


Introduction
Approximately 153 020 people will be diagnosed with colorectal cancer (CRC) and 52 550 individuals will die from CRC in the US in 20231. CRC is the fourth most common cancer with the fourth highest cancer mortality rate in the US1. Because of higher prevalence of risk factors, including obesity and limited access to health care, rural residents have a higher incidence of CRC than urban residents (43.9 v 40.1 per 100 000)2. Also, studies have found that rural residents have lower odds of receiving CRC screening than urban residents3 and living in rural communities is associated with late-stage diagnosis of CRC.
Agricultural operators, defined as individuals who ‘maintain crops and tend to livestock’4 are important parts of rural communities. In 2017, there were an estimated 3 400 000 agricultural operators in the US, and about 80% of them were 45 years or older5, 45 being the recommended age for starting CRC screening according to the US Preventive Service Task Force guidelines6. Despite the significant proportions of agricultural operators in the US, to our knowledge, cancer prevention and control efforts focused on increasing CRC knowledge and screening among agricultural operators have not been undertaken.
In Nebraska, the age-adjusted CRC incidence rate was higher (42.9 per 100 000) than the US average (38.0 per 100 000) during 2014–20187. Similarly, in Nebraska, rural primary care patients have been found to be less likely to be up to date on CRC screening than their urban counterparts (74.4% v 88.1%)8. Agriculture plays an important role in the lives and economy of Nebraskans. The state’s farms and ranches utilize 45 million acres or 92% of the state’s total land area, one in four jobs in Nebraska is related to agriculture, and cash receipts from farm marketing contributed more than US$21 billion (A$33 billion) to Nebraska’s economy in 20189. There were more than 77 000 agricultural workers in Nebraska in 2017, of which 60 000 (77%) were 45 years or older10.
Previous rural cancer research suggests that it is important to incorporate education into CRC screening interventions to increase cancer screening rates11-13. As a first step towards developing culturally tailored educational materials for the agricultural population, in this study, focus groups were conducted among agricultural operators in Nebraska to investigate barriers and facilitators of CRC screening.
The focus groups in this study were guided by the concept mapping14 approach in order to engage participants and enhance the generation of ideas and opinions regarding CRC screening. Concept mapping is a mixed-methods approach based on brainstorming by participants with minimal interference by facilitators. Participants’ ideas generated from the brainstorm are then grouped and ranked to produce a quantitative measure of importance or other metric of interest to the researchers, which can be used in statistical analysis and visualization. The qualitative data (ie themes generated from the transcribed focus group discussion and debate) are combined with a quantitative measure summarizing the data. Concept mapping is a less common approach employed in cancer prevention and control, and to our knowledge, there has been no published research that used concept mapping with agricultural operators. This study used the concept mapping approach to explore cultural issues affecting the use of CRC screening and inform future education and prevention efforts among agricultural operators.
Methods
Conceptual framework
A comprehensive review of relevant empirical literature and health education theories was conducted, and a conceptual framework of shared decision-making about CRC screening by Christy and Rawl was selected as the basis for the model used in this study15. The original model by Christy and Rawl included patient characteristics, cultural beliefs, provider/healthcare system variables, health belief/knowledge/stage of adoption variables, and shared decision-making between patients and providers. This model was adapted for this study (Fig1) by removing patient–provider interaction-related variables because this study was conducted in community settings, not in clinical settings.
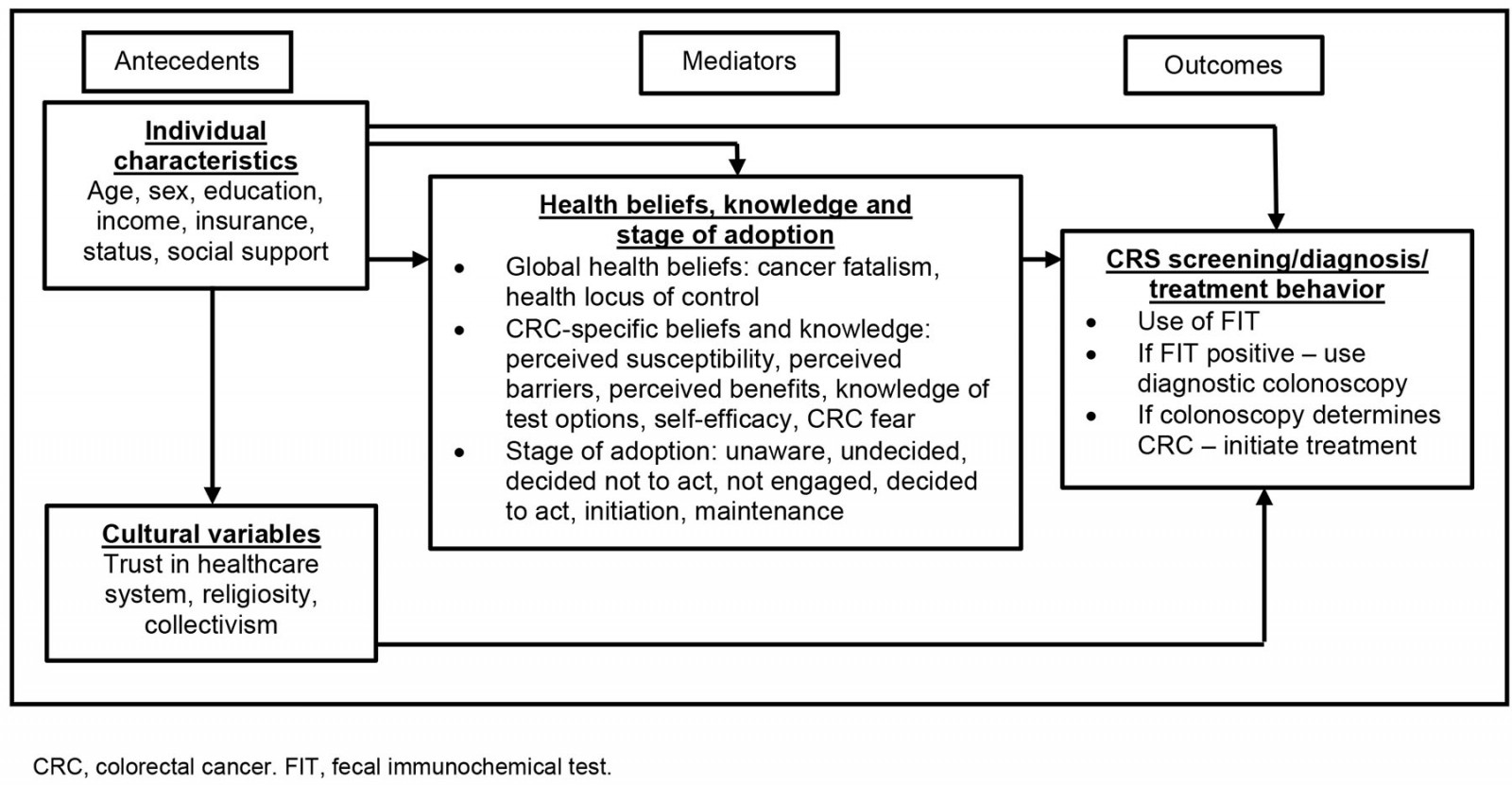 Figure 1: Conceptual framework about CRC screening, diagnosis and treatment.
Figure 1: Conceptual framework about CRC screening, diagnosis and treatment.
Study design and participants
This was a focus group study conducted among agricultural operators in Nebraska. Inclusion criteria for focus group participants were as follows: agricultural operators in Nebraska aged 45 years or older. The cut-off point of age 45 years was used based on the recent CRC screening guidelines published by the US Preventive Services Task Force6. A total of 14 participants were recruited through the agricultural extension program. The agricultural extension program has a list of agricultural operators who participate in various educational programs. The extension program used flyers, phone calls, emails and word-of-mouth to recruit participants.
Two focus groups (one for men and another for women) were formed. Although agricultural operators are predominantly male, one focus group of female operators and a separate group of male operators were formed because gender is a factor that influences cancer screening behavior16. Also, women often make healthcare decisions in the family17 and their perceptions about preventive care can be different from those of men18,19. Participants for a female focus group were recruited from a central part of the state, whereas participants for a male focus group were recruited from a south-east part of the state.
Data collection
Semistructured interview guides were developed based on the conceptual model shown in Fig1. Topics included attitudes and knowledge towards CRC and CRC screening and barriers and facilitators to receiving CRC screening. Focus groups were conducted in-person at a facility that is often used by agricultural operators. The focus groups lasted approximately 60 minutes. To encourage open discussion on the sensitive topic of CRC screening, a female facilitator was assigned to the female focus group and a male facilitator was assigned to the male focus group. A US$50 (A$78) gift card was mailed to participants following the focus group. The female focus group was audio-recorded and transcribed verbatim. The male focus group was not recorded as the men were not comfortable being recorded; thus, since no transcript was generated, the facilitator’s notes were used for data analysis.
Focus group implementation and analysis
A concept mapping approach was used because it is designed to quantify and summarize ideas14. Concept mapping is ‘a type of structured conceptualization which can be used by groups to develop a conceptual framework which can guide evaluation or planning’14. It is an extension of card-sorting methods in qualitative analysis. The guideline developed by Trochim was followed to conduct the concept mapping process, but participants were not asked for a follow-up meeting14.
Step 1 (Preparation) included two tasks. The first task was to select participants. Eligible individuals were recruited via extension partners. As mentioned previously, the extension program has broad reach among agricultural operators through existing outreach networks and educational activities. The second task was to develop the focus on topics. The participants defined the focus for the brainstorming session using open-ended prompt questions.
For step 2 (Generation of statements), a primary prompt for the focus group was ‘Why would you choose to be screened for CRC?’ Participants were encouraged to brainstorm and generate many statements related to perceived control over their risk of cancer; trust in the healthcare system to provide reliable information about their risk of CRC; the perceived difficulty of CRC screening; and personal views of the barriers to screening. The conversations were guided to a discussion of the type of messaging to which they would be most receptive. The facilitators recorded the statements on a whiteboard as they were generated so that all members of the group could see the statements and build on the ideas. Once a final set of statements was generated, the group examined the statements for editing considerations to clarify wording and remove duplicates. Final editing was done jointly by the participants and the facilitator.
For step 3 (Structuring of statements), information about interrelationships among statements using an unstructured card-sorting procedure was collected14. Participants were asked to sort cards into piles of statements that they felt were similar. They could create as many piles as they desired. Participants were asked to rate each statement within a pile (dimensions of the topic explored). The benefit of this approach is that the responses derive from the participants and can confirm or discount the model in Fig1. Statements made by members of the group were rated individually by the group members and evaluated for their degree of importance. A Likert-type response scale was assigned to indicate how much importance or priority was associated with each statement.
Step 5 (Interpretation of maps) was conducted before moving to step 4. Step 5 involved the facilitator asking each participant to read through the statements for each sorted pile (cluster representing a dimension) and come up with a short phrase or word that seemed to describe or name the set of statements as a cluster. Step 5 occurred prior to step 4 during the initial focus group so that participants would not need to meet again because agricultural operators would not be available for a second meeting.
For step 4 (Representation of statements), using the participant ratings, each statement was analyzed to position it as a separate point on a map. The ratings of participants on each statement were used to create an N´N similarity matrix, which can be plotted on an x–y graph where each point represents the number of participants who gave the statement the same rating. Statements with the most agreement among the group members clustered together and those with the least agreement stood alone on the plot. The statements were partitioned on this map into clusters, which represented higher-order conceptual groupings. Finally, maps were created to overlay the averaged ratings either by point or by cluster. C-Map in the statistical package R was used for these analyses14.
For step 6 (Utilization of maps), the point map, cluster map, and their respective ratings map were used to identify educational targets that would benefit the greatest number of agricultural operators. Educational materials were designed to target the largest cluster of statements with the highest ratings. The goal of these data reduction methods is to provide a participant-driven means to find the most important themes, rate them, and compare them across various subgroups. For this study, results from steps 1–5 only were reported.
One thing to note is that in the male focus group, multidimensional scaling was not used because participants did not rate sorted cards within groups. A k-means clustering analysis was done to understand how the rankings of the statements clustered together and a dendrogram was produced to show the clustering of the statements. The cluster package in R (R Core Team; https://www.R-project.org) was used for these analyses and a dendrogram was used to visualize the results.
Ethics approval
The University of Nebraska Medical Center Institutional Review Board determined that the project was exempt because its purpose was to develop educational materials.
Results
Female agricultural operators
Seven female participants were aged 48–63 years. Six of them reported personal experience with CRC; one participant had been diagnosed with CRC. They brainstormed a total of 14 statements, sorted the 14 statements into similar categories, and labeled them with a theme. Within each category, they ranked the statements on a scale of 1–5, where 1 = least important and 5 = most important. Not all statements were sorted by each participant if they did not find it to be a meaningful statement. Only three ratings were missing in the sorted categories, and these were mean imputed within their sorted pile to not alter the overall mean. The final number of ratings was 98 (14 statements from each of seven participants). Four clusters were identified based on the dendrogram and on the labeling of the statements by the participants (Fig2). The stress value was 0.174, indicating a good fit of the concept map (multidimensional scaling) to the data where lower values are better than higher values in a range of 0 to 1.
The means of the statement ratings ranged from 2.71 to 4.86. Of highest importance (>4 of a possible 5) was experiencing symptoms of CRC, costs, awareness, and family (and personal) history of CRC (Table 1). The multidimensional scaling results showed that the cost domain was most agreed upon as important, followed by experiencing symptoms, awareness, and family (Fig2). The healthcare provider dimension scored lower than other items related to cost, family, and awareness. There were only two statements related to healthcare provider support. All clusters were statistically equivalent (F(3, 10)=0.78, p=0.53). The results suggest that increasing awareness on costs and symptoms of CRC screening would be an important target of educational materials. Participants specifically stated that they wanted encouraging and positive messaging on CRC screening, including why it is important and why they should be screened.
Table 1: Descriptive statistics on rating of importance of statements and cluster description in seven female agricultural operators, 2021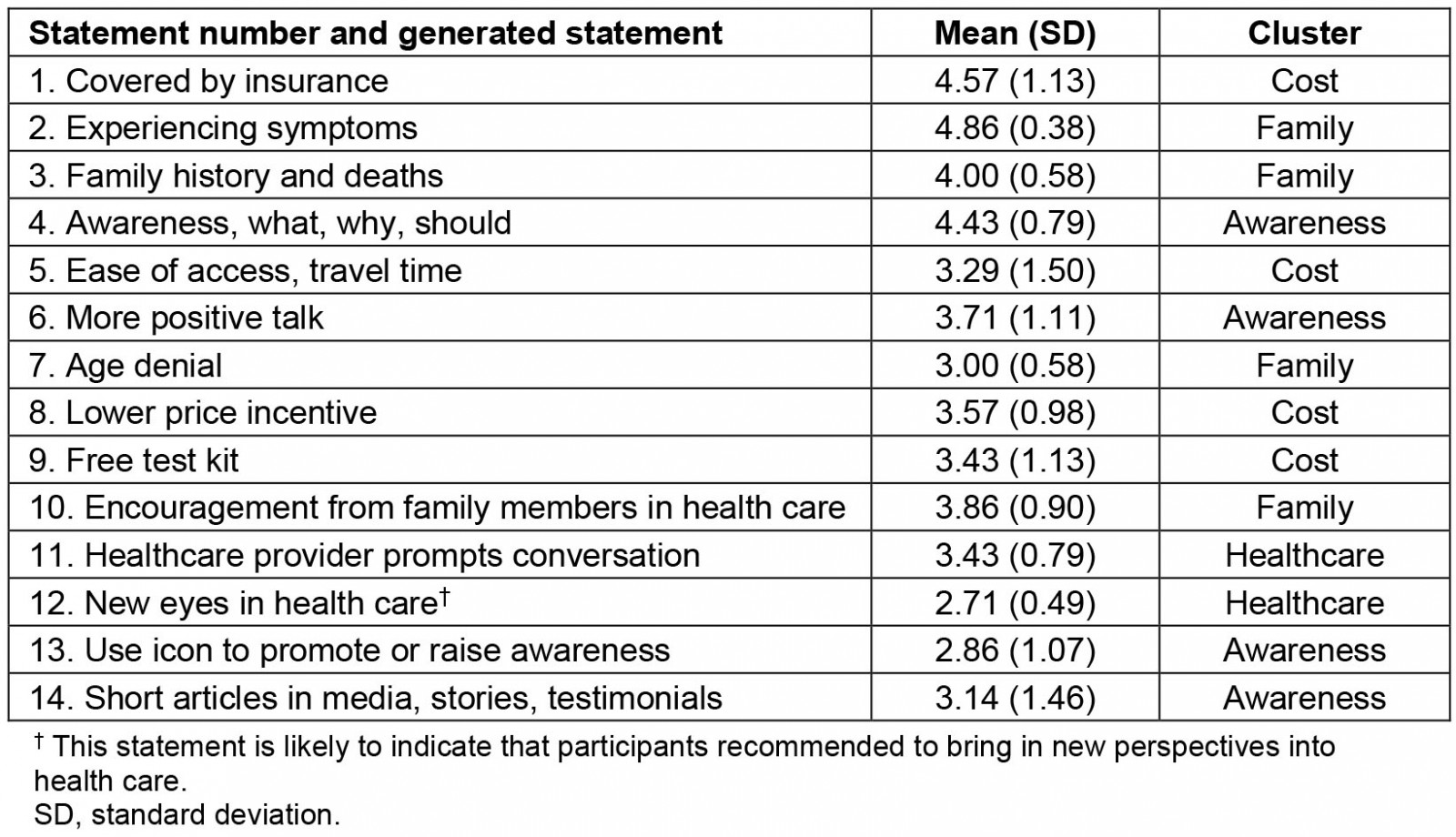
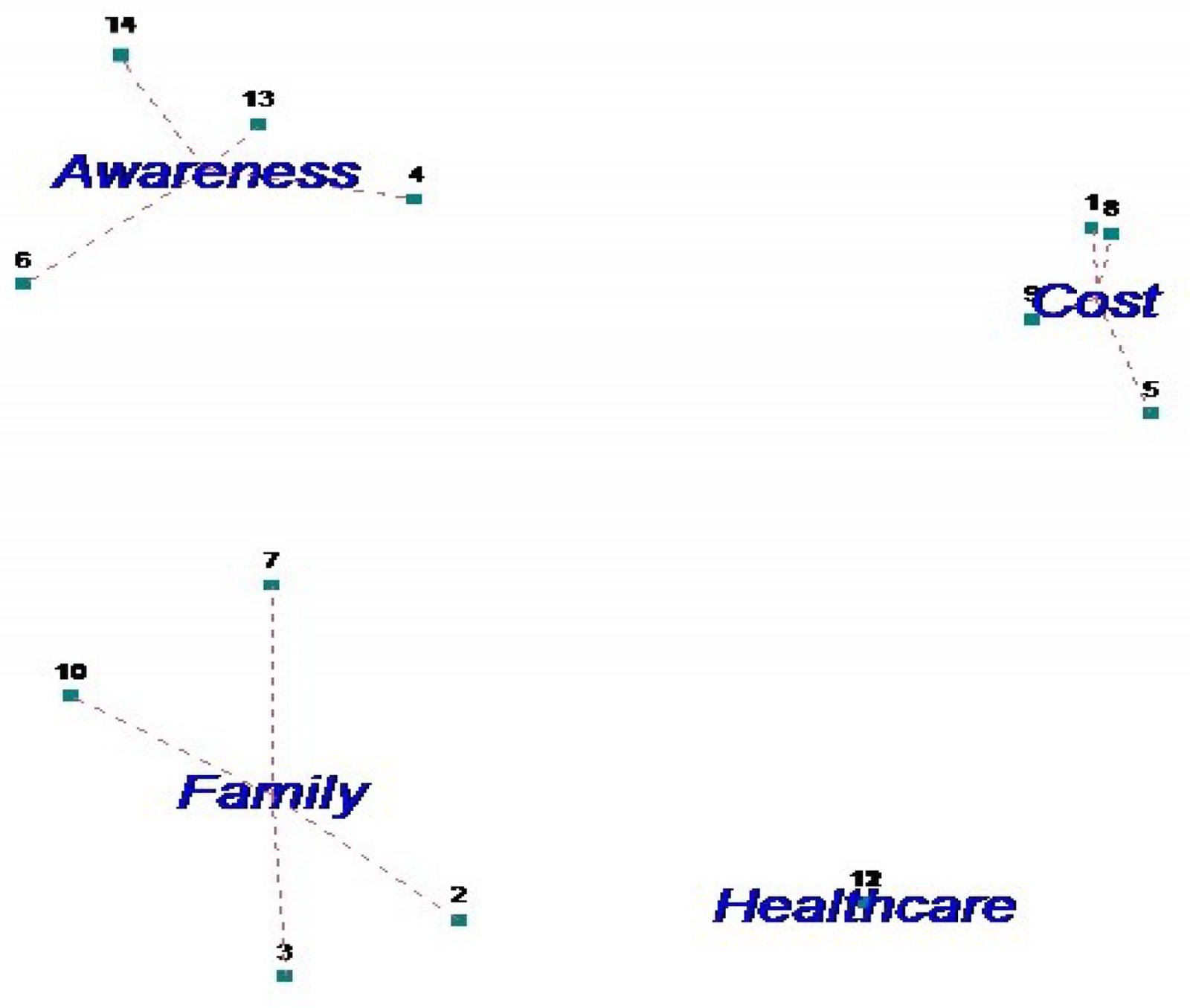 Figure 2: Four clusters from multidimensional scaling results from Nebraska farm women (where points are numbered according to the statement numbers in Table 1).
Figure 2: Four clusters from multidimensional scaling results from Nebraska farm women (where points are numbered according to the statement numbers in Table 1).
Male agricultural operators
The male focus group had seven participants, ranging in age from 58 to 63 years. None reported a personal history of CRC, although several knew people who had been diagnosed with CRC. The group brainstormed 15 statements. The men grouped the statements into two categories/piles (ie barriers and facilitators) and did not use the Likert-type rating scale sorted piles required for concept mapping (Table 2). This focus group provided an example of using the brainstorming approach without the card-sorting approach. Participants said that they had difficulty understanding the instructions and steps to be followed. The result is a one-sample analysis with a total of 15 statements.
The list of barriers and facilitators to CRC screening were ranked as a group by participants and not all participants ranked every statement. Some barriers and facilitators were more important than others. The dendrogram (Fig3) shows that the statements separate into clusters. In the k-means clustering analysis, the first two clusters explained 61.2% of the variance in participant responses. Clusters include family and friend support, feeling as though they are too young to get CRC, family or personal history of CRC, and lack of awareness of the need to be screened. The healthcare provider statements were in different subclusters although the means and standard deviations suggest they were not different from one another. These were not of primary importance in terms of being facilitators. Three items scored as a low priority and clustered together in the dendrogram (workplace support, knowing someone personally who was diagnosed with CRC, and television advertising on Cologuard). The item on workplace support in relation to one’s spouse may be a measure of having health insurance through the spouse’s employment. However, having health insurance was not a statement generated by male participants. The largest subcluster was related to the testing process itself. Male participants were more positive about being tested if their provider was not a personal acquaintance and if their providers encouraged them to get screened for CRC. Pressure from a spouse was in this same cluster.
Table 2: Descriptive statistics on rating of importance of statements and cluster description in seven male agricultural operators, 2022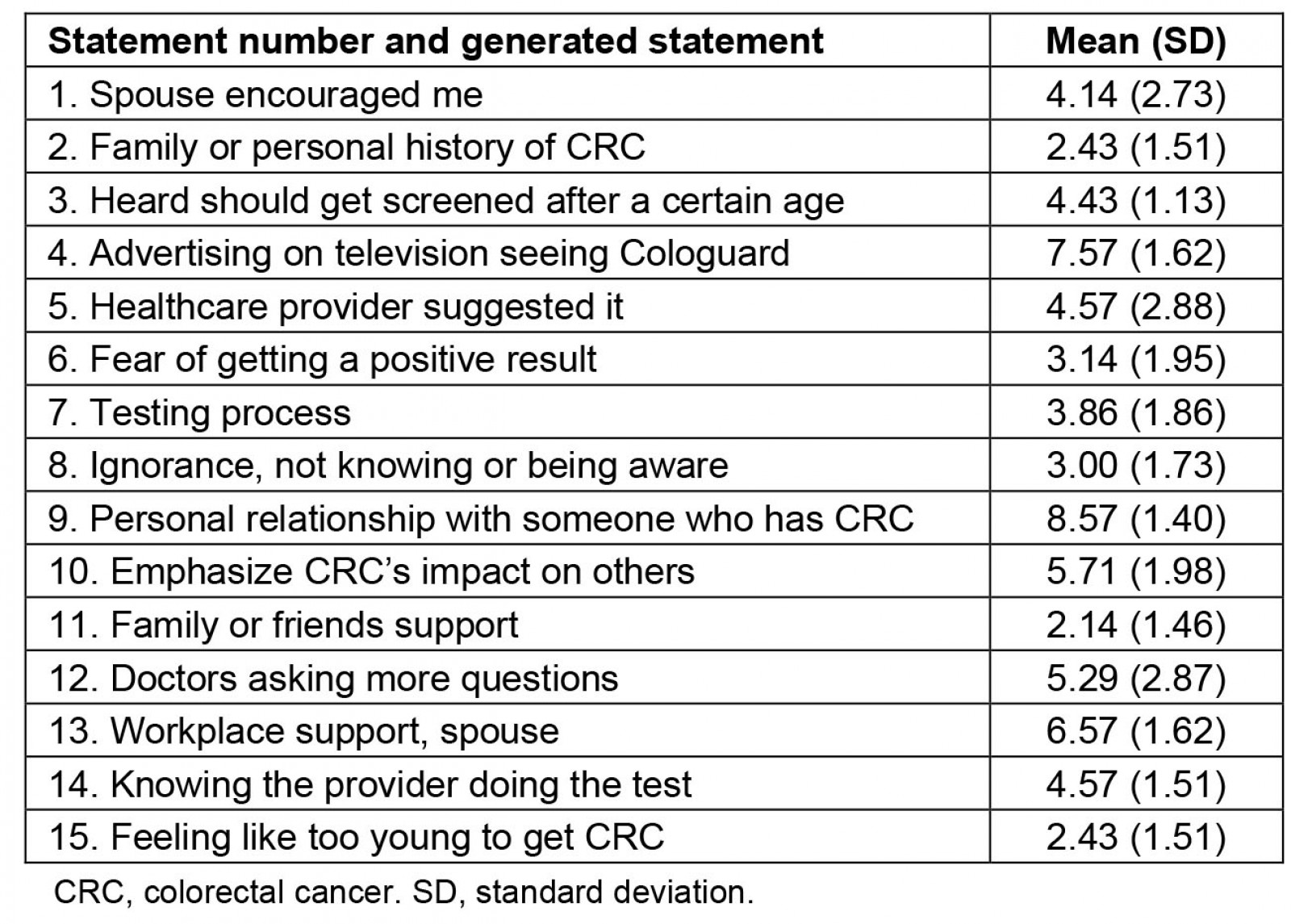
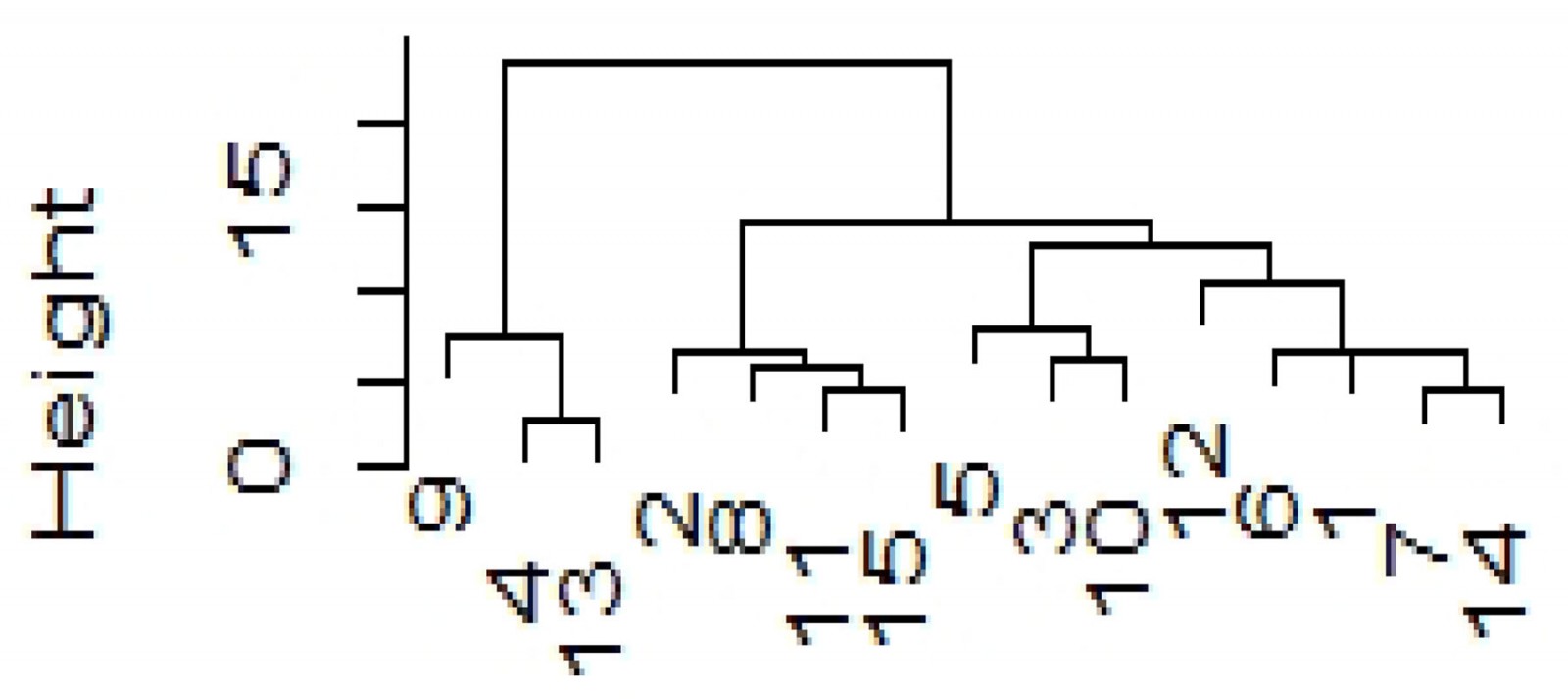 Figure 3: A dendrogram of grouping of statements generated from focus group of seven Nebraska male agricultural operators, 2022 (where numbers represent the statements in Table 2).
Figure 3: A dendrogram of grouping of statements generated from focus group of seven Nebraska male agricultural operators, 2022 (where numbers represent the statements in Table 2).
Conceptual model and alignment with focus group results
Table 3 shows similarities and differences between the perspectives of female and male focus group participants. For example, within the ‘individual’ domain, women perceived that CRC screening may not be completely covered by their health insurance, which discouraged them from getting screened, but men did not mention anything about the financial aspect of screening. On the other hand, it appears for both men and women, getting social support from their family members, friends, and coworkers was an important factor to motivate them to get screened. Within the ‘cultural’ domain, both men and women reported that receiving encouragement or a recommendation from the healthcare provider made a difference for them to get screened. Within the ‘health beliefs, knowledge, and stage of adoption’ domain, both women and men commented about how having a family or personal history of cancer affected their decision to get screened. Also, both men and women mentioned that there is a denial about the recommended screening age – ‘too young to get CRC screening’ and in general, there is a low level of awareness of CRC and CRC screening in their communities. Also, men commented on their fear of getting a positive CRC screening result, and these fears may prevent men from getting screened. Men were far more concerned about the personal embarrassment factor than were women. Men were more comfortable with a colonoscopy if they did not personally know the provider doing the testing. This is understandable in a rural community where there is a lack of anonymity. Women did not raise this same concern. It is important to take these gender-based differences in participants’ responses into account when designing messages for this population.
Table 3: Mapping of focus group concepts to the conceptual model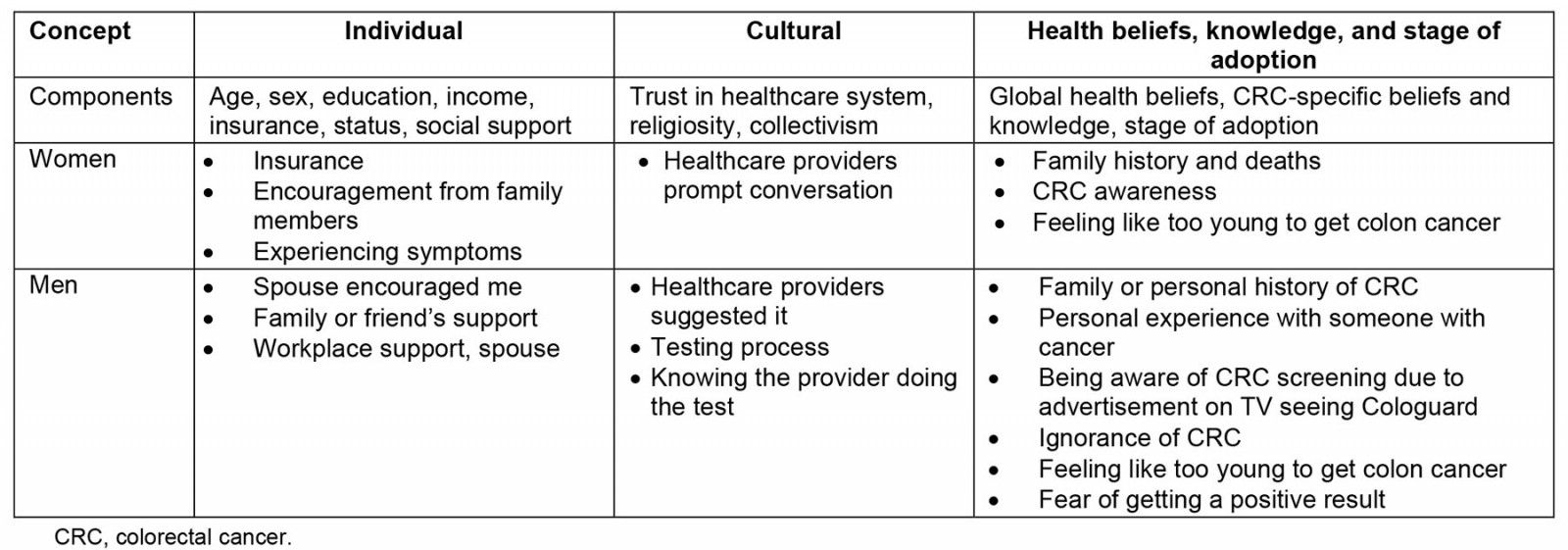
Discussion
Benefits and challenges of using a concept mapping approach
The brainstorming aspects of concept mapping can lead to greater insight and spontaneity in qualitative data because the participants come up with the statements by interacting with each other without prompting or questioning by a facilitator. In this study, the participant-derived statements and their ability to quantify and classify them was useful for the purposes of exploring barriers and facilitators of CRC screening. The card-sorting exercise with the Likert importance rating provided more insight into the groupings among the statements. The multidimensional scaling allowed visualization of what domains the messaging should hit on and how participants could tap into related domains with fewer messages. Although the k-means clustering analysis was not as powerful as multidimensional scaling in identifying key domains for message creation, it provided more insight than simply examining means and standard deviations or using a traditional qualitative text analysis and coding for themes.
There were some challenges with the application of a concept mapping approach. The facilitator needed to be very clear at every step about what the process was and needed to guide participants through it. Preparation was necessary for listing the statements, writing the statements on index cards, sorting the cards, and rating each card within each sorted pile. Also, participants needed to follow instructions at each step and the facilitator needed to explain and even demonstrate how the procedure worked.
Comparison with previous studies
Because this was one of the first published studies that examined the issues related to CRC screening in the agricultural operator population, there are no previous study results that can be directly compared to our results. However, examination of previous research on rural populations provides useful points of comparison. For example, Wang et al conducted a systematic review published in 2019 to identify barriers of CRC screening in rural communities in the US20. They found that most frequently reported reasons for not getting CRC screening were screening cost and lack of insurance coverage, embarrassment or discomfort undergoing screening, lack of knowledge about screening or no perceived need for CRC screening, and lack of physician recommendation. The review also highlighted the need for further research on barriers to CRC screening in rural populations and research on effective strategies to increase CRC screening uptake in rural populations20.
In this study, women reported a concern about insurance not covering the cost of CRC screening completely, but men did not mention anything related to finance. In our study, men said that they were concerned about the CRC testing process, especially about colonoscopy, but women did not express discomfort or embarrassment about CRC testing procedures. One study in 2007 of 70 adults aged 50–75 years in Virginia found that women viewed the preparation for endoscopic procedures as a major barrier to screening while men did not21, and another 2013 study of 2000 adults in Singapore found that more women than men feared a positive diagnosis, were embarrassed, and had pain and risk concerns about colonoscopy22. In our study, both men and women expressed a desire to receive recommendations and support from healthcare providers, which is similar to the findings of the review study by Wang et al20.
Differences between our study and the findings from the review study by Wang et al20 include that agricultural operators emphasized the importance of support from family, friends or coworkers, and family and personal history of (colorectal) cancer as motivating factors to get CRC screening. Agricultural communities are known to be close-knit communities and, therefore, perhaps support from community members plays a more important role in encouraging individuals to get screened23.
Public health messaging
Public health messaging should address the fear of a positive CRC screening result and the anxiety over the testing/screening process. Kotzur et al conducted a survey to identify barriers and solutions to increase CRC screening among 2746 adults in Scotland in 202224. Some of the solutions included increasing the awareness of benefits of early detection, improving the self-efficacy and personal responsibility to take care of one’s own health24. It appears that gender differences in CRC screening do exist across different cultures. In a large trial conducted in Sweden with more than 7000 individuals published in 2020, it was found that women reported more worry, discomfort, and pain than men25. In 2013, Martinez et al, who used data from a screening trial among over 2000 older adults in Maryland26, concluded that gender-specific approaches may be used to promote CRC screening adherence26. For example, a 2011 study conducted in New York of 245 diverse, urban adults recommended providing an opportunity to choose a same-gender provider27, and another 2019 study of 49 535 adults conducted in Germany found that gender-specific design of invitation letters may increase the acceptance of screening colonoscopy28.
Strengths and limitations
The use of concept mapping was primarily for program planning aimed at increasing CRC screening rates in understudied rural, agricultural communities. It was an excellent approach to reduce the amount of qualitative data and to identify important concepts. Ideally, the method can utilize focus groups of larger sizes, which in turn would generate a greater number of statements. However, we found it challenging to recruit agricultural operators; even extensive recruiting efforts by the agricultural extension program via a variety of channels (eg flyers, email, phone calls) yielded a sample size of only seven per group. It appears that the approaches that we used were not extensive or strategic enough to recruit agricultural operators, who are very busy, even in the off-season29, and who may not even have an off-season if their work involves animal operations. Thus, the study findings should be interpreted and generalized carefully to a larger agricultural population. In addition to the need for more robust recruiting methods, attention must also be paid to proper execution of the concept mapping steps. For example, in our study, the lack of sorting of the cards in the male focus group resulted in a lack of information about the priority of categories. Facilitators must be aware of how to guide the brainstorming without taking an active role in the discourse.
Despite these limitations, our study is the first of its kind to explore rural agricultural operators’ views of CRC screening through a theory-driven, mixed-methods strategy (ie concept mapping). Through the concept mapping approach, our study findings showed similarities and differences by male and female agricultural operators regarding their views of barriers and facilitators of CRC screening. Our findings provide critical information in designing culturally tailored and gender-specific educational materials to promote CRC screening among agricultural populations in the US.
Conclusion
Despite the large agricultural populations in rural US communities, dedicated cancer prevention and control programs focused on agricultural operators have not been developed or established. In this study, focus groups were conducted with rural male and female agricultural operators to understand their perceptions about barriers to and facilitators for getting screened for CRC using the concept mapping strategy. Further research may include replications of this study with a larger sample to confirm the barriers and facilitators identified from this study and development and testing of tailored educational messages or interventions for male and female agricultural populations based on findings from the focus group study. In addition, future research may explore potential social network or media platforms that are appropriate for promoting CRC screening for agricultural populations.
Funding
The project described is supported by the National Institute of General Medical Sciences, U54 GM115458, which funds the Great Plains IDeA-CTR Network, and by the National Institute for Occupational Safety and Health’s Agriculture, Forestry and Fishing Grant U54 OH010162, which funds the Central States Center for Agricultural Safety and Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or Centers for Disease Control and Prevention.
Conflicts of interest
The sponsors had no role in the design, execution, interpretation, or writing of the study.
Data availability
The data presented in this study are available on request from the corresponding author. The data are not publicly available because the focus group transcripts may lead to identification of participants.