




Introduction
About 12 million girls give birth every year globally, most of them from low- and middle-income groups. An estimated 3.9 million adolescents (defined here as ages 15–19 years) undergo unsafe abortion, which is particularly concerning in low- and middle-income countries1. Complications of pregnancy and childbirth are the main causes of adolescent death. Also, babies born to adolescent mothers have a 50% higher risk of experiencing death2. Adolescent birth in low- and middle-level economies can lead to school leaving, loss of productivity and an increase in intergenerational poverty3.
The Indonesian Government, through the Population and Family Planning Board, sets a target every year for adolescent births. In 2020, the Indonesian Government aimed to reduce the adolescent birth rate from 33 to 25 per 1000 adolescent girls4. The adolescent birth rate in Indonesia (47 per 1000 adolescent girls in 2018) is high compared to the adolescent birth rate globally (42 per 1000 adolescent girls). The adolescent birth rate is lower than the birth rate in Indonesia in 2014 (48 per 1000 adolescent girls)5. This rate is much smaller than for African countries.
The 2017 Indonesia Demographic and Health Survey (IDHS) showed that, in Indonesia, 5% of adolescent girls had given birth and 2% were pregnant with their first child. The percentage of adolescent girls who have given birth or got pregnant with their first child decreased from 10% in the 2012 IDHS to 7% in the 2017 IDHS. The adolescent pregnancy rate was highest among adolescents who had completed primary education or less (15–37%)6. The national adolescent birth rate was 46.9 per 1000 adolescent girls, with a provincial level ranging from 19.7 to 95.1 per 1000 adolescent girls7.
The results of research conducted in Ghana indicated that adolescent birth was significantly influenced by the level of education of girls and their partners, girls’ employment, wealth status and media exposure8. The education level of girls is the most influential and consistent factor related to the likelihood of giving birth in adolescence. In particular, adolescents with a primary level of education are twice as likely to have had a first-time birth compared to adolescents educated at the secondary level, even after analysis controlled for age, period and other characteristics9. Insufficient knowledge about adolescent pregnancy, cultural acceptance, illiteracy, lack of knowledge about the consequences of adolescent pregnancy, difficulties in obtaining information and access to family planning methods are the main factors causing adolescent pregnancy and dropping out of school as a result of adolescent pregnancy10.
Some factors like age, living in a rural area, not using contraception and the marital status of parents (divorced) had a statistically significant relationship with adolescent pregnancy11. United Nations divides adolescent gestational age into 15–17 years and 18–19 years12. Family factors can also be a driving force for adolescent pregnancy: previous research showed that the chances of adolescent pregnancy for girls with at least one older sister who had adolescent pregnancy were 3.38 (99% confidence interval (CI) 2.77–4.13) times higher than for girls with an older sister who had no history of adolescent pregnancy. Girls whose mothers had a first child before age 20 years were 1.57 times (99%CI 1.30–1.89) more likely to have adolescent pregnancy than those whose mothers had a first child after age 19 years13. Another analysis showed that adolescent birth in Congo was strongly influenced by religion, economic level, education level, knowledge of contraceptive methods, marital status, age at first intercourse and age at first marriage14. Education, policy, economy, and social and community have a relationship with adolescent pregnancy15. Likewise, adolescent pregnancy in Namibia was significantly influenced by the use of contraceptives, the age at which girls have sex for the first time, education level and household wealth status16.
Indirect causes of adolescent pregnancy include rights violations, gender inequality, child marriage and socioeconomic inequality3. Previous studies have also explored the relationship between the ownership of health insurance and adolescent births: the results of a study showed that there was a significant relationship between the age of pregnant women and the ownership of health insurance17,18. Many efforts have been made to reduce adolescent pregnancy by empowering adolescents through education, community, economic and policy interventions. Further research should be performed to clarify their role in reducing adolescent pregnancy16. This study aimed to analyse the determinants of adolescent birth in Indonesia.
Methods
Data sources and design
This study used secondary data from the results of the Government Performance and Accountability Survey (GPAS)/Survei Kinerja dan Akuntabilitas Program (SKAP) 2019 which was conducted in July – September 2019 by collaboration between BKKBN (the National Population and Family Planning Board) and Badan Pusat Statistik (BPS; Central Agency on Statistics) with representative sample coverage at the provincial and national levels. The target population of this survey was households, females of childbearing ages 15–49 years, families and unmarried adolescent girls aged 10–24 years. This survey was conducted by using a cluster approach as an enumeration area. The cluster referred to in this survey was a collection of census blocks (one or more census blocks) that were close together, located on one stretch, and with a load of about 200 households. The sampling design for this survey was stratified multistage random sampling.
Sample selection
GPAS 2019 was designed to produce parameters estimated at the provinces and national level. The target number of the 2019 GPAS sample was 67 725 households spread across 34 provinces, 514 districts/cities in 82 030 villages with a total of 1935 clusters. Following the previous long-term national plans and GPAS surveys, respondents consisted of household respondents, family respondents and females of childbearing ages 15–49 years, however, in 2019 the youth module (unmarried) was 10–24 years.
Sampling in this survey was carried out in several stages. The first stage involved selecting several villages by probability proportionate to size (PPS) sampling with the size of the number of households in the list of all villages (or in the sample frame of all villages). The village sample selection was carried out independently between urban and rural areas in a district/city. The second stage involved selecting one cluster from each selected village through PPS sampling with the size of the number of households in the selected cluster. The third stage involved selecting 35 households using systematic random sampling based on the results of household listings conducted by door-to-door interviews by enumerators in the selected cluster using applications on smartphones.
All females aged 15–49 years in the 35 selected households in each selected cluster constituted the sample of females aged 15–49 years. This study took a sample of 7786 adolescent girls from a total of 59 825 females aged 15–49 years), with a response rate of 99.7%.
Variable measurements
This study defined adolescent birth as birth by adolescent girls of childbearing age to at least one child showing signs of life such as crying, breathing or moving (even if the baby lives for only a few minutes), regardless of the length in the womb. This can be described as ‘children ever born’ (CEB). Data processing on adolescent pregnancy variables was carried out so that code 0 denoted non-CEB adolescents and code 1 was for CEB adolescents.
The predictor variables used in this study include social, economic, demographic, media information and reproductive history characteristics. The following predictor variables were analysed:
- highest level of education of adolescents: this variable was categorised into ‘no education’, ‘primary school’, ‘secondary school’, ‘high school’ and ‘tertiary education’
- region: the area where adolescents live, whether in urban or rural areas
- level of welfare: this variable was categorised into ‘low’, ‘medium’ and ‘high’
- employment status: each adolescent girl was asked about her status and type of work which was then categorized into ‘working’ and ‘not working/housewife’.
- insurance ownership: this related to health insurance ownership status for both National Health Insurance (NHI) and non-NHI health insurance. This variable was categorised into ‘having health insurance’ and ‘not having health insurance’
- family planning information: health information and family planning (family planning tools/methods) was categorised as ‘yes’ (receiving family planning information) and ‘no’ (not receiving family planning information)
- access to family planning print media: this referred to family planning information obtained by accessing various types of print media such as newspapers, magazines, pamphlets/leaflets/brochures, flipcharts, posters, banners and billboards. This variable was categorised into ‘yes’ (getting access) and ‘no’ (never getting access)
- access to family planning electronic media: this referred to family planning information obtained by accessing various types of electronic media such as radio, television and the internet. This variable was categorised into ‘yes’ (getting access) and ‘no’ (never getting access)
- age at first sexual intercourse: this variable was categorised into ‘10–14 years’ and ‘15–19 years’
- age at first marriage: this variable was categorised into ages ‘10–14 years’ and ‘15–19 years’.
Data analysis
The data analysis of this study used the Statistical Package for the Social Sciences v23 (IBM; https://www.ibm.com/analytics/spss-statistics-software). The statistical analysis technique was carried out descriptively and inferentially. Descriptive, presented bivariate data tabulation was used to determine the distribution of data between predictor variables and adolescent births. Listwise deletion or univariable and multivariable analysis was used for missing data. Analysis was carried out to determine the factors that influence adolescent birth by using simple and multiple logistic regression tests (confidence level 95%)19. The multicollinearity test was assessed by a correlation matrix among the predictors in this study. The test showed correlation coefficients among independent variables were less than 0.90, which meant that the assumption of multicollinearity was met.
Ethics approval
This study was approved by the Committee of Research Ethics of The Family Planning and Reproductive Health, BKKBN (454/LB.02/H4/2019). This survey was implemented based on the regulations of the Head of BKKBN (11/2018).
Results
The total responses in this study were 7786 respondents, 373 respondents of whom were CEB adolescents (4.8%). Most CEB adolescents had a junior high school level of education (48.3%); tertiary level education was 1.3% (Table 1). Of those respondents who had no education, 26.2% were CEB adolescents; this contrasts with 0.9% of respondents with tertiary education being CEB adolescents. There were 236 rural CEB adolescents (6.4% of all rural respondents), compared to was 137 CEB adolescents (3.3% of urban respondents). A total of 42 CEB adolescents were already working (5.4% of all working respondents) compared to 331 adolescents who were not working (4.7% of all non-working respondents) (Table 2).
The highest percentage of CEB adolescents in terms of welfare was at the low welfare level (n=150, 8.2%), then the medium level (n=175, 4.4%), and the lowest percentage were at the high welfare level (n=48, 2.4%). CEB adolescents tended to have received information about family planning (n=330, 5.2%), either by accessing it through printed media (5.5%) or electronic media (5.1%). Adolescent birth in this study, occurred mostly in adolescents who engaged in first sexual intercourse at the age of 15–19 years, which was 51 adolescents (73%), and were first married (n=30, 68.8%) at the age of 10–14 years (Table 2).
Table 2 shows that the statistical test results are not all significant for births in adolescence. Several variables that did not significantly affect adolescent births were level of education, family planning information, insurance ownership, age at first marriage, access to print media, access to electronic media and age at first marriage.
The results of the multivariate logistic regression test, when measured simultaneously, showed that the birth of adolescents was significantly influenced by the area where an adolescent lived, work status, welfare level and age at first sexual intercourse. The most influential factor in determining births in adolescence is the age at first sexual intercourse (OR=2.286, 95%CI 0.847–6.168). Even so, the age at first marriage for adolescents in this study was found to have no significant effect on adolescent births (Table 2).
Table 1: Respondent characteristics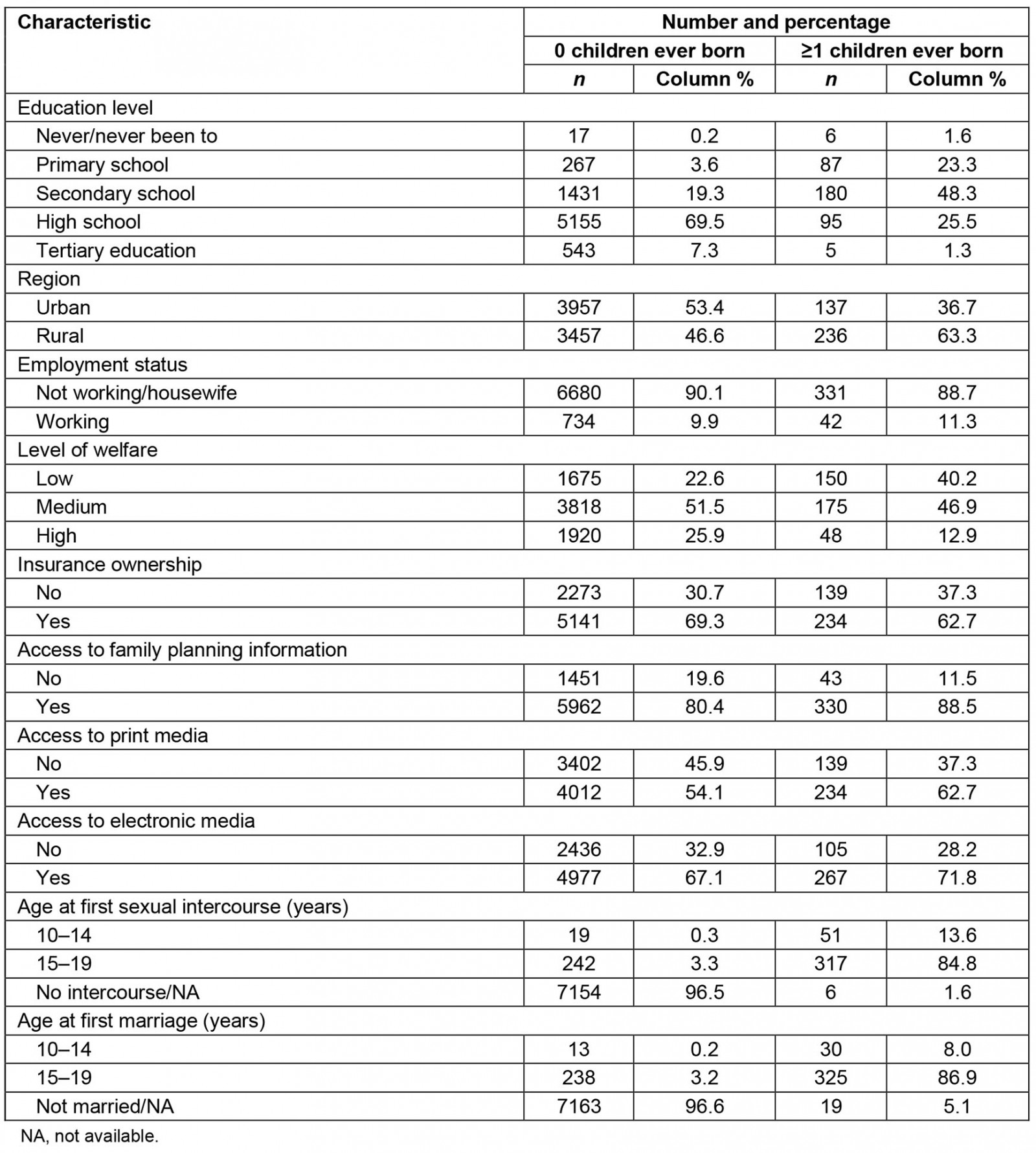
Table 2: Relationships between independent variables and adolescent birth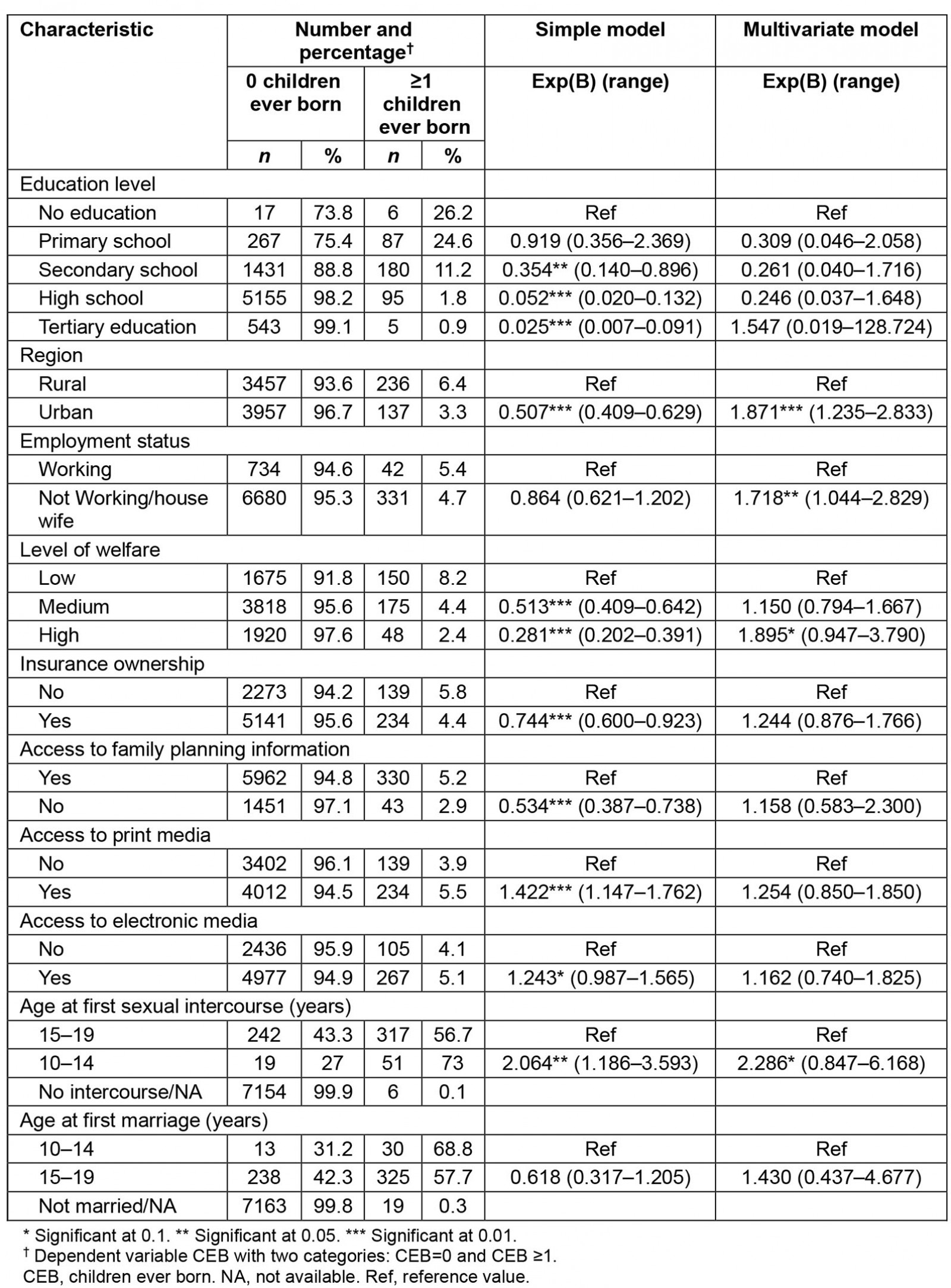
Discussion
Adolescent pregnancy is an event in teenage life that can interfere with reproductive health physically, mentally and socially. Complications in pregnancy can lead to maternal and infant mortality. Psychosocially, adolescents are prone to be isolated, feel ashamed, depressed, drop out of school, find it difficult to work and be poor20. The incidence of adolescent births in Indonesia is declining, but is still high.
The study results showed that 5% of adolescent girls have given birth at least once. In the 2017 IDHS, 7% of adolescent girls stated that they had given birth or were pregnant with their first child at the time of the survey.
Adolescent girls in rural areas that have poor education, are unemployed and have poor economic status have a high risk of experiencing birth in adolescence21. This is in line with the results of a study finding that women with higher education tend to delay their first birth22.
A previous study in north-east Ethiopia with a prevalence of adolescent pregnancy of 28.6% showed that one of the influencing factors was residence in rural areas23. Based on the previous research, this was because the exposure of adolescents to information about reproductive education remains low in rural areas24. Research conducted in South Florida stated that several pregnancies in rural areas were due to low socioeconomic conditions and poorly educated parents, unequal adolescent health services and adolescents being cared for by single parents (thus lacking supervision)25. Descriptively, the findings of the present study were likely to have the same pattern as other studies, yet after controlling for these variables, it was found that urban areas and high levels of welfare had a significant effect on adolescent pregnancy. A previous study stated that there was a negative correlation between low income and adolescent pregnancy26. While wealth status affects adolescent birth, the possibility of adolescent birth was 25.5 times higher for adolescent girls whose households were poor and 4.5 times higher for adolescent girls whose households were medium compared to adolescent girls with rich household status8. The economic challenges for pregnant adolescents were also shown in the study27. The results of the study also showed that the average age of pregnant adolescents was 18 years. Approximately one-fifth of all female participants were illiterate or dropped out of primary school. All pregnant adolescents were homemakers with low economic status27. Economic support for adolescent girls is an important aspect that needs to be considered in reducing adolescent pregnancy rates28, although the study showed there was no significant correlation between household wealth status and adolescent pregnancy29.
The present study showed that the level of education did not have a significant effect on adolescent birth. A previous study also stated that education level was not significantly related to adolescent births because it depends on economic status and age at first marriage. In addition, this was due to the lack of reproductive health education in schools. Discussions about the reproductive system are still considered taboo in many countries30. The results of the present study were distinct from previous studies which show that there was an effect of education on adolescent pregnancy31. However, results of the frequency distribution show that most adolescents who had given birth had a junior high school education, while the lowest rate of adolescent birth was among those who were highly educated. This can be taken into consideration to encourage girls who do not intend to continue after junior high school to consider further education. The results of previous studies indicated that highly educated women tend to delay their first birth32. Studies in five countries with the highest prevalence of adolescent pregnancy showed that the level of education affects the incidence of adolescent pregnancy33. Low levels of education and knowledge were related to an increase in risky behaviour. Education can influence a person's decision-making behaviour.
In this study, employment status has a significant effect on adolescent births. This was in line with research conducted in Ghana by Nyarko, which stated that adolescent birth was influenced by employment status. The probability of adolescent birth was found to be 3.98 times higher in women who did not work than in women who work. Nyarko also stated that media exposure affected adolescent birth8. However, in the present study, information and access to media did not have a significant effect on the incidence of adolescent birth in Indonesia. Many relevant media in Indonesia do not fully involve teenagers, thus there is a gap between existing media and the needs of youth34. The previous study showed that health promotion media using applications on mobile phones (the Remaja Sehat app) were more effective than edutainment methods to improve adolescents’ knowledge about reproductive health35.
The study results show that insurance ownership does not have a significant effect on youth fertility. This is in line with previous studies in Central Java, Indonesia, where one of the factors not related to adolescent birth is insurance ownership36.
Adolescents who had their first sex as older teenagers were more likely to experience teenage pregnancy than adolescents who had their first sex at a younger teenage age, according to a Namibian study16. This is in line with the results of the present study, which showed that the age of first sexual intercourse by adolescents had a significant effect on adolescent birth, and the majority of adolescents who had their first sexual intercourse were aged 15–19 years. Likewise, previous studies showed the median age of 17.4 years at first sexual intercourse37. Although the results of this study indicated that age at first marriage did not have a significant effect, a previous study explained that most young women (66% of respondents in their study) felt forced by their parents to undertake early marriage and adolescent pregnancy10. In some parts of Indonesia, there is also a culture of child marriage. BPS noted that areas in Indonesia that have the highest number of child marriages are West Sulawesi, South Kalimantan, Central Kalimantan, West Kalimantan and Central Sulawesi38. Girls entering their teens often drop out of school because their parents force them to marry39. One government effort to suppress child marriage in Indonesia was revising the law on marriage (Indonesia Law Number 16 of 2019), which previously stipulated a minimum age at marriage of 16 years, so that the minimum marriage age was 19 years. The government took the role as prime mover and stakeholder in efforts to prevent adolescent pregnancy40. Cooperation from across sectors has been one of the keys to success in youth health programs41. Results of a cluster randomized controlled trial with longitudinal observations evaluated 2 and 4 years after intervention showed a positive impact on knowledge of sexual and reproductive health, financial literacy and saving behavior yet no effect on basic education or the impact on adolescent birth42. This suggests that longer or more effective program designs are needed to carry out health interventions to prevent high rates of adolescent pregnancy.
The strengths of this study were the source of data using big data from a national survey representative of the population in this study. In addition, the authors were involved in the study design, data collection and processing. A limitation of this study was that it was conducted by processing data obtained from a previous cross-sectional survey. The authors were unable to confirm the temporal relationship between the exposure variable and the outcome. The study did not investigate several known factors from previous research that investigated determinants of adolescent birth, including knowledge, partner’s education and employment status, and history of adolescent birth in the family.
Conclusion
Overall, it can be concluded that the determinants of adolescent pregnancy in Indonesia are work status, level of welfare, region and age at first sexual intercourse (the most influential factor). The results showed that the factor that most influenced adolescent birth was the age at first sexual intercourse: the earlier the sexual intercourse, the greater the risk of adolescent birth. Based on the results of the study, it is suggested that relevant stakeholders design programs like peer education programs and develop an application for youth43,44 to target youth groups of 10–14 years that have limited education, come from rural areas, are unemployed and have low welfare levels.
Information access to media is also important. The results of the study can be used as an evaluation material to improve existing information media by involving youth in making it more effective. To reduce adolescent birth in rural areas, the authors suggest that the central government increase cooperation and coordination with Kementerian Komunikasi dan Informatika (The Ministry of Communication and Information Technology) in filtering information media, especially social media, websites and online games, which are frequently accessed by adolescents. It is also necessary to develop an online message about the important role of parents in assisting their children to access information, especially adolescents in rural and remote areas. At the local government level, the authors recommend optimising the existing programs such as PIK-R (Pusat Informasi dan Komunikasi Remaja/Center of Information and Communication in Adolescents), BKR (Bina Keluarga Remaja/Fostering Adolescent Families), and PKPR (Pelayanan Kesehatan Peduli Remaja/Youth Care Health Service)45 using village finances.
Acknowledgements
We gratefully acknowledge the National Population and Family Planning Board for providing the opportunity given to utilize the 2019 GPAS data and the LPDP (Lembaga Pengelola Dana Pendidikan/Education Fund Management Institution) for financial support.