






Introduction
The emergence of COVID-19, caused by SARS-CoV-2, caused an unprecedented worldwide public health crisis leading to high fatality rates and healthcare system collapse. After the first reports of a severe respiratory disease caused by a new virus in Wuhan, in the Wubei province of China, in December 2019, SARS-CoV-2 spread rapidly and WHO declared COVID-19 a pandemic on 11 March 20201. A few weeks after the initial outbreaks, the first COVID-19 cases were reported in Latin American countries. In Ecuador the first case was confirmed on 29 February 20202, and in October 2020 more than 166 additional deaths per 100 000 people were reported, making Equador one of the countries with the highest number of COVID-19-related deaths during the first wave of COVID-193-5. In the COVID-19 official report from the Ecuadorian government, a total of 77 276 COVID-19 cases were confirmed by PCR between 29 February and 1 August 2020. For the Amazonian provinces included in this study, there were 2055, 1377 and 1186 COVID-19 cases for Morona Santiago, Pastaza and Sucumbios, respectively. By April 2022, the Ministry of Health of Ecuador reported more than 869 449 confirmed COVID-19 cases and 35 594 COVID-19 related deaths6).
There are more than 476 million Indigenous people in the world, representing around 6% of the population. In the Americas, indigenous populations are relatively large, but traditionally neglected 7-14. Some communities, particularly those in the Amazon Basin, are highly endangered and vulnerable to public health threats like COVID-19 due to their extreme isolation and inadequate health infrastructure7,8. In Ecuador, Indigenous Peoples make up about 7% of the total population and are primarily located in underserved rural communities15,16. Since the beginning of the COVID-19 pandemic, reports have been calling for action to protect Indigenous Peoples from the Americas against SARS-CoV-2 spread7,8,10,14. Unfortunately, the threats were confirmed in countries like Ecuador where Indigenous populations had the highest level of additional deaths during the COVID-19 pandemic, and preliminary studies reporting COVID-19 community transmission from the early stages of the pandemic were published3,7,8,10,15.
This work is a retrospective cross-sectional study of the demographics and SARS-CoV-2 detection rate and viral loads during the first wave of the COVID-19 pandemic in 21 Indigenous communities from Ecuadorian Amazonia. The data were retrieved from the COVID-19 surveillance inter-institutional program carried out from June to August 2020 including isolated and endangered communities from Waorani, Siona, Kichwa, Kofan and Shuar ethnicities.
Methods
Study design and setting
We carried out a retrospective analysis of previously collected data in a cross-sectional COVID-19 surveillance program among Indigenous communities from the Amazon region of Ecuador from June to August 2020. A total of 21 communities from five Ecuadorian ethnicities distributed among three Ecuadorian provinces were included in the study. Two ethnicities, Kofan and Siona, were located in Sucumbíos province, and two communities from both ethnicities were included in the testing. In Pastaza province, three communities from the Kichwa ethnic group and eight communities from the Waorani community were recruited. Shuar individuals were distributed among six communities in Morona Santiago province (Fig1). All the individuals willing to be tested at each community were tested, and symptomatology was not an inclusion criteria. Four age groups were defined to classify positive cases as follows: children (0–14 years), young adults (15–39 years), adults (40–59 years), and elders (>60 years). Because the current study is a retrospective analysis of a previous COVID-19 surveillance intervention, the researchers authoring this manuscript were not involved in the individual recruiting criteria.
Sample collection, RNA extraction and RT-qPCR for SARS-CoV-2 diagnosis using the CDC protocol
The samples were processed in the Universidad de Las Americas laboratory (Quito, Ecuador), certified by the regulatory agency from the Ministry of Health of Equador for SARS-CoV-2 diagnosis. Nasopharyngeal swabs were collected in 0.5 mL TE pH 8 buffer for SARS-CoV-2 detection by RT-qPCR, following an adapted version of the US Centers for Disease Control and Prevention from USA (CDC) protocol by using PureLink Viral RNA/DNA Mini Kit (Invitrogen, https://assets.thermofisher.com/TFS-Assets%2FLSG%2Fmanuals%2Fpurelink_viral_rna_dna_man.pdf) as an alternative RNA extraction method and CFX96 BioRad instrument (BioRad, https://www.bio-rad.com/es-ec/product/cfx96-touch-real-time-pcr-detection-system?ID=LJB1YU15)17-22. Briefly, the commercial kit RT-qPCR FDA EUA 2019-nCoV CDC kit (FDA, https://www.fda.gov/media/134922/download) was used for SARS-CoV-2 detection. This kit is based on the WHO-endorsed CDC protocol, targetting the viral genes N1 and N2, with RNase P included as a quality control for RNA extraction17,18. Also, negative controls (TE pH 8 buffer) were included as controls for carryover contamination, one for each set of RNA extractions, to guarantee that only true positives were reported. For viral loads calculation, the 2019-nCoV N positive control (IDT, https://www.idtdna.com/pages/landing/coronavirus-research-reagents) was used, provided at 200.000 genome equivalents/µL, and a factor of 200 was applied to convert the viral loads to genome equivalents/mL and then converted to logarithmic scale (log10 genome equivalents/mL).
Statistical analysis
For the statistical analysis of data, positivity or infection rates were calculated for each ethnic group and each community within each ethnic group, as well as across different sex and age groups. All rates were calculated as proportions from the total samples of each group, and the 95% confidence interval (CI) is provided. To assess significant differences in the positivity rates among ethnic groups, sex and age groups, a χ2 test for comparison of proportions was applied. Moreover, viral load data among age groups, sexes and ethnic groups were compared using non-parametrical Kruskal–Wallis and Wilcoxon tests to compare means. All statistical analyses were carried out using R v3.6.1 (R-Project, https://cran-archive.r-project.org/bin/windows/base/old/3.6.1/).
Ethics approval
All participants signed an informed consent to participate freely and voluntarily in the molecular diagnosis of SARS-CoV-2. The informed consent clearly specified that the nasopharyngeal swabs would be exclusively used for SARS-CoV-2 diagnosis. No further analysis was performed on those samples. (This was included in the institutional review board (IRB) request for the study to be conducted according to national regulations for the Indigenous population in Ecuador.) This study is a secondary analysis of the anonymized laboratory results from a previous surveillance testing done in the context of the COVID-19 pandemic. Nevertheless, the study was approved by the IRB of Hospital General San Francisco (Quito) with code CEISH-HGSF-2021-002. Additionally, this study agenda was carried out in consultation with Indigenous communities and results were reported back to these Indigenous communities as soon as they were available.
Results
Geographic and demographic features of the study population
From June to August 2020, a total number of 853 individuals belonging to 21 different Amazonian Indigenous communities were tested for SARS-CoV-2 infection by RT-qPCR. The Amazonian communities were distributed among three Ecuadorian provinces: Sucumbíos, Pastaza and Morona Santiago (Fig1). The five Amazonian ethnic groups included were Kichwa (249 individuals), Kofan (82 individuals), Shuar (159 individuals), Siona (130 individuals) and Waorani (233 individuals) (Fig2). The age and sex distributions for the study population are shown in Figure 2.
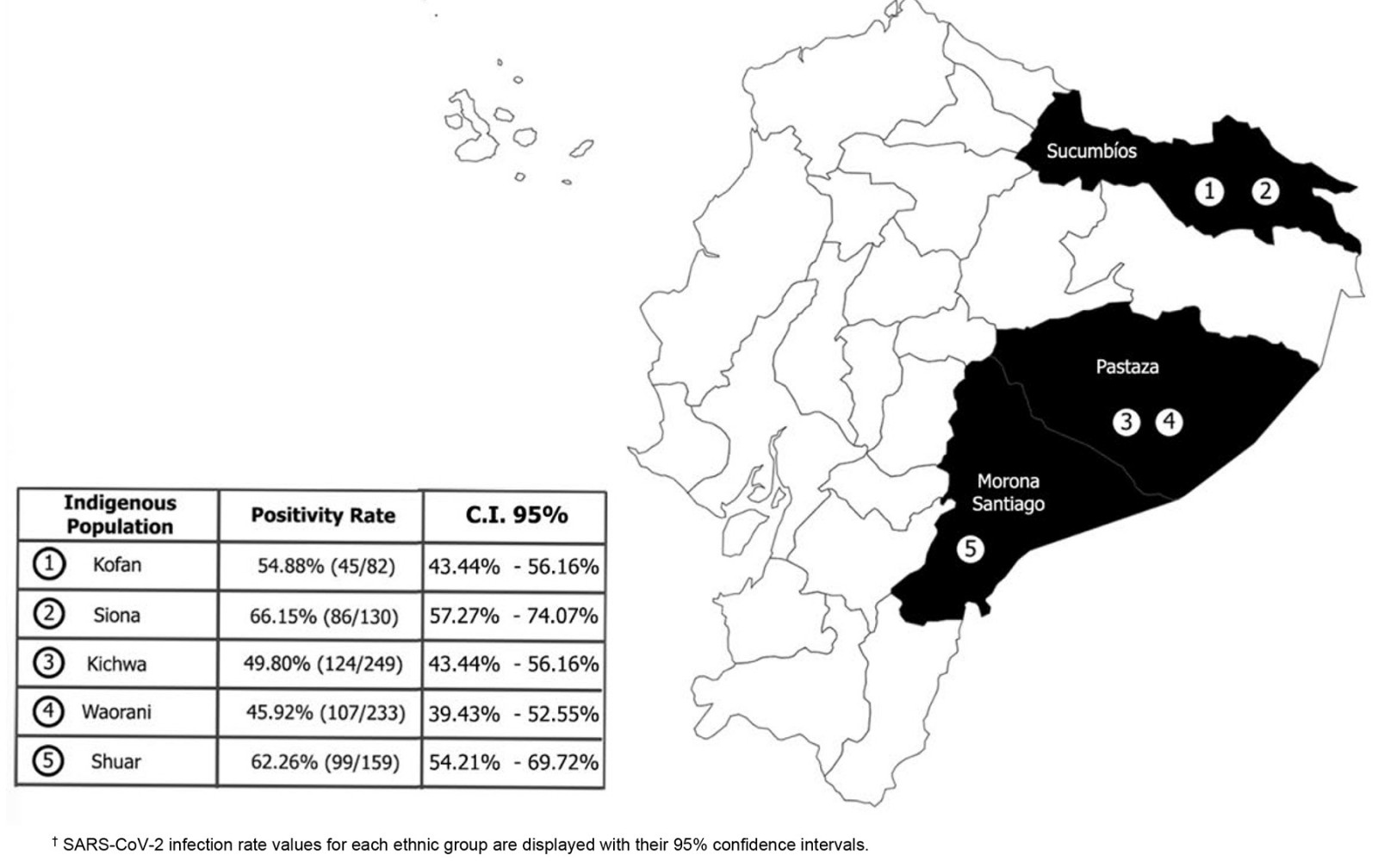 Figure 1: Location within Ecuador of Amazonian Indigenous communities included in the study (Sucumbios, Pastaza and Morona Santiago provinces)†.
Figure 1: Location within Ecuador of Amazonian Indigenous communities included in the study (Sucumbios, Pastaza and Morona Santiago provinces)†.
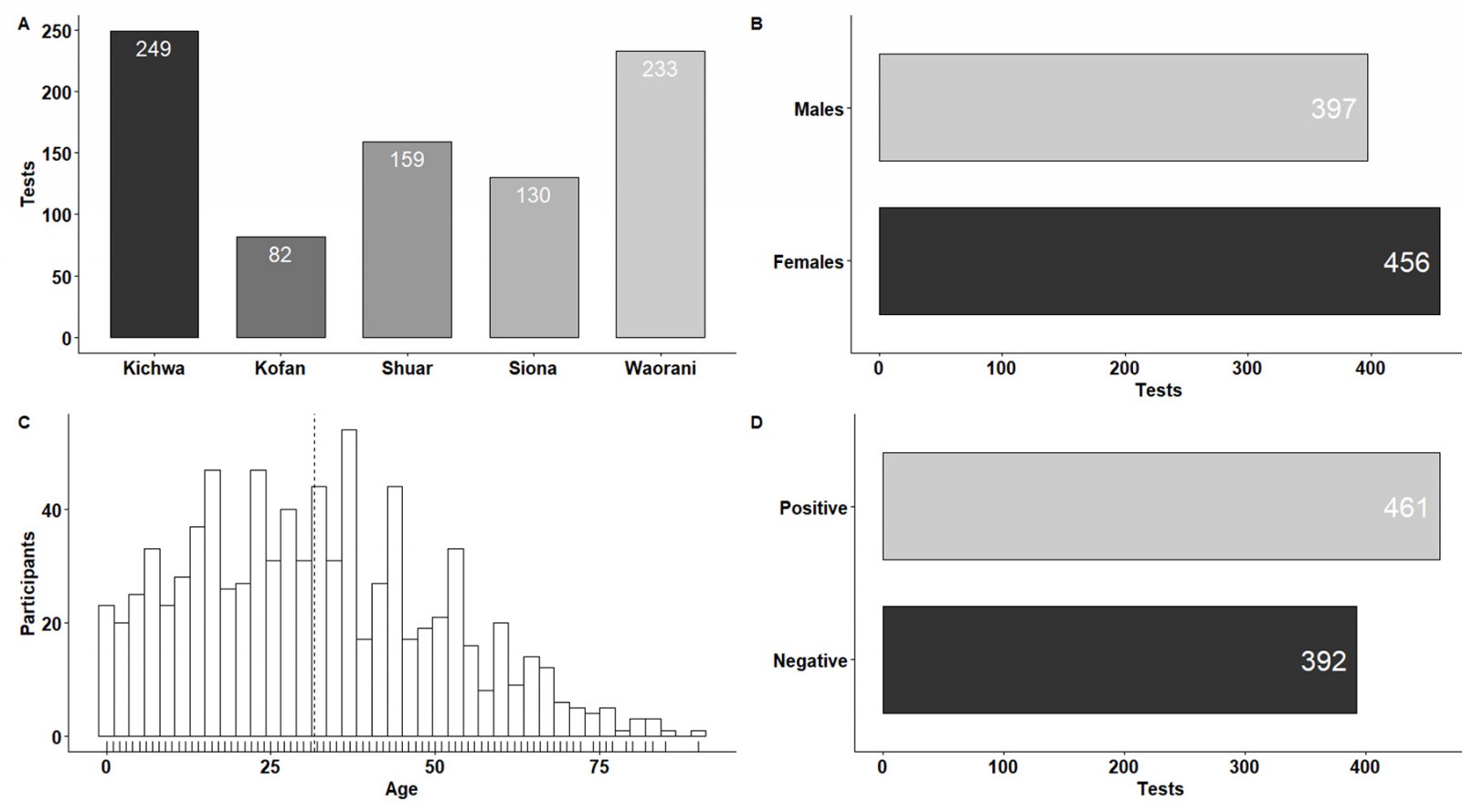 Figure 2: Characteristics of the study population. (A) Number of SARS-CoV-2 RT-qPCR tests applied in the different Amazonian ethnic groups. (B,C) Sample distribution according to age and sex of participants. (D)
Figure 2: Characteristics of the study population. (A) Number of SARS-CoV-2 RT-qPCR tests applied in the different Amazonian ethnic groups. (B,C) Sample distribution according to age and sex of participants. (D)
Absolute frequency of positive and negative SARS-CoV-2 individuals.
SARS-CoV-2 infection rate and viral loads for different age and sex groups
The overall SARS-CoV-2 infection rate was 54.05%, as 461 individuals tested positive for SARS-CoV-2 detection by RT-qPCR (Fig2). The sex and age distributions for the SARS-CoV-2 positive individuals are shown in Figure 3. The SARS-CoV-2 infection rates for females and males were 52.41% (95%CI 47.72–57.07%) and 55.92% (95%CI 50.88–60.85%), respectively, with no significant association found between positivity rates and sex distribution.
The mean age and standard deviation for positive cases was 31.11±0.86 years. The SARS-CoV-2 infection rates for the age groups were 54.80% for children (95%CI 47.17–62.23%), 55.72% for young adults (95%CI 50.71–60.62%), 53.81% for adults (95%CI 46.59–60.88%) and 44.16% in elders (95%CI 33.00–55.90%); no significant association was found between positivity rates and age groups.
Concerning viral load distribution in the study population, 29 individuals (6.2% of the SARS-CoV-2 positive ones) had viral load values greater than 108 copies/mL. A total of 13 of those individuals (44.8%) were in the young adults group (Fig4).
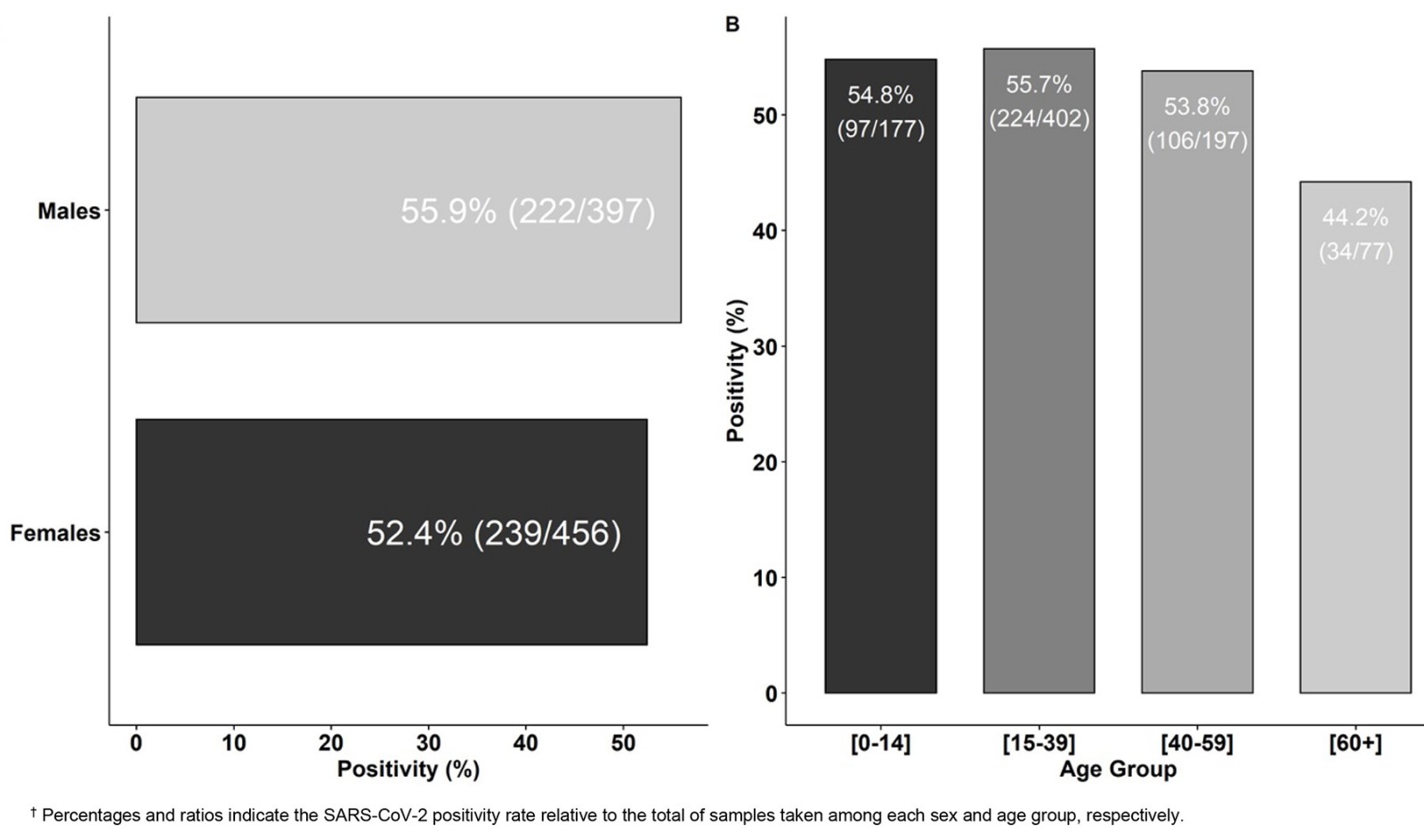 Figure 3: Distribution of SARS-CoV-2 positive cases according to (A) sex and (B) age in the Amazonian Indigenous communities included in the study†.
Figure 3: Distribution of SARS-CoV-2 positive cases according to (A) sex and (B) age in the Amazonian Indigenous communities included in the study†.
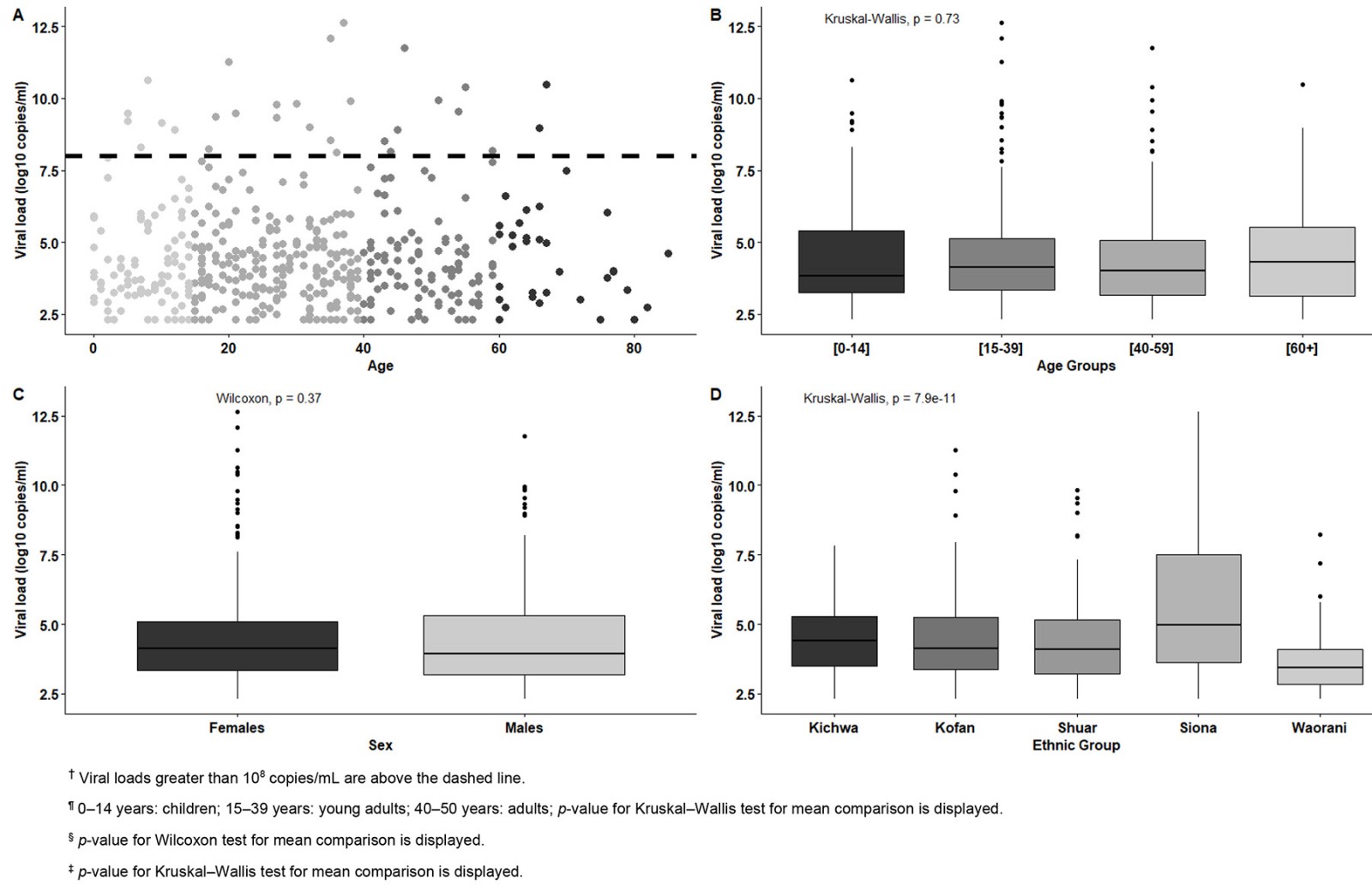 Figure 4: (A) Distribution of SARS-CoV-2 viral loads (log10 copies/mL) according to (A) age†, (B) age group¶, (C) sex§, (D) ethnic group‡.
Figure 4: (A) Distribution of SARS-CoV-2 viral loads (log10 copies/mL) according to (A) age†, (B) age group¶, (C) sex§, (D) ethnic group‡.
SARS-CoV-2 infection rate and viral loads for different communities and Indigenous groups
High SARS-CoV-2 infection rates were found among all the ethnic groups (Fig1): 66.15% (86/130) for Sionas, 62.26% (99/159) for Shuars, 54.88% (45/82) for Kofans, 49.80% (124/249) for Kichwas and 45.92% (107/233) for Waoranis. Those differences in SARS-CoV-2 infection rates among ethnic groups were significant (p<0.05). The SARS-CoV-2 infection rate for each community or village within each ethnicity was also addressed. As detailed in Figure 5, the variability of infection rates ranged from 0 to 90% depending on the community or village tested. One Waorani community remained SARS-CoV-2 free. As some villages had very small sample sizes (eg 3–10 individuals), no comparison of positivity rates between communities or villages was performed. However, these results are displayed in Figure 5 as an insight into the disparities in the epidemiological situation even within each ethnic group.
Among the ethnic groups, the highest viral loads were observed in Siona, with 18 individuals having viral loads equal to or exceeding 108 copies/mL, while the Waorani had only one individual with such high levels. Thus, significant association was found between ethnic group and mean viral load (Fig4).
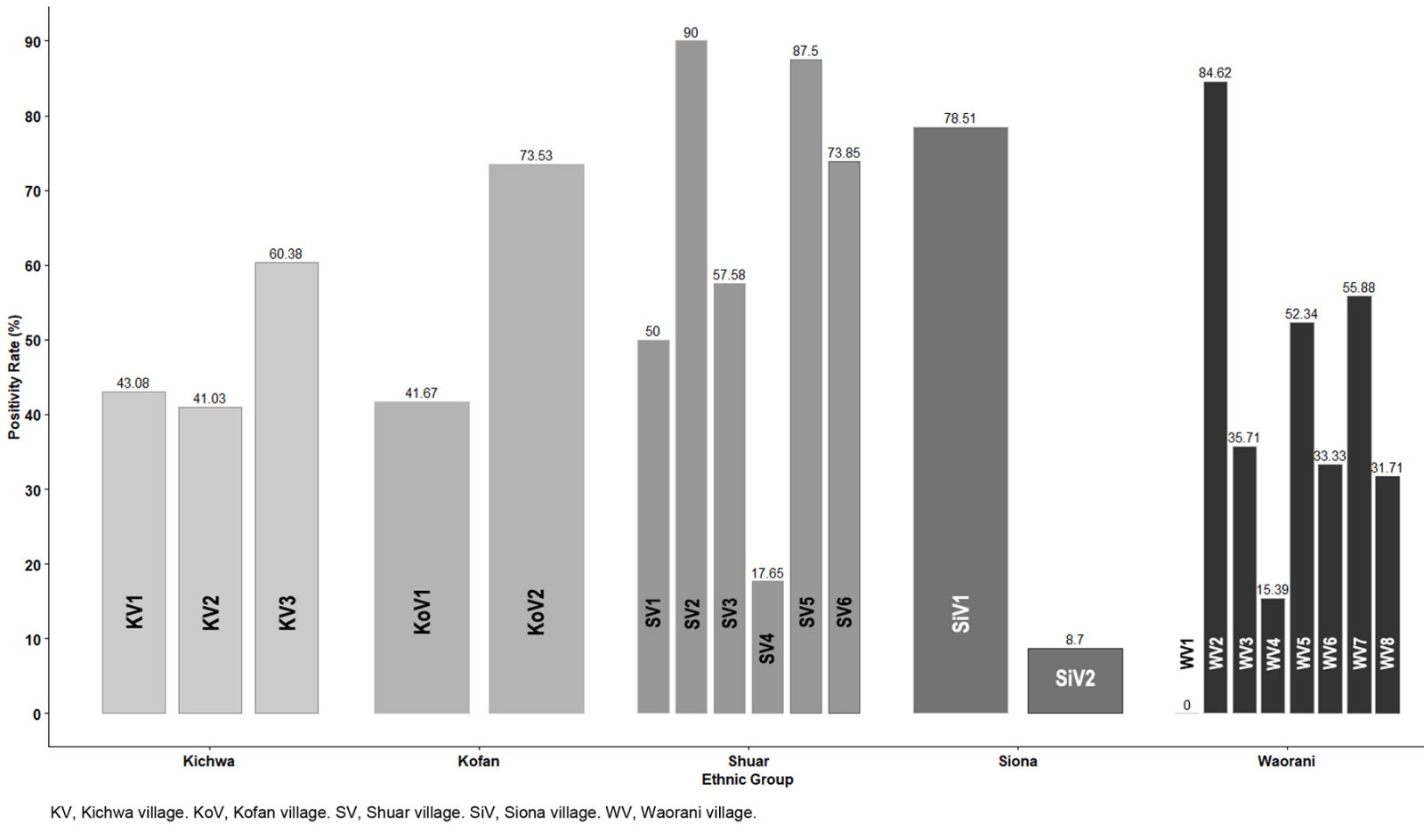 Figure 5: SARS-CoV-2 infection rate values for each village/community among each ethnic group included in the study.
Figure 5: SARS-CoV-2 infection rate values for each village/community among each ethnic group included in the study.
Discussion
The goal of the present study was to address the epidemiological scenario for COVID-19 during the first wave of the COVID-19 pandemic in 2020 for Indigenous communities from the Ecuadorian Amazonia, including isolated and endangered communities from Waorani, Siona, Kichwa, Kofan and Shuar ethnicities. From the early stages of the COVID-19 pandemic, there was a concern among the scientific community about the negative impact on the Indigenous communities of the Americas7,8,10,15. Moreover, those fears were translated into growing evidence of COVID-19 community transmission3,12,23-27 and strong additional mortality rates among Indigenous Peoples3. This scenario is particularly concerning for Indigenous groups in the Amazon Basin, as some of the most endangered ethnic groups inhabit this region12. These Indigenous communities face distinct health and cultural challenges amid the pandemic of SARS-CoV-2, with extreme poverty rates that are triple those of the rest of the Latin American population10,15,28,29. The data presented in this study, where we retrospectively analyzed the results obtained from a COVID-19 surveillance medical intervention in June–August 2020, confirmed the devastating impact of COVID-19 pandemic in the Amazon region. From the 21 communities visited, only one Waorani village remained COVID-19 free for the period covered by this study, while the other 20 communities belonging to five different ethnics groups suffered severe COVID-19 outbreaks. There was no protection associated with the level of isolation of these communities, despite most being accessible only accessible by boat or plane, as has been discussed elsewhere7,8,12. This could be partially due to the concept of isolation, which is conceived from a non-Indigenous perspective. During our visits to these communities, the individuals living there reported to us frequent visits to either communities or to small cities within the Amazonian region of Ecuador, such as Shell, Puyo, Tena and Lago Agrio, sometimes taking several days of walking through jungle forest. Similar findings were reported in Brazil, Peru and Colombia, where COVID-19 outbreaks have been reported for the areas of those countries included within the Amazon Basin11,12,26,30.
As well as specific issues related to neglected ethnic groups in South America, those countries also face the problems associated with low- and middle-income countries more generally, such as poor laboratories and hospital infrastructure. This was translated in a recurrent overflow of critical care units and consistently poor SARS-CoV-2 testing capacity throughout the entire COVID-19 pandemic3,30. In the case of Ecuador, the COVID-19 diagnosis efforts from the Ministry of Health mainly focussed on the hospitalized population31,32. However, several reports have endorsed that community transmission has been happening, affecting community-dwelling asymptomatic or mild symptomatic individuals either from urban occupational risk groups or rural and Indigenous communities not only in Ecuador but also in Brazil, Colombia and Peru3,12,25-28,30-32. The data presented in this study, with an overall SARS-CoV-2 infection rate of over 50%, peaking up to 90% in some Amazon Indigenous villages, point out the limitation of a national COVID-19 surveillance strategy mainly based on symptomatic individuals attending hospital facilities. In the context of Ecuador, this strategy made rural and remote Indigenous communities totally neglected in terms of COVID-19 surveillance. The same idea is endorsed by the striking finding that 6.2% of SARS-CoV-2-positive individuals in this study carry very high viral loads, over 108 virions/mL. These viral loads have been associated with superspreading events33.
The main limitation of our study is that the data used were obtained from a non-random selection of communities, as they were chosen based on requests from the community leaders in the three provinces analyzed, without detracting from the information provided on the spread of SARS-CoV-2 in Indigenous Peoples from the Amazonia. Also, for simplicity in the analysis we excluded the potential effect of clustering of individuals by community in our analysis. This means the results obtained may not fully represent the overall situation in the Ecuadorian Amazon. However, a similar scenario using the same surveillance approach has also been described for other rural and remote communities in Ecuador25,34-36, as well as among Amazonian Indigenous communities in Brazil, Colombia and Peru11,26,30,37.
Our study allows a broader vision of COVID-19 damage produced in Indigenous communities of the Amazon. It therefore establishes that a strengthening of health systems should be carried out with the execution of comprehensive care, epidemiological surveillance and monitoring of infected patients and their families, not only for future pandemics but also for other infectious diseases endemic in the region. In addition, it highlights the need for intercultural surveillance and prevention strategies led by Indigenous community leaders to succeed. The efforts from Indigenous community leaders from the Ecuadorian Amazonia to claim for their protection against COVID-19 made the Ecuadorian public health authorities include ethnic minorities among priority groups for COVID-19 vaccination. Moreover, a special operation was done to vaccinate the members of the Waorani communities living in the borders of the so-called Tagaeri-Taromenane Intangible Zone, to protect the last non-contacted Indigenous groups Tagaeri and Taromenane against COVID-19 outbreaks.
Also, we call attention to the implications of our results under the One Health concept scope. It has been shown that reverse zoonotic transmission from infected humans to pets happened frequently38,39. SARS-CoV-2 transmission has been described for free-ranging dogs living within Amazon Indigenous communities39. Considering the ecological context on our study, an uncontrolled SARS-CoV-2 spread could lead to spillover to wild mammals, generating new viral reservoirs39.
Conclusion
Our study supports that an uncontrolled COVID-19 community transmission was occurring among isolated Indigenous groups in the Ecuadorian Amazonia from the early stages of the COVID-19 pandemic, posing a serious public health threat and an unprecedented risk of extinction to these endangered ethnicities. Public health policies should be revised to prevent those dramatic scenarios in case of future pandemics.
Acknowledgements
This COVID-19 surveillance program was possible through the collaboration of Indigenous organizations and community leaders, non-profit organizations providing aid in the Amazonian region and the Universidad de Las Americas in Quito, where samples were processed for SARS-CoV-2 detection. We especially thank the collaboration of Confederation of Indigenous Nationalities of the Ecuadorian Amazonia in this study. Andres Tapia, co-author of this article, is affiliated to this Indigenous organization.
Conflicts of interest
The authors declare that they do not have any conflict of interest related to this study.
Funding
Fundación CRISFE and Universidad de Las Americas (grant 491.A.XIV.24) funded this study.
References
You might also be interested in:
2021 - Why do some medical graduates lose their intention to practise rurally?
2014 - Differences in media access and use between rural Native American and White children