Unah28 and Ayeni29 observed that the Nigerian government in partnership with private organisations provided support in the form of food relief to households to cushion the economic impact of the pandemic. However, most of these interventions were targeted at cities while the infection pattern had transcended from imported cases in the major cities to rural community transmission with potential for an outbreak in rural communities30; yet rural community transmission has attracted very little scholarly attention.
This study is topical because a large percentage (48.84%) of Nigeria’s population, as in many Sub-Saharan African countries, live in rural communities31, and traditional rulers, who are part of the local authorities and are closest to rural people, have a prominent role to play in curbing community infections32. This is in accordance with role theory, which is based on the observation that people’s behaviour is context-specific; that is, people’s behaviour is defined by their social position and expectations from the social structure within their environment33. Evidently upheld by role theory is that human behaviour is guided by status and role expectations; humans are continually acting out the socially defined categories ascribed to them by social structure34. Thus, rural people, who are also particularly affected by the impacts of COVID-19 because they are poorer, have less access to the already poor healthcare system, and have the highest proportion of older persons in Nigeria, have high expectations of the efforts and roles of their traditional rulers in addressing their challenges. Therefore, there is a need for a study on the experience of traditional rulers in the fight against COVID-19 in rural Nigeria because this will reveal challenging areas in the effort to protect people from COVID-19. This is salient because traditional rulers are significant stakeholders in community engagement activities, given their work with groups such as community health workers, local government officials, and other health experts to protect rural people, especially during disease outbreaks35,36.
Conceptual framework
The concepts of traditional governance and polity dualism are combined to explain how traditional rulers act as a link between rural people and the government at different levels. The traditional rulers’ governance and authority hinge on the culture of the people, which validates them37,38; hence, chiefs, kings, headmen, queen mothers, or councils of elders steer the affairs of the community, making and enforcing rules, and delivering services39.
Polity dualism is the existence of two distinct political and legal systems designed for and applied to the same people40. This institutional setup has been described by scholars as ‘mixed government’41, ‘twilight institutions’42, or ‘hybrid political orders’43. It is practised in many Sub-Saharan Africa communities where traditional rulers are recognised as custodians of culture and tradition32,44 and believed to have supernatural authority from the gods. The authority, legitimacy, and presence of these traditional rulers make them uniquely suited for reaching rural people45.
Thus, rural people in Nigeria are under the legal and political systems of the Nigerian government at federal, state, and local levels, and under the traditional governance of the traditional leaders. For effective governance, therefore, different levels of government work in collaboration with these traditional rulers to reach rural people and get feedback through them (Fig1). Studies have shown the effectiveness of this collaboration in past epidemics such as Ebola35, and have equally highlighted its growing importance in the fight against COVID-19 in Ghana46 and Zimbabwe47. International institutions and agencies have similarly recognised the unique role of traditional rulers in protecting rural people against pandemics48; their authority and influence are invaluable assets that could help the government in rural Nigeria where limited access to factual data causes an ‘infodemic’47.
Figure 1 shows the flow of governance and illustrates polity dualism. It shows how federal, state, and local executive governments steer the affairs of rural people, given that their policies and laws affect them. It also shows how the executive governments, the legislators in both federal houses and the state house govern rural people through traditional rulers. Traditional rulers give feedback to the government on policies and social issues while also exercising authority, settling disputes, and making rules according to the local traditions and culture. To illustrate, the governments at federal, state, and local levels make COVID-19-related decisions such as lockdowns, compulsory use of facemasks, and physical distancing, and the traditional rulers are responsible for enforcing the set rules and decisions in their rural communities. Again, the government executives and the legislators representing the constituencies also send relief materials to rural people through the traditional rulers and if there is a rural outbreak of a disease, the traditional rulers are charged with reporting to the government at different levels.
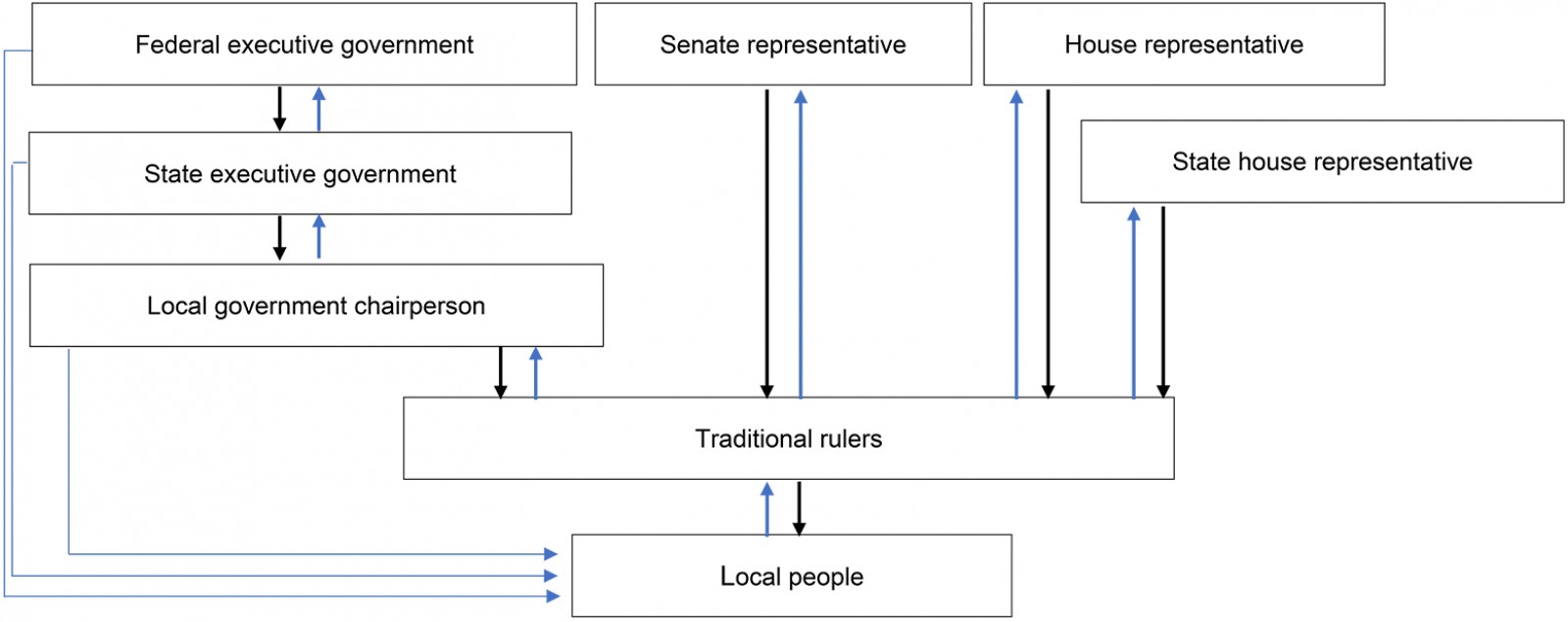 Figure 1: Flow of rural governance.
Figure 1: Flow of rural governance.
Methods
Study area
The study was conducted in Enugu state, south-eastern Nigeria. As of 30 January 2021, Enugu had the highest number of COVID-19 cases in eastern Nigeria, more than 130018. The estimated population of Enugu state is 4 411 100, covering an area of 7625 km249. Its inhabitants are predominantly Igbos (the ethnic group) and Christian. Enugu has more than 300 traditional rulers who constantly meet with their respective local government chairmen, and occasionally with the state government, to discuss matters that directly affect rural people50. Many of the traditional rulers reside with the people in the rural communities, and some of them live in the cities and constantly visit their communities. This unique relationship makes the state particularly suited for a study on the relevance of traditional rulers and their roles in fighting the spread of COVID-19.
Sampling procedure/data collection
Purposive sampling was used to choose Enugu state for the study partly because of the number of cases, but also because the researchers were residents of the state at the time and movement was still limited, making it difficult to reach traditional leaders in other south-eastern states. Snowball sampling was used to select the research participants because the participants are authority figures, and the easiest way to get them to participate in the study was through referral by their colleagues. The researchers sent letters to five traditional rulers requesting interviews and assistance with the recruitment of other traditional rulers. The first two traditional rulers to respond helped identify other participants who were either comfortable with a phone interview or available and lived close to the city capital or Nsukka metropolis. Out of 28 traditional rulers contacted, eight male participants aged 58–77 years agreed and were sampled for the study. Given the qualitative nature of this study, the sample size (n=8) was expected to provide enough data to reach theoretical saturation51. The rationale for the gender is that traditional rulers in the state are all men. The age range is 58–77 years because traditional rulers in the state are primarily advanced in age; wisdom is attributed to old age in the people’s tradition. Two of the participants had no formal education, three had primary education, two had secondary education, while only one identified having studied to university level.
In-depth interviews were used to collect data from the participants. The interview guide was designed and revised several times by the researchers and some of their research colleagues before it was finally used for data collection. Influenced by the role theory, questions in the interviews focused on how the communities protect themselves, the roles played by traditional rulers in protecting the communities, and the challenges faced in carrying out these roles. The participants gave their verbal consent before the interview commenced. The researchers also assured them of anonymity and confidentiality, and explained their rights to withdraw from the study or to retract any or all of their contributions should they choose to do so, before publication of the study. The participants were not incentivised; this was to ensure reliability of the data. Because of the COVID-19 pandemic, the research participants were provided with the option of a phone interview or an in-person interview. During in-person interviews, recommended infection preventive measures were meticulously observed. The interviews lasted from 30 to 45 minutes and were audio-recorded after the research participants had consented to it.
Data analysis
The collected data were translated from Igbo into English and transcribed as verbatim as possible, using the parallel transcription framework described by Nikander52. The transcribed versions were then compared with the recorded discussions to ensure participants’ original meanings and ideas were retained and to guarantee the validity of the data53. The data were coded using qualitative analysis software NVivo v12 (http://www.qsrinternational.com/nvivo). No pre-existing codes or coding structure created in advance were used; an inductive approach was adopted to create the codes, and this allowed codes to occur to the researchers while reading the transcript and examining reviewed literature. The study was an ethnographic inquiry. The rationale for adopting ethnography was to assess roles, behaviours, experiences, and social interactions within a small group in rural communities54,55 in response to a health risk. Given the fundamental assumption of role theory, which stipulates that people consciously perform roles that are expected of them due to their statuses, adopting ethnography in this research will aid exploration of the perspectives of the traditional rulers regarding their roles in fighting the spread of COVID-19.
Thematic analysis was used to analyse the data; it involved finding out, interpreting, and reporting patterns of meaning with data44. Results were written up and themes without enough evidence to support them were discarded. In the reporting of the findings, some proverbs used by the traditional rulers were quoted in their original form and then interpreted in brackets to prevent meanings from being lost in translation because traditional rulers and elders in Igbo culture are known to typically use proverbs when addressing people.
Ethics approval
Ethics approval was obtained from the Department of Psychology Research Ethics Committee (IRB0000-030) of the University of Nigeria, Nsukka.
Results
Measures adopted to protect community members
Evidence from the analysis showed that the traditional rulers had a basic understanding of the COVID-19 pandemic and the preventive measures recommended by health experts. The community members expect that part of a traditional ruler’s role is their protection, and the leaders of rural communities gave examples of fulfilling this role in relation to COVID-19. They stated that they provide running water and detergent in their palaces for the hand hygiene of community members who come to visit them. This helps protect them and serves as a symbol that they (the traditional rulers) believe in the existence of the disease so that their community can emulate them and also make efforts to protect themselves. In recognition of his position as a role model, a traditional ruler stated:
In my palace, I have a wash hand bucket with soap and hand sanitiser. Before you come to my chamber, when you enter the compound, you, first of all, wash your hand with soap and then use sanitiser. You must put on your face mask. So, that is how we do it in my palace; you don’t come there without your nose mask or face mask. (P4)
In Nigeria, funerals and traditional marriages typically take place in rural communities and these events attract many people from both rural communities and cities. At the onset of the pandemic in Nigeria, traditional rulers stopped all ceremonial events that attract large numbers of people. However, they reported that they lifted the ban on ceremonial events but encouraged their subjects to protect themselves during those events by using facemasks, washing hands, and maintaining social distancing because these ceremonies can easily become super-spreader events. Because people in these rural communities exchange pleasantries through handshakes and hugs, the traditional rulers also advised their subjects to reduce human contact in the process of exchanging pleasantries, telling people to greet from a distance without physical contact.
At first, we stopped all funerals, weddings, and other ceremonial events in the village, but now I advise them that they should cover their nose and mouth with facemasks, and if you come to such event, don’t stay too close to other people. Handshaking and hugging, all these forms of greetings that our people use, I told them to try and stop it. If you see your relatives just greet them with your mouth, you don’t have to start shaking hands or hugging each other because of this disease. This much we can do we should try to do it in order to protect ourselves. (P7)
Finally, the traditional rulers also played a role in creating awareness among their subjects about the disease. They used their local information network to spread the information to community members. They also raised awareness among community members in the market squares, and in the churches through their priests. This is because those places (churches and market squares) attract a lot of people and so many people will get the information. The use of priests in churches will also have an impact because Nigerians are very religious; religious leaders have authority, and their followers respect and adhere to their instructions.
We create the awareness in the market square, we create awareness in the churches, our town criers move around early in the morning spreading the information. They hit the Ogene [gong] and tell them: ‘the Igwe [traditional ruler] said that anyone who is to have a funeral or wedding or anything that brings people together, before going there you should make sure you cover your face with facemasks’. Luckily for us, the local government chairman distributed facemasks to us and we shared it to our people. Everyone should wear it and if you are coming you should wash your hand and when you get there, also wash your hand. That’s what we do, we use the town criers to spread the information. (P1)
Risks of an outbreak in the communities
Some traditional rulers stated that there is no risk of an outbreak in their rural communities because they ensure people protect themselves. Others, however, noted regretfully that many of their subjects have abandoned the preventive measures, irrespective of the few suspected cases, to exhibit behaviours that place the community at risk of an outbreak.
It is only God that can say for sure because Igbo people have a saying ‘onye chukwu na azọ na azọ onwe ya’ [whoever God protects should also protect themselves]. There is a risk but by the grace of God, it is only by the grace of God that we have not had an outbreak, we just had few cases, like a man who just came back from America and died. But as for our risky behaviour, which puts us at risk of an outbreak, I believe we are exhibiting behaviours that might lead to an outbreak. Behaviours that are prohibited in the Western countries where the cases are so high irrespective of how careful they are and their more advanced health systems. (P1)
Another traditional ruler added that initially people were quarantined when they returned to the rural communities from the cities, but the practice has been abandoned.
You know that when this thing started, we told everyone that came back from the city to stay in quarantine. To ensure you don’t have it before you start moving about. But with the rate people are just coming back and moving around, it is putting the community at risk of an outbreak. We are just begging God so that people returning to the villages will not be carriers of the disease so that they will not transmit it to others because it will be very terrible. (P8)
Many of the traditional rulers who acknowledged that their rural communities are at risk of an outbreak nevertheless believed that God would protect them. As stated earlier, Nigerians are religious and dependent on God, especially when they feel they are powerless in situations. The traditional rulers cannot force their subjects to adhere to set measures; therefore, they turn to God for protection.
Difficulties in protecting community people
Disbelief about the existence of COVID-19: Analysis of the data showed that many rural people do not believe in the existence of the disease and this makes it difficult for the traditional rulers to ensure their safety. The traditional rulers argued that the Igbo ethnic group are very stubborn and would only believe in the existence of the disease when they witness increased mortality as a result of infections:
As we say, Igbo fụ na-anya fa ekwe na ụka [Igbos don’t believe until they see], anyi anaghi agba ọsọ na abughi mgbe ọmazuru anyi arụ [we don’t run from the rain until it drenches us]. (P2)
Two traditional rulers narrated:
You know that our people are very stubborn. They will ask you why shouldn’t they shake people or hug their relatives. The greatest challenge is that many people do not believe that there is anything like COVID-19. Many do not agree and when you try to explain to them they will say ‘please leave me’. Mgbochi ọria ka ọgwụgwọ [protection is better than cure]. People should do what they are told to do, whether it is real or not, just do it. When you do it, you can stay alive and healthy. If someone should contract the disease and transmit it to others, by then it will be too late because we don’t even have the medical resources for treatment. The greatest challenge we have is that many do not believe in the existence of the disease. But we keep telling them that it is real, do not put yourself at the risk of contracting the disease, if you feel it is not real, go to the hospitals in the city or the isolation centres in the city and see for yourself. (P4)
Mana ịchị anụmanụ ka nfe karia ichi mmadụ [controlling animals is quite easier than ruling over humans], irrespective of all the efforts, people obeyed the rules for sometimes and when they saw that nothing happened, they stopped following the rules. If you go to funerals now, you will be surprised, there is nothing more we can do other than to keep talking to them, you cannot arrest them for it or ostracise them, or remove them from the community. There are no laws to support harsh measures. (P5)
Another stated that members of his community have a contrary view about the pandemic. Many of them believe the disease has been in existence in their community for a long time and is not new. The rural people in his community argued that COVID-19 has been in their community in the forms of common cold and flu, which they have survived for years; therefore, there is no reason to be afraid of it. Some others in his community, however, believe in the novelty of the disease and make efforts to protect themselves.
Members of my community are doing the best they can. But the problem is that many of them do not believe in the existence of the disease. They will be asking who and who is deceased as a result of the disease? Claiming that such diseases have been in existence before they were born, that catarrh and cold have been in existence before they were born. But some of them still believe in the existence of the disease; in churches, they wear masks to protect themselves. (P7)
Widespread poverty: Another challenge identified in the study that prevents rural people from protecting themselves against COVID-19, and traditional rulers from playing their roles effectively, is widespread poverty. Many rural dwellers are poor and thus cannot afford to stay at home to protect themselves – they need a livelihood. One traditional ruler argued that you cannot tell rural dwellers to stay at home to avoid dying when they can die of starvation at home.
You know many people attend burials and funerals so that they can eat because of poverty. If they had what to eat at home, they will remember that they were told not to go to gatherings. But because of poverty and hunger, they will not listen, they will say it is their opportunity to eat, do you want them to starve to death? They will say that death is death. It is hunger that attracts people to ceremonies. They will say that it is better to die of disease than die of hunger. (P4)
Some others stated that because of poverty, the members of their community cannot afford to purchase protective tools such as facemasks and hand sanitiser. Furthermore, the community cannot afford to provide running water in the market squares for the hand hygiene of rural people. Also, the market structure in Igbo land, which is designed to operate once every 4 days, is also a challenge because everyone in the community comes to the market on market days. This can be a COVID-19 super-spreader in the event of an outbreak.
In my community and Igbo land, you know that we are not like Westerners. The Westerners normally have hand hygiene apparatus everywhere. Our problem is that many do not even have these things. The hand sanitisers are not free and many of them cannot afford it. You cannot carry water around to wash your hands, but you can have a bottle of hand sanitiser to use all the time. I believe the local government or state government should find a way to make this available. Again, we don’t have supermarkets, we have village market squares, which all the community members use on Eke [market days] which is once every four days, and everyone will be trying to ensure they buy all they need on those days and when you check, there is no running water in the market, many of them cannot afford to buy good facemasks because many of those made with clothes can suffocate someone. This is another challenge. (P6)
Dealing with the impact of the pandemic on livelihood
The COVID-19 pandemic does not only affect the health of communities; it also affects socioeconomic conditions. Rural people are particularly vulnerable to the economic impacts of the pandemic because lockdowns and movement restrictions affect their economic activities, which mostly depend on remittances from migrants. The economic hardship caused by the pandemic reduced remittances, which have consequentially affected the economy of rural communities. One traditional ruler responded:
Oh of course the economy shut down. When we had lockdown, nothing was moving. It affected economic activities in the community so much that nothing was moving as it should. Everything came nearly to a halt, so it affected us so much. (P1)
The lockdown also prevented people from engaging in economic activities and earning income. Artisans were no longer employed for menial jobs and farmers stayed at home because of the lockdown. Only petty traders who sell essential materials such as medicine and foodstuffs were allowed to open their shops.
ị mana ọdịrị aka mma ọdịrị mgbuji ájá [when it gets good for one person, it becomes good for others]. Migrants who send money to the village for building of their homes, which provide jobs to bricklayers and carpenters no longer send money thereby putting people out of work. Farming activities were also affected, leading to massive unemployment and feeding problems for many. (P6)
However, to cushion the economic impact of the pandemic on their subjects, many of the traditional rulers distributed relief materials in the form of foodstuffs. The traditional rulers received the relief materials from the government, political office holders, and churches. They stated that they distributed the relief materials, starting with the poorest members of the rural communities. The use of traditional rulers for the distribution of relief materials may be said to be effective because they know the rural dwellers and they know those who need support the most. Some of the traditional rulers also stated that they support their subjects with personal resources because many of the rural dwellers are suffering.
Those I can give I try my best to give to them. You must have heard about when we shared ‘palliatives’ [relief materials] to the poorest in my community. I shared foodstuff, like bags of rice, tomatoes, onions, oil, salt, and other condiments to the poorest to support them so that they will not die of starvation because it is they who are alive that can plan for tomorrow. So, we support them at the best. Every now and then my wards come to me and tell me they don’t have money to feed and I give them as much as I have because all of us are now our brothers’ keepers. (P4)
Another added:
We were given ‘palliatives’ at the local government to share to our people. We brought it home and shared it to our people, especially the poor and those in serious need of support. They ensured we started from the poorest in distributing the ‘palliatives’. When you come to the village you will see where people are suffering. So, we started with them so that they will at least have food to eat. Especially when the government made the movement restrictions. Our senator brought, our house of rep member brought and the local government brought. So, we shared palliative three times to them. People were so happy that they saw what to eat. (P6)
Discussion
The COVID-19 pandemic is having a profound impact on the health and socioeconomic wellbeing of people all over the world. Its impact has been felt in Africa and Nigeria, although not as initially predicted by experts14. Similarly, the Nigerian government has also responded through collaboration with WHO, non-government organisations, and other healthcare institutions to produce a framework for reducing the spread of the disease13. However, the federal and state government’s efforts have largely focused on urban centres, which leaves rural communities in the hands of local governments and, more importantly, traditional rulers.
Drawing from the conceptual framework of traditional governance and polity dualism, traditional rulers were shown to provide a link for the government to access rural people45; the authority and influence they command also make them particularly relevant in the fight against COVID-19 in rural communities. Thus, consistent with the tenets of role theory, traditional rulers have been involved in the fight against the spread of COVID-19 and its economic repercussions in rural communities in Nigeria. Findings show that, by following the directives of the government and health experts19, traditional rulers ensured that there were no public gatherings at the onset of the pandemic, and created awareness through town criers, religious leaders, and other community leaders.
Although traditional rulers credit their protection against the disease to the Christian God, they still educate and raise awareness among their community members on the right preventive measures while also fighting the infodemic47, which has led to blatant neglect of set preventive measures20. Findings showed that many rural people believe they are immune to the disease because they have had other strands of coronaviruses that caused illnesses like the common cold, while some argue that they have not seen people dying of COVID-19 in their villages. Traditional rulers play a role in admonishing them, encouraging them to protect themselves, with one ruler stating that ‘prevention is better than cure’.
Another challenge identified by the traditional rulers in the fight against COVID-19 in rural Nigeria is widespread poverty. They argued that the initial stay-at-home order was difficult to enforce because rural people are poor and would starve if forced to stay at home. They also stated that many rural people attend ceremonial events such as weddings and funerals where they can get free meals because it is customary to serve event attendees food at such ceremonies. These ceremonies could easily become super-spreader events.
In response to this and the general economic hardship caused by the pandemic, the traditional rulers distributed relief materials provided by both the government and private citizens28,29 to community members. Federal representatives in the Senate and House of Representatives, as well as the state and local governments, provided relief materials for traditional rulers to distribute. This is consistent with the conceptual framework adopted for this study. The traditional rulers indicated that they started by distributing to the poorest in the communities before giving to other members of the community. In some cases, they had to give their personal money to poor community members to help them deal with the economic fallout of the pandemic. However, these traditional rulers maintained that these efforts are not sufficient because many people in rural communities are still suffering from the economic impact of the pandemic and are therefore in need of more government intervention.
Conclusion
With many countries experiencing another wave of COVID-19, the Nigerian government considering another lockdown, and the identified vaccine hesitancy, it is crucial that the Nigerian government increases their collaboration with traditional rulers who are in direct contact with rural people. Traditional rulers have some level of control and influence on some of the law enforcement outfits in the state; they should therefore make better use of them in further enforcing the preventive measures in their communities in a humane manner. While it may be difficult, but not impossible, to mandate the use of masks everywhere in the communities, the government, with the help of traditional rulers, can provide handwash basins and running water, soap, and sanitisers at market entries. Some rural people cannot afford to buy personal anti-infection kits, and local governments may not be able to supply enough to be shared to the rural people; however, it is not very difficult to supply to market squares and churches, and to permit entrance only after a person has properly sterilised their hands. Traditional rulers play a role in educating rural people about vaccinations and setting an example by publicly getting vaccinated – this will go long way in encouraging increased acceptance of the vaccine by rural people.
Traditional rulers should maintain continuous communication with governments to get timely and accurate information as new data about the pandemic are uncovered and risks of new COVID-19 variants increase. They should also continue admonishing their community members to adhere to the safety guidelines promoted by the government, health experts, and the WHO. Furthermore, engagement with youth will help to disseminate accurate information. Young people are the highest users of technology and social media, and social media sites have been incubators for both factual data and conspiracy theories that can be harmful to community members. Hence, as well as using town criers to share information, traditional rulers can actively partner with the youth in their rural communities to develop messages that resonate with their peers who use social media to communicate protective information to a wider audience. Not only will this provide younger community members with accurate data on the pandemic, but older rural dwellers who do not use social media will become well informed because they will discuss the pandemic with their children or younger relatives.
Traditional rulers should also collaborate with religious leaders to spread accurate information about the disease and vaccines and to ensure that religious gatherings, rituals, and practices are carried out with minimal risk of transmission. They should also encourage people to support their neighbours during this unprecedented time, especially the most vulnerable in the community. They should encourage people to ensure that their older neighbours, children, and the immune-compromised have access to proper nutrition, health care, and assistance with daily living such as grocery shopping, while maintaining social distancing.
The role of primary health workers cannot be underestimated. Thus, the collaboration of traditional rulers, health workers, and social workers will help improve awareness and change attitudes towards the pandemic and vaccines, given that community members may be predisposed to accept the opinion of professionals and health experts, recognising them as people with more knowledge of the pandemic.
Finally, traditional rulers should work to promote empathy in the community because the pandemic can result in discriminatory attacks on vulnerable groups and communities. They should ensure the spread of thoughtful messages that prevent social stigmatising of people in the community.
Limitations
Some limitations were recorded in the study. First, the sample size (n=8) is not a good representation of the population. This was a result of the difficulty in getting this population to participate in research coupled with the pandemic, which has necessitated limited contact with people, especially in the age range of the study population. Therefore, findings should be interpreted with caution as the aim is to provide a detailed description of the research issue and not to generalise.
It is recognised that bias can be a challenge in qualitative research; consequently, the parallel transcription framework by Nikander52 was used to compare recordings with translations to ensure the validity of data53 and avoid bias. To address the credibility, transferability, conformability, and dependability of the research findings, a standardised methodology was used, and the study was conducted in a familiar context with no predetermined research findings, and no participant incentivisation. Finally, the study’s failure to explore the collaboration of traditional rulers and community health workers is another limitation. Therefore, this will be an area of interest for future studies.