Introduction
Opioids are recognized for their analgesic effects and have an important medical application for mitigating acute and chronic pain. Repetitive use, however, can lead to dependence that has consequences for substance use disorder and drug overdose deaths1. The potential for chronic misuse and dependency and the increasing supply in response to demand over the past decades have driven an increase in prevalence of substance use disorder and overdose mortality rates globally2,3. In 2018, overdoses involving opioids accounted for 69.5% of drug overdose deaths in the USA, with two-thirds (67%) of these resulting from synthetic opioids4.
The US Department of Health and Human Services declared the opioid crisis a public health emergency on 26 October 2017, identifying prescription opioid misuse as a leading public health concern and classifying opioid use disorders as an epidemic5. The complexity of the issue poses challenges not only for the legal and healthcare systems, but also for communities seeking solutions to the opioid crisis. Rural communities are particularly impacted by opioid misuse. They have higher opioid prescription and overdose mortality rates and have struggled to tackle these issues due to limited resources6. Although opioid prescriptions are declining nationwide in response to new guidelines and prescription monitoring programs, there is considerable county variability in per-capita opioid prescriptions, with higher rates in rural and micropolitan counties and counties with greater non-Hispanic white populations, higher prevalence of diabetes and arthritis, and higher unemployment rates7,8.
Rural communities face many barriers to addressing opioid misuse and its associated harms. Limited access to evidence-based treatments, behavioral health services and providers, and specialty hospital care presents significant challenges9-11. Attitudes toward addiction treatment, stigma, long travel distances to treatment, and cost are additional barriers common to rural communities9,12. Despite the common challenges that exist among rural communities and a growing number of evidence-based strategies available to address them, individual communities confront unique sets of challenges related to the prevalence of opioid misuse, local conditions, resources, and priorities for intervention13. Therefore, solutions must be developed within the local context and with engagement of key community partners through processes that give voice to those most impacted14. The Stakeholder Engagement in Research Question Development (SEED) Method, a participatory engagement method, was used within a rural community impacted by the opioid epidemic in Southern Virginia as a model for local solutions to the crisis15.
In Virginia, rural communities face significant impacts from the opioid crisis. The rural community in Southern Virginia that is the focus of this article had one of the highest per-capita opioid prescription rates in the USA from 2006 to 201216,17. The community’s opioid prescription rate in 2017 was 336.4 per 100 residents, compared to 58.7 nationally18. The opioid mortality rate was three times higher than the state average (38.8 and 12.4, respectively), and the area had the highest rate of unintentional opioid overdose emergency room visits statewide (55.5 per 10 000 compared to 23 per 10 000 statewide)19. Like many other rural communities, the county has lower levels of educational attainment, higher levels of disability, and lower median household income compared to national data20. Once a prosperous farming and manufacturing center, the community had experienced economic turbulence as production was outsourced overseas and factories closed between 1980 and 200021.
Considering the significant challenges facing this resilient community, community organizations mobilized to form an opioid taskforce in 2016. The local taskforce, led by the police department, included key community partners such as behavioral health providers, the local health coalition, peer- and faith-based recovery programs, the local hospital, and representatives from the judicial system, among others. To establish an action plan, the taskforce connected with an existing community–academic research team, EM Team, that had previously worked in the community to develop and prioritize research questions related to the community's disparity in lung cancer mortality22. In response to the need for methods that effectively involved community members in actions to address opioid and substance misuse in rural communities, and the importance of understanding local conditions prior to choosing strategies for action14, EM used the SEED Method to engage community members for action to address needs related to opioid misuse. The SEED Method is a multi-stakeholder method that uses a community-based participatory research approach to engage diverse community members to address identified health concerns. It engages community residents and partners at various levels of involvement to develop strategies and implement priority strategies through community action planning23. With the help of the local taskforce, EM launched the project using the SEED Method to generate community action plans15.
As part of the SEED Method process, EM conducted in-depth focus groups with key stakeholders in the community affected by the opioid crisis. The focus group information was used to inform the project by providing insight into community members’ views, perceptions, and experiences with the opioid issue. This information assisted the research team and participating stakeholders in the development of strategies and action plans to implement in the community. A complete description of this project15 and the SEED Method is available elsewhere23,24. The focus group process and key findings are reported in this article. The results are particular to this community but may be relevant to other rural communities trying to address the opioid crisis.
Methods
The study was designed to engage community stakeholders from diverse backgrounds in a systematic process of evaluating the factors impacting the opioid crisis, prioritizing strategies to address the crisis, and developing action plans to implement the selected strategies. Participants engaged at three levels: EM Team led the project and identified diverse local stakeholder groups for engagement; three topic groups (TGs) of stakeholder participants explored factors impacting opioid misuse and developed and prioritized strategies to address the crisis; and consulting (SCAN) stakeholders provided local perspectives during focus groups. The EM Team included two university faculty members, a graduate research assistant, two community EM project members who had participated in a previous lung cancer project in the community (one of whom operated as the project coordinator and EM liaison), and four additional community members with personal experience or knowledge in the treatment or prevention of opioid use disorder. The EM Team had diverse demographics: there were three aged 24–44 years and three aged 45–64 years; two Black/African Americans and four White/ Anglo-Americans; and three individuals with a high school education or equivalent, one with a college degree, and two with a graduate degree. TG members consisted of stakeholders who participated in the major project activities, such as reviewing data, identifying potential stakeholder focus groups, developing conceptual models, and prioritizing potential strategies15. Focus groups were chosen as a method of gathering information from consulting stakeholders in order to learn about diverse experiences and gain more information about the community. The TG members used results from the focus groups to create and prioritize actions. The article discusses the themes that emerged from the focus groups.
Focus group selection
Members from each of the three TGs identified community stakeholders with distinct perspectives on the opioid crisis in their community. A facilitated process guided the TGs to identify stakeholders based on lived experience, as well as stakeholders with experiences as a clinical service provider, policymaker, law enforcement official, or a person serving individuals with substance use disorder. Each TG selected one stakeholder group with whom to conduct a focus group. The EM Team went through a similar process to select stakeholders for a fourth focus group. Care was taken to avoid duplication of stakeholder groups, such that four distinct groups with differing perspectives on the opioid crisis were selected.
Focus group recruitment
The EM Team developed a recruitment plan for each of the focus groups. The EM Team identified locations within the community to recruit a convenience sample of participants for each group, such as organizations that have contact with members of the selected stakeholder groups. The EM Team also selected methods for recruitment appropriate to each group, including e-mail listserv announcements, social media posts, newspaper ads, and fliers. Recruitment materials and messages were drafted by the EM Team. Eligibility for all of the focus groups was limited to individuals aged 18 years and older who were current residents or employees of the rural community. Participants were excluded if they did not meet the minimum age requirement or would be unable to participate in oral discussions due to a health condition. The EM Team communicated with interested participants to confirm self-identification with one of the four stakeholder groups selected for the focus groups. Signed informed consent was acquired prior to participation. A single focus group was conducted with each of the four stakeholder groups, with a target recruitment of 8–10 participants in each group.
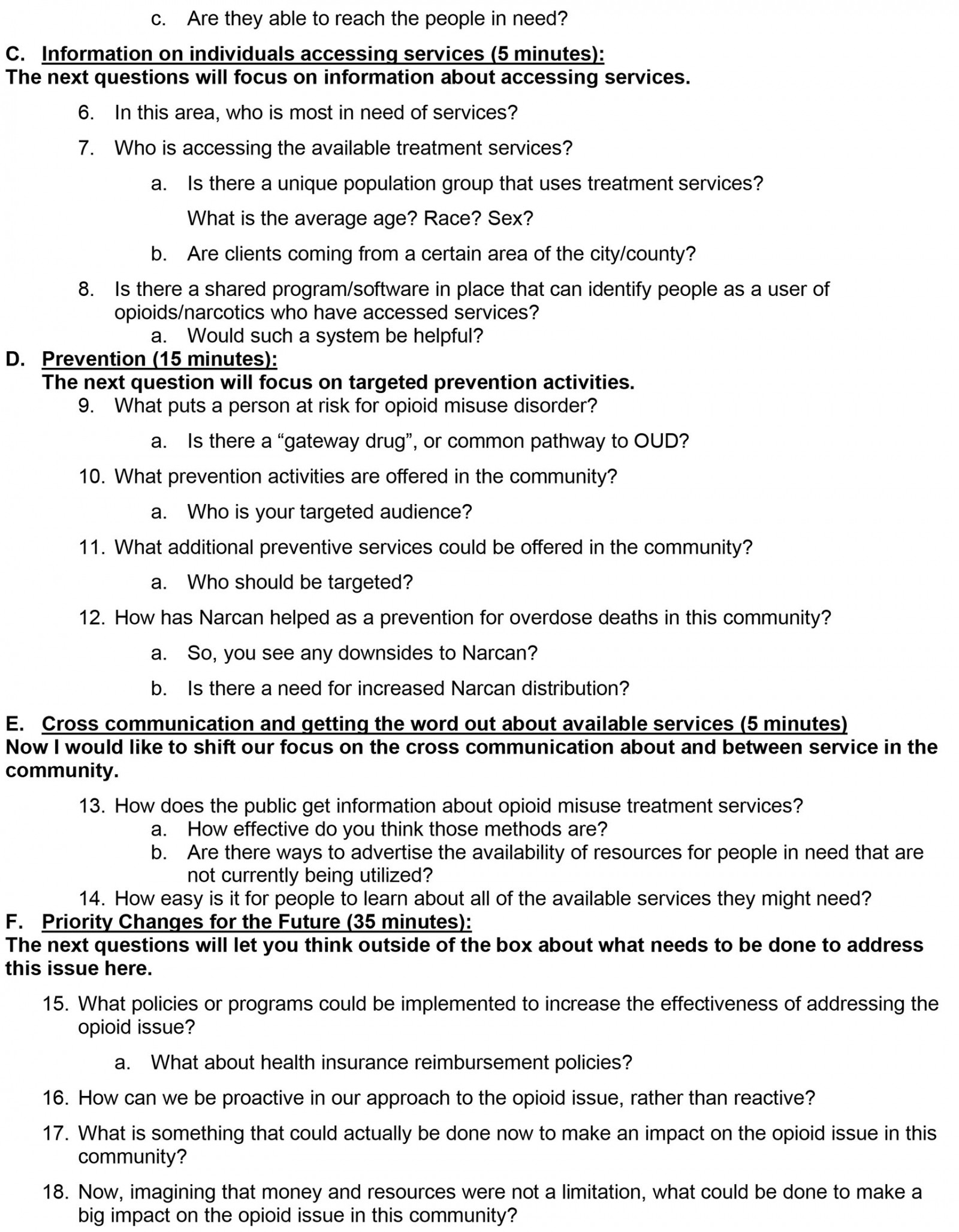
Focus group facilitation
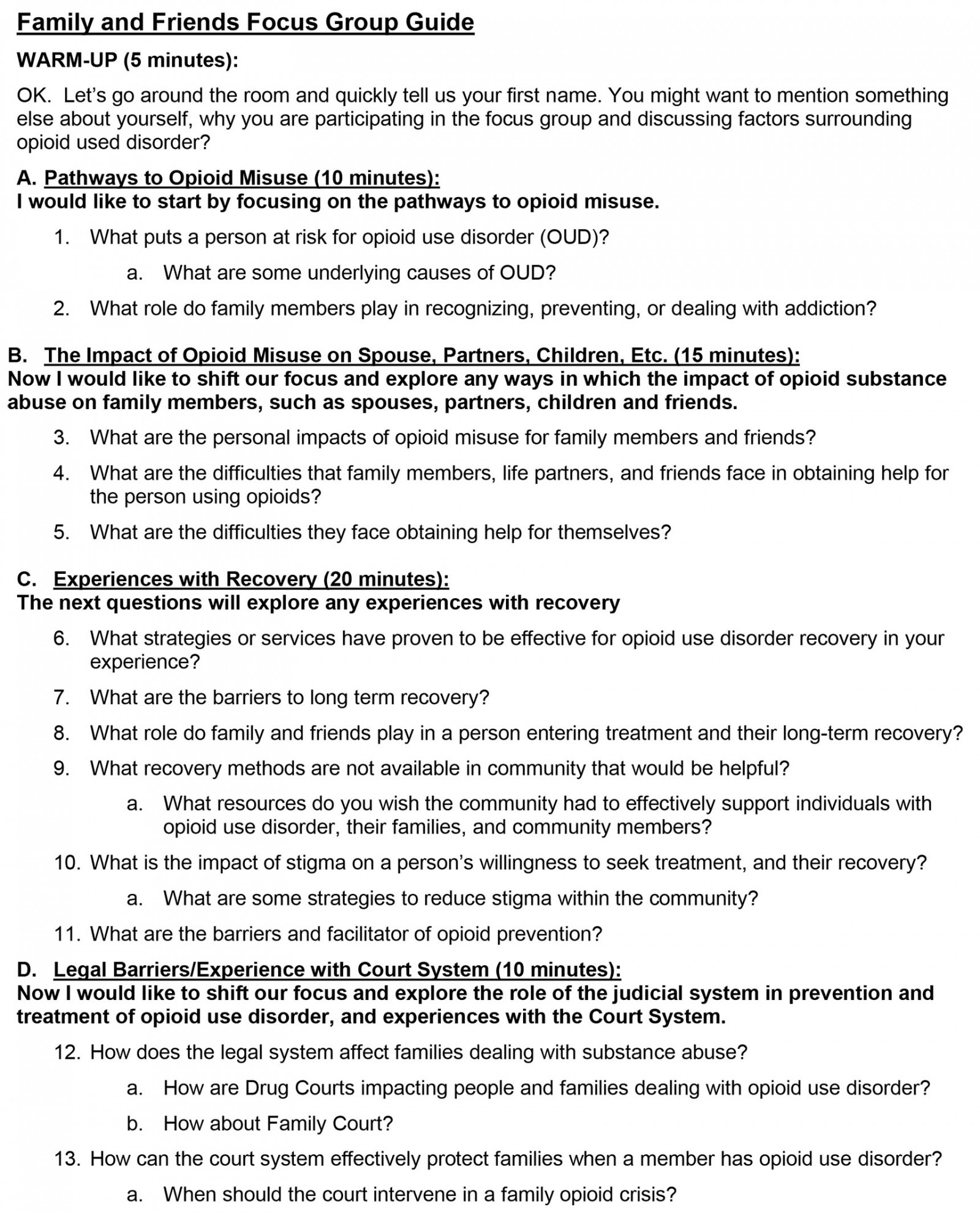
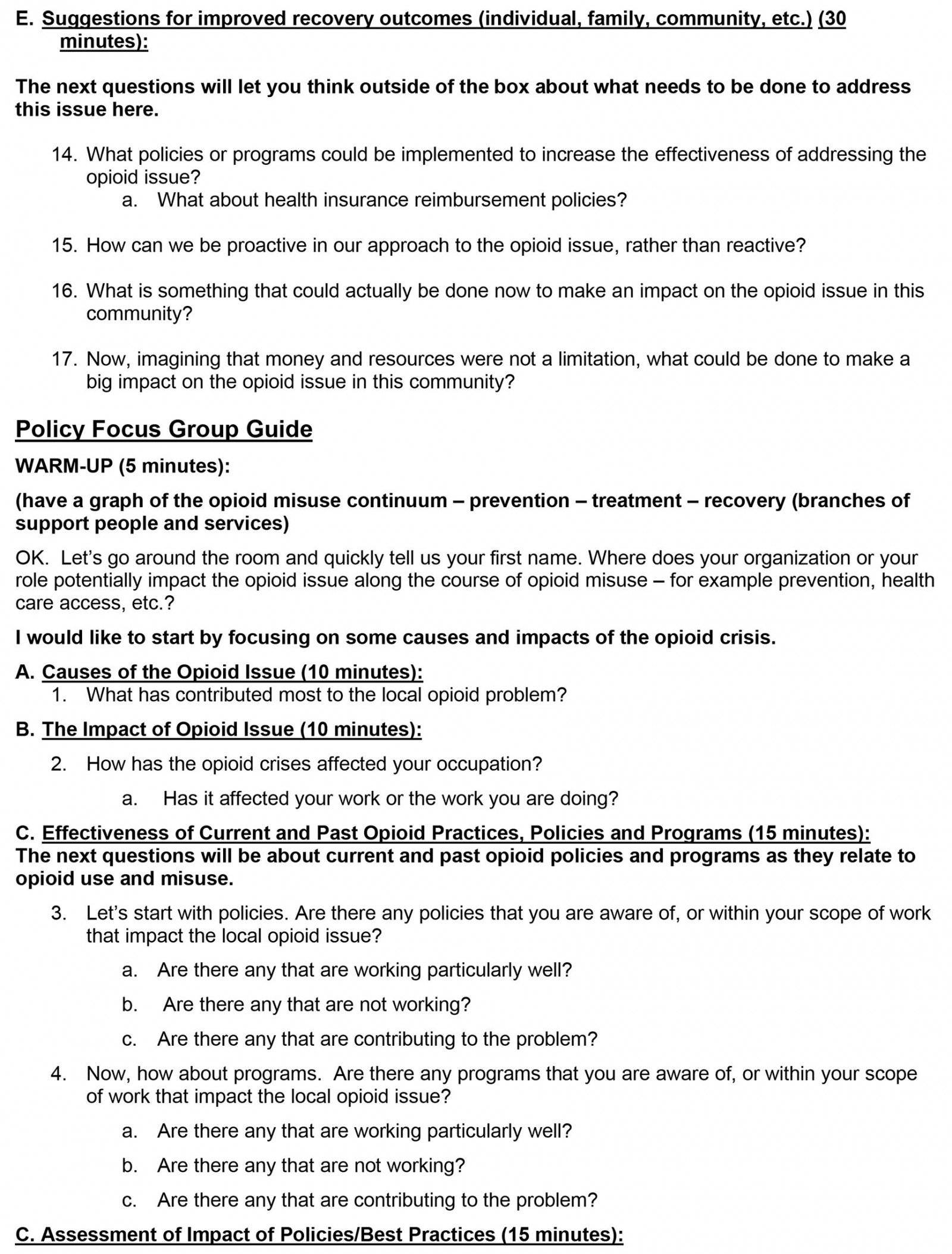
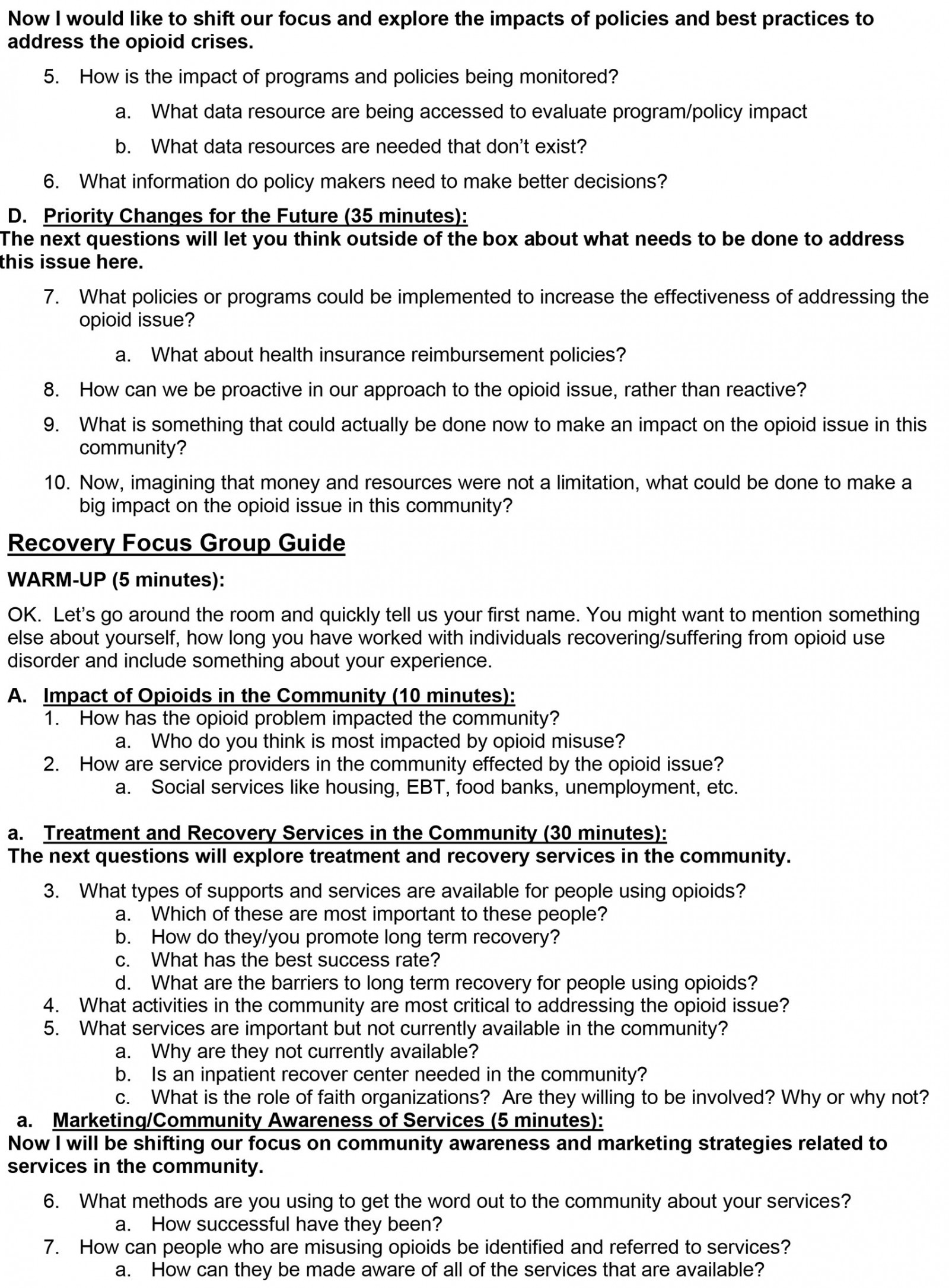
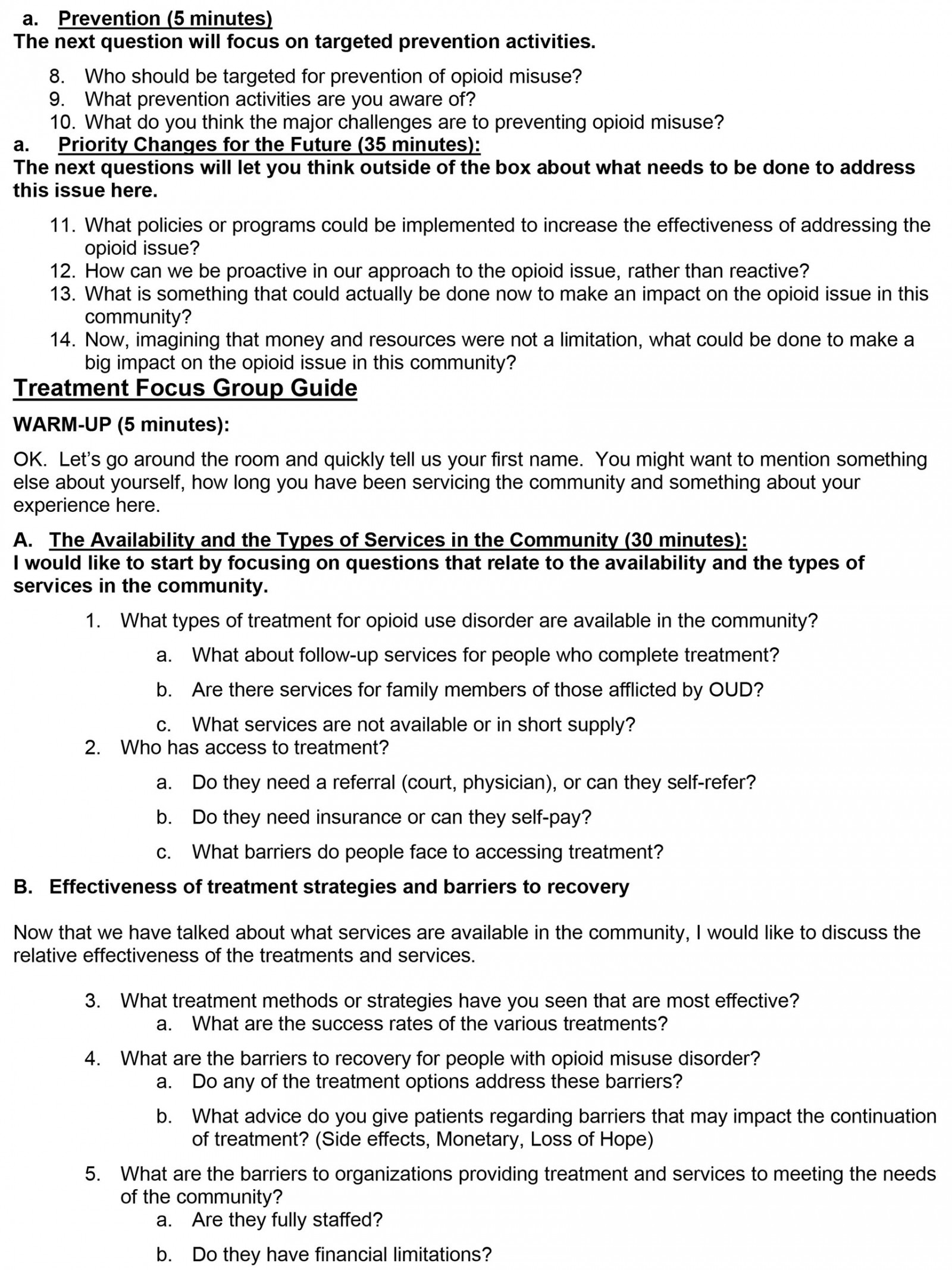
Each 90-minute focus group was facilitated by an EM Team member. Each EM member was trained by an academic faculty member of the research team, and focus group questions were developed by the TGs and the EM Team. A distinct facilitator guide was developed for each of the four stakeholder groups (Appendix I). The questions were generated to explore pathways to opioid misuse, prevention, barriers to treatment, stigma, community awareness, policies, and programs from the perspective of each group.
Data analysis
There were two aims in conducting the focus groups. The first aim was to provide contextual background and a greater understanding of the experiences of diverse stakeholders to help inform the strategy development and action planning work of the TGs. The second was to explore relevant causes of the opioid problem in the community and barriers to prevention, treatment, and recovery. The objective of the focus groups was not to reach saturation; rather, it was to elicit perspectives from four diverse stakeholder groups. For the first aim, the focus group data were initially summarized by research team members and the summarized findings were presented to the TGs for discussion to inform the strategy development and prioritization process. For the second aim, the data were inductively coded using a reliability thematic analysis of the focus group transcripts.
In this analysis, audio-recordings of the focus groups were professionally transcribed. The transcriptions were reviewed for accuracy, and corrections were made when necessary. An initial coding schema was then developed using the focus group summaries created by the research team. Two investigators reviewed the transcripts independently using the schema and added emerging codes. An open coding process was used to break down, compare, and conceptualize the data. The codes for each transcript were reviewed for intercoder agreement, and final codes were agreed upon. Discrepancies were resolved by a third coder. The final codes were then categorized into major themes and subthemes. Themes were derived from the codes and representative supporting quotes were selected through a consensus process and an intercoder reliability matrix. This process was adopted and modified from Braun and Clarke, and Tolley et al25,26.
Ethics approval
The study design was approved by the Virginia Tech Institutional Review Board, protocol number 18-860.
Results
The stakeholder groups identified by the TGs and EM Team to participate in the focus groups included family and friends of opioid users, recovery service providers, treatment service providers, and decision- and policymakers. Distinct areas of inquiry were developed by the TGs and EM Team for each group (Table 1). All four focus groups were asked to discuss actions they felt would improve the opioid situation in their community, without regard to feasibility or cost.
The focus groups were conducted on two separate days in private administrative rooms in a local hospital. There was a total of 26 participants (16 females and 10 males). The participants brought multiple perspectives, with backgrounds ranging from community members, to peer counselors, to policymakers, and represented various organizations and institutions (Table 2).
The results of the four focus groups were organized into five categories: social and environmental factors impacting opioid use and recovery; impacts of opioid use disorder on the family; impacts of opioid use disorder on healthcare providers; barriers and facilitators to treatment and recovery; and communication strategies for targeting at-risk opioid use disorder populations.
Table 1: Composition of stakeholder focus groups and lines of questioning as part of the Stakeholder Engagement in Research Question Development (SEED) Method, in a rural community impacted by the opioid epidemic in Southern Virginia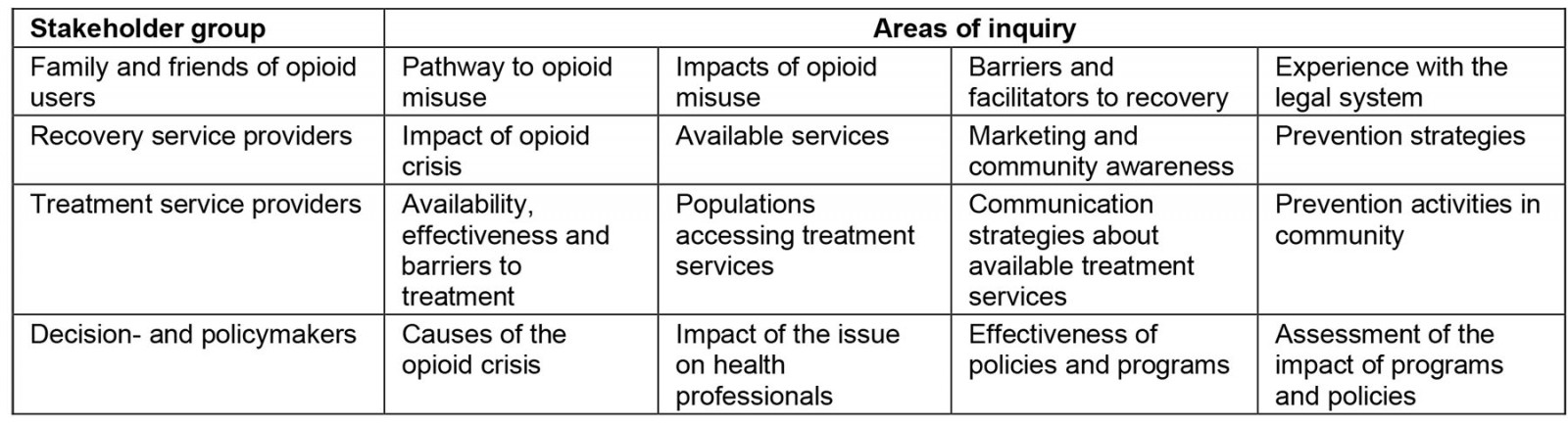
Table 2: Stakeholder focus group participants by affiliation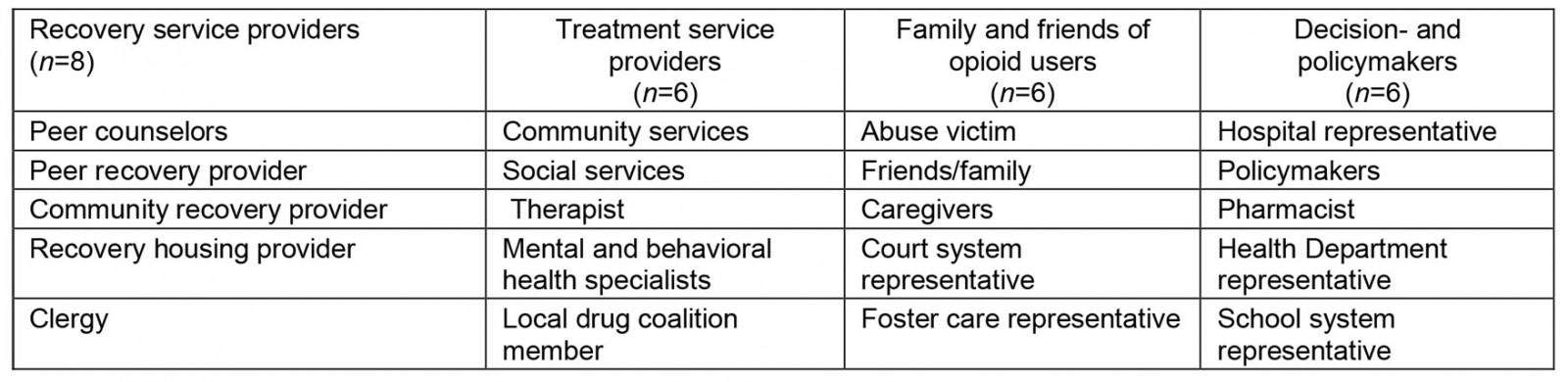
Social and environmental factors impacting opioid use and recovery
The importance of family ties and social networks as risk and resiliency factors in this community was a major theme. Strong family and social ties form an important safety net for individuals, but also increase potential negative influences of family and peers on attitudes and actions related to substance use. Focus group participants highlighted multi-generational substance use as one of the root causes of the opioid crisis. They reported that drug use, particularly prescription drug use, may be normalized in the home by family members modeling substance use behaviors. The presence of drugs in the home, and early childhood exposure to parents who use substances, may increase individuals’ propensity for substance misuse.
… when you ask, ‘where did you get it?’ ‘Mama had it at the house.’ It’s two or three generations that’s all caught up in the addiction.
Focus group participants also discussed industrial jobs and the role of historic economic decline in this once-prosperous manufacturing community as a contributing factor in the opioid crisis. Abundant, well-paid manual labor jobs of the past had allowed residents with limited higher education to prosper, but also increased the need for pain management resulting from physical injury and work-related pain. As prescription opioids became more abundant and were promoted by pharmaceutical companies and prescribed by trusted physicians, their use increased and was normalized as a response to pain. The ongoing closure of manufacturing companies in the community resulted in a lack of jobs suited to the local labor force. Over time, unemployment led to a sense of hopelessness and low self-esteem, further driving the abuse of readily available substances. Lack of mental health services to help residents cope was identified as a compounding factor.
I quit school in the 8th grade and went and worked at [the factory], and now I have no job and I have no education … I'm 52 years old, and I ... I don't even know what to do with myself.
Impacts of opioid use disorder on family
The emotional toll on families of individuals with opioid use disorder was a recurring theme in the focus groups. Participants described the extreme internal conflict they experienced trying to help their loved ones. They felt conflicted about the role of ‘tough love’ for the purpose of assisting someone's long-term wellbeing. They also struggled with the balance between helping their loved ones overcome their addiction and allowing their loved ones to avoid facing repercussions.
… that's all you want to do is help them. But at the same time, you're helping them … it's too fine a line. You're, you're also enabling and hurting them.
Comments like these show the difficulty that family members experienced trying to find appropriate ways to support their loved ones, and they reported that these struggles resulted in strained interpersonal relationships and distancing. This is particularly significant in view of the importance of family ties within the community.
In addition to the emotional toll of supporting a family member with opioid use disorder, the significant financial costs impacting the extended family were described. The financial costs included support to addicted individuals as well as the costs associated with incarceration, an often-unrecognized financial burden that strains the social support network and may delay treatment due to depleted financial resources.
Impacts of opioid use disorder on healthcare providers
Focus group participants described how the increasing demand for services for people with opioid use disorder has overstretched the limited treatment and social service resources available in this underserved rural community. High caseloads have increased the burden on providers and reduced the quality of care. Providers experience guilt over their inability to provide the time and human resources needed to adequately address their patient needs, as well as burnout from the cycle of opioid users’ needs and demands.
From the social services sense, I think it makes your caseloads high. Too high to manage. Um, you don't spend as much time with clients as you probably should. Um, you know, you become like a revolving door of trying to help somebody.
… [Community Service Boards] are just understaffed, overworked and everything else …
Participants described how the dramatic reforms related to opioid prescriptions and pain management policies have had mixed impacts on the community’s healthcare providers. While dramatic decreases in opioid prescriptions were seen as a good thing, participants worried that the result was inadequate pain management for some patients. New regulations and monitoring systems have also increased physician concerns about risks to medical licenses. Providers discussed feeling unprepared to treat opioid addiction in their patients while managing their pain and expressed the need for appropriate training. Providers also described expectations for pain medication held over from the decades of treating pain as the ‘5th vital sign’27. Providers felt caught between meeting regulatory expectations for eliminating pain and prescribing under the new guidelines.
Some primary care providers are just wanting to cut it off and say, ‘Okay, I'm stopping you.’ When essentially you can't just stop [the opioid medications] because you're gonna create a bigger problem. So, it's, ‘How do we stop? How do we win? How do we transition?’
Participants from the provider groups discussed how the changes impacted them. New opioid prescription regulations have resulted in difficulty accessing pain medications among patients with pain management needs. A public health specialist from the policy focus groups reported that monitoring practices have left patients feeling like criminals, and prescription opioid use has been stigmatized.
I've been on a fentanyl patch for years … and it makes me able to get to work every day. And now, suddenly, I'm a criminal. I feel like I'm a criminal. I'm going in to get my fentanyl patch and everybody's looking at me.
Barriers and facilitators to treatment and recovery programs
Focus group participants indicated that availability of treatment and recovery services was increasing in the area; however, lack of certain essential services continued to be an issue. These included the lack of local services for inpatient detoxification and a comprehensive system providing a continuum of care from detoxification through long-term recovery. Participants stated that an integrative approach to substance abuse treatment that meets patients' needs, takes a holistic approach, addresses root causes, and provides transitional services could be more effective in changing and increasing the chances of continued recovery while lowering the chances of relapse. Of the services available in the community, medication-assisted treatment, peer recovery groups, rehabilitation centers, faith-based recovery programs, and long-term recovery programs were identified as particularly effective.
The significance of adopting an intrinsic, patient-centered approach to treatment and recovery that addresses the ‘whole person’ was a recurring theme in assisting individuals during recovery programs.
It's a process of changing the way somebody thinks – the way they deal with the stress, the way they deal with emotional problems. Because all of that has always been pushed away with chemicals.
Holistic and comprehension approaches must also address the social determinants of health that are associated with treating the whole person.
… Maslow’s levels of need are not being addressed. So, we have to assess them for food, security, relationships, housing, everything … things that can come on board and help them find a place to live, or transportation to get to treatment.
Participants also discussed judicial policies as barriers to recovery because they place a financial burden on those charged with substance-related offenses. An example was court fines that, if not paid, result in revocation of drivers’ licenses. Lack of a driver’s license limits the ability to work to pay the court fines, compounding the situation and putting treatment and recovery further out of reach. Lack of treatment while incarcerated; lack of effective linkage to social services, peer counselors, and treatment programs upon release; and cyclical incarceration were also important barriers to long-term recovery.
Finally, ensuring ongoing funding for opioid healthcare services and programs in the community was identified as critical. Medicaid expansion has provided funding for the most vulnerable. However, inconsistent and insufficient health insurance reimbursement policies and the variable allocation of government funds for programs remain significant funding barriers to expanding treatment services. Participants emphasized keeping legislators informed of ongoing funding needs and opioid statistics. To accomplish this, it is important to address limitations in local opioid data, such as the accuracy and availability of opioid overdose information coming from emergency services, and to solve barriers to interagency data sharing and metrics relevant to city and state funding decisions.
… you had to use different silos, we'll just call them state police, department of health, social services, whatever. The don't talk to each other. And they, they still don't talk to each other within the rules of HIPAA [Health Insurance Portability and Accountability Act].
The stakeholders need to be at the table at all times and the legislative branch needs to hear from people all the time …
Communication strategies needed for targeting populations at risk for opioid use
Another focus group theme was stigma associated with opioid misuse and the need to reduce stigma. Participants felt that stigmatizing opioid misuse kept people in denial and prevented them from seeking help. Stigma also hinders people with legitimate pain issues from receiving appropriate care. Depersonalization of individuals with opioid use disorder was felt to permit stigmatization. Campaigns to combat the stigma were recommended.
Promoting a ‘culture of hope’ in the community was a second communication theme. Hopelessness due to the lack of economic opportunity was identified as a driver of opioid and substance misuse in the community. Participants saw schools as a vital community institution that gives hope to children. Therefore, strategies to communicate a broader vision of hope for the future were targeted at children and youth.
In the school system teaching children, the ability to dream about what they know … Realizing there's something out there besides what I know. There's more to life than what I've seen. Forming a program that focuses on hope, exposure, and greater opportunities can shift the minds of the youth.
Priority actions to combat the opioid crisis
As part of the focus group discussions, participants were asked to share ideas for actions that could reduce the opioid problem in their community, without regard to cost. The focus groups yielded several recurring ideas. The most commonly occurring concepts in the data were classified as actions. The top five proposed actions were establishing a drug court to divert people from the legal system and into treatment and recovery, allocating sufficient human and financial resources to meet the service needs of those with opioid use disorder and their families in the community, providing drug avoidance education in the schools and for those who are incarcerated, establishing a long-term rehabilitation program in the area that includes family in the process, and using the school system to promote hope among youth (Table 3)15.
Table 3: Supporting quotes for commonly proposed actions among focus groups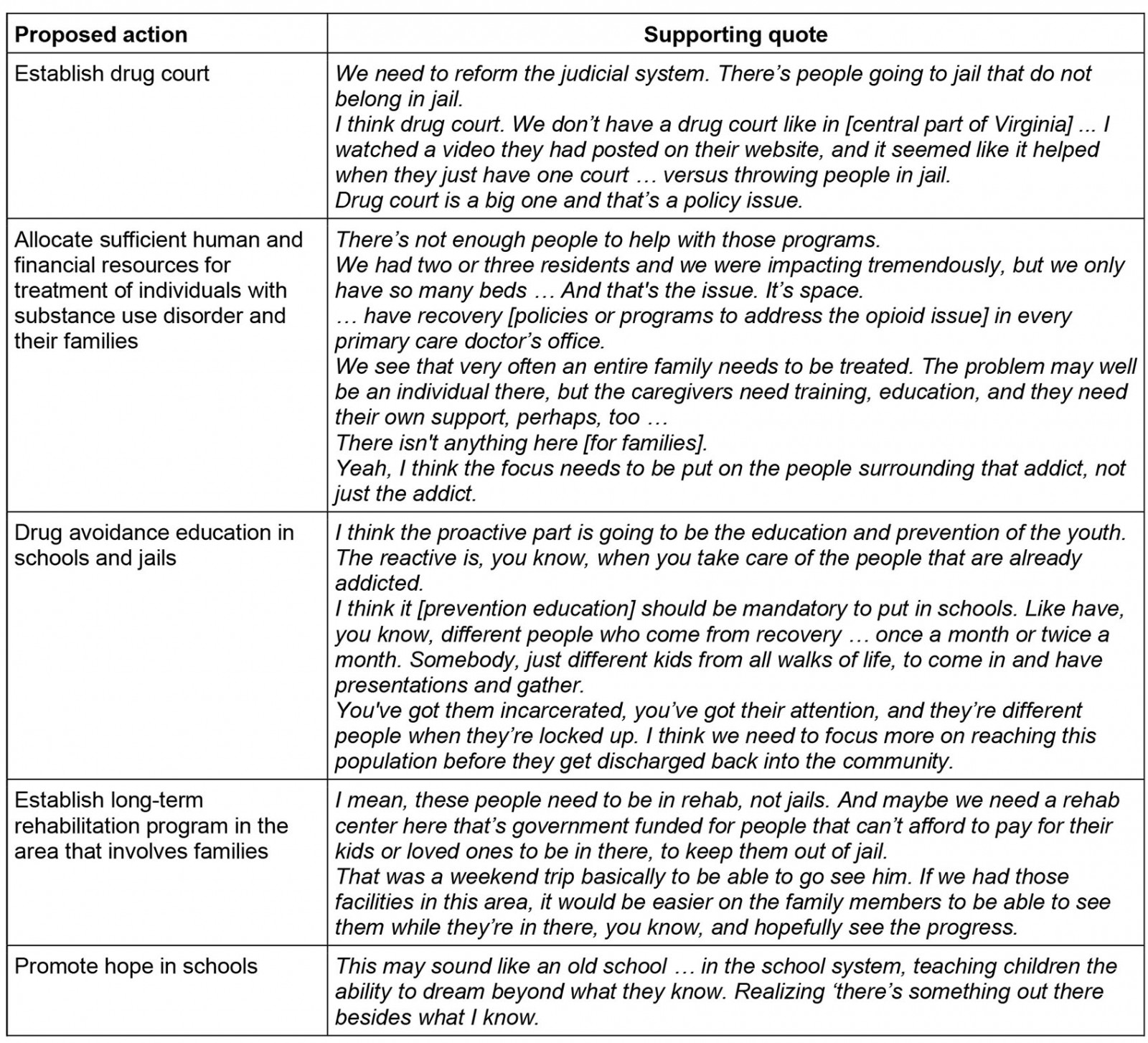
Discussion
The rural community where this study was conducted falls within the area considered Appalachia, and shares many of the characteristics with those communities that made them vulnerable to the opioid crisis: high rates of chronic pain due to the large number of manual labor jobs, inadequate regulatory oversight, overmarketing of opioids, availability of willing prescribers, and lack of public education about the risks or prescription pain medications28. Despite the commonalities of these rural communities, solutions to opioid and substance misuse must be based on local experience. The EM Team held four focus groups with diverse stakeholders impacted by the opioid crisis (individuals in recovery/family and friends of people with opioid use disorder, treatment providers, recovery providers, decision- and policy makers) who provided valuable perspectives on the opioid problem in their community. They highlighted the impact on service providers and patients, explored barriers to treatment and recovery, and proposed potential strategies and solutions.
The importance of family to the social support structure for individuals dealing with opioid misuse in this community was a salient point. An important cultural difference between rural and urban life is the breadth and influence of family networks29. Strong family ties are an important support system for those dealing with opioid misuse and other stressors but can also pose a potential risk for intergenerational opioid misuse and hinder long-term recovery29,30. Addiction is a disease that impacts not just the user, but also the user’s family and social network31. Taking a holistic approach to treatment and recovery that engages and provides support to the family is particularly important in this rural context. Programs to support healthy families and family dynamics in communities that rely on strong kinship networks are crucial when addressing opioid and substance misuse. Programs should focus on building individuals’ ability to manage and plan for difficult social, financial, and relational situations, and should disrupt the intergenerational transmission of substance use by addressing the multiple factors that influence undesirable behavior32-34. Using a family and social network approach to address substance use can result in better treatment outcomes and reduce harm for both the person misusing substances and other family members35,36. As a best practice, substance use disorder providers should assess the strengths and needs of a user’s family and social networks, and implement evidence-based approaches that address those needs37.
Focus group participants described a lack of opportunity, and an associated pervasive hopelessness as important contributors to opioid misuse in the community. Hope is an important factor in addiction and recovery. It has been defined as the will and confidence to see things through, set goals and develop steps to achieve them38,39. Higher measures of hopefulness are associated with decreased likelihood of substance use in adolescents and may moderate the effect of other risk factors, such as depression40-42. Promoting a culture of hope through schools, social activities, economic opportunity, and job creation were key recommendations from focus group participants.
Rural areas have fewer per-capita general health and mental health providers compared to urban areas39,43,44. The disproportionate incidence of opioid misuse in this community has strained already-limited healthcare and social service resources, causing an overburdened workforce dealing with new prescription regulations, pain management needs, treating opioid use disorder patients, and providing long-term recovery services. The frustration of healthcare and social service providers unable to provide quality care due to time, training, and resources constraints was palpable and consistent with other rural community experiences45. Expanding the existing workforce and providing adequate training to healthcare providers were seen as essential strategies to address opioid misuse in the community. The former is challenging, as recruiting qualified healthcare professionals to work in rural communities is difficult under the best of circumstances46. Creative solutions will be needed to accomplish this, such as increasing access to healthcare professionals through telemedicine47, task sharing48, interdisciplinary partnerships49, and targeting rural students for medical training and residency programs who are more likely to stay in the community46,50.
In addition, focus group participants identified important strategies for stopping the cyclical demand for services for individuals with opioid use disorder, including increasing detoxification and long-term recovery services and establishing effective systems to transition patients across the continuum of care. In rural communities with limited resources, collective impact could be improved through better coordination between existing services, including non-traditional and faith-based recovery programs. As one participant expressed:
I don’t think it’s a standalone solution. I don’t think a local community service can fix it alone.
To expand and sustain effective programs for those impacted by opioid dependence, this community recognized the importance of government action. Statistics drive legislation, and there was a need to improve the data currently available to inform local legislators, healthcare providers, and service providers. Information about repeat offenders, emergency medical services visits, treatment visits, and Narcan usage were seen as critical. Breaking down regulatory barriers to data sharing between the organizations in possession of the data was identified as a key first step. Consistent, ongoing communication with legislators that presents clear, concise ideas and statistics, as well as personal testimonies from constituents, would assist legislators in attaining the necessary support to move priority actions forward and maintain prevention and treatment funding in the community.
The findings presented here are useful in understanding the viewpoints of important stakeholders in a rural Virginia community that has been severely affected by the opioid crisis. These findings could be very useful for other rural populations in similar situations but may not be substantially generalizable in other contexts. This study did not seek to reach saturation with any of the stakeholder groups because the information received from these four groups was used to inform a larger approach. As a result, it's possible that not all of the important information from these stakeholder groups was gathered. Having said that, this study purposefully set out to acquire varying community perspectives from as many community voices as possible. The data presented here provides valuable viewpoints from these stakeholder groups.
Conclusion
Rural communities face unique challenges that can hinder the process of mitigating the crisis of opioid use disorder. These communities have the essential tools to combat this public health crisis, especially if they can foster strong community engagement and prioritize actions suited to the community. The study demonstrates the use of community-engaged approaches that gather multi-stakeholder input to identify tailored strategies is a promising approach to addressing the opioid crisis in rural communities.
Community stakeholders identified and advocated for rational solutions to address substance use disorder and opioid use disorder. Those strategies include increasing access to local long-term treatment programs, targeting youth for prevention, addressing stigma and hopelessness, increasing and equipping healthcare personnel, incorporating holistic approaches, and developing a drug court. The information gathered from the focus groups was used to inform the community stakeholders engaged in the SEED Method, who ultimately developed strategies they felt were needed in their community, and that they felt empowered to implement.
The findings reported here are limited in that they come from only one community. Nonetheless, the perspectives shared by these diverse stakeholders will resonate with people in other rural communities or at least form a basis for discussion and reflection.
Acknowledgements
This material is based upon work funded by the Office of Research and Evaluation at the Corporation for National and Community Service (CNCS) under Grant No. 18REHVA001 through the community conversations research cooperative agreement competition. Opinions or points of view expressed in this document are those of the authors and do not necessarily reflect the official position of, or a position that is endorsed by, CNCS.
The academic research team members wish to express our gratitude to the rural community for their assistance and willingness to work beside the research team. The academic research team members are sincerely thankful for all the EM research team members, focus group and topic group participants, and community organizations that supported, invested, and took part in the collaborative experience.