



Introduction
Children who live in rural Australia experience poorer health, development and education outcomes than those living in metropolitan areas1-4. The latest Australian Early Development Census found that, compared to children living in major cities, regional and remote children have higher rates of developmental vulnerability in all four domains: physical health and wellbeing, social competence, emotional maturity, and language and cognitive skills3. Without treatment, developmental problems such as speech and language delays, behavioural and learning issues, and psychological disorders reduce a child’s capacity to engage in education and can lead to poor literacy, unemployment5, contact with criminal justice systems6,7, and other long-term health and productivity costs8. Treatment and therapy services can ameliorate these impacts, with evaluations showing improvements in educational achievement and significant returns on investment9,10. However, rural and remote communities face a lower availability of health and social services and often need to travel long distances to gain access. Rural and remote families are also more likely to experience socioeconomic disadvantages that make accessing services more challenging2,11. The resulting lack of access can mean that rural children’s health and development needs go unmet.
In Australia, recognition of the key role that schools can play in supporting children’s health and wellbeing is increasing. In recent years, several Australian school-integrated healthcare models that aim to address the needs of less advantaged communities have been established12-16, including school-located nurse models13-15. These models not only co-locate nurses in schools but also integrate them with school learning and wellbeing teams where they work collaboratively with education staff to support children and families. In contrast to historical programs, these models of school nursing focus less on managing acute illnesses and injuries and more on chronic disease, mental health, child development, and disability. Students with these types of problems often require specialist health services, as well as additional educational supports at school. The role of the school nurse in these models focuses on relational practice17 to improve care pathways and coordinate access to appropriate assessments and supports for students18,19.
The School-Based Primary Health Care Service (SB-PHCS), a nurse-led model of care developed in Far West New South Wales (NSW), Australia is one of these newer models. Details of the services’ background, design, and implementation are reported elsewhere15,20. The SB-PHCS integrates health district-employed primary health care registered nurses (PHCRNs) with school learning support teams18. All public schools in NSW have a learning support team. Most include a school counsellor, a specialist learning support teacher, and executive staff. The learning support team identifies and supports children with additional physical, cognitive, social, and emotional needs. This support includes assisting teachers to adjust teaching practices, coordinating additional resources, and liaising with external services21. The PHCRNs work with learning support teams to provide school entry health checks, assessment and care navigation services for children with health and developmental issues, and health promotion for children and families. The strategic positioning of the PHCRNs across the health and education systems allows the nurses to develop relationships with families and education staff to better understand the needs of children, while maintaining connections with the health system to enable effective coordination of care and access to other services.
A qualitative exploration of the PHCRN role found that SB-PHCS nurses use care navigation to reduce barriers to care by addressing elements of healthcare candidacy18. Candidacy theory is a conceptual model of healthcare access that explains the way that eligibility for health care is negotiated between individuals and healthcare services, particularly in less advantaged communities11. To meet their children’s needs, families experiencing healthcare candidacy challenges need support beyond standard ‘assess and refer’ services. This is recognised by the SB-PHCS and reflected in how the service supports families to access services: the PHCRNs not only make referrals, they support other professionals to do so, liaise with services to follow up on referrals and book appointments for families, encourage and support families to attend appointments, and follow up to check that services have been accessed and children’s needs are being met. Qualitative studies provide examples of children who had been identified as needing healthcare services but had not gained access under the standard system; however, when candidacy-focused care navigation was provided, service access was obtained13,18.
While qualitative studies suggest school-located nurse programs can improve access to other healthcare and social services13,18,22,23, quantitative data are limited, particularly in the rural context. This study reviews the electronic medical records of primary school clients of the SB-PHCS and describes the use of assessment, treatment and therapy services of clients who received PHCRN support to access other healthcare services. We consider this data in the context of rural health service accessibility and availability.
Methods
Setting
Broken Hill is a relatively isolated rural community of 17,588 people24 that is 3 hours by road from the next largest community and 6 hours from the nearest capital city. There are six public primary schools, one Catholic primary school, and two public secondary schools in the community. The SB-PHCS operates in all nine schools. Public schools in Broken Hill have below-average Index of Community Socio-Educational Advantage scores, with seven schools having scores below the 15th percentile25. Lower scores indicate greater disadvantage. Broken Hill also has lower levels of educational attainment24 and a higher burden of disease26 compared to NSW averages.
Study design
We conducted a retrospective record review of the Community Health and Outpatient Care program electronic medical records of public primary school children referred to the SB-PHCS for assessment and care navigation during 2019. Cases were followed until 30 June 2020. Children attending secondary school or the Catholic school were not included, because the service was less established in these schools at the time of the study. This substudy examines the records of children who had referrals to other services and who received support from the SB-PHCS to access those services.
Case finding procedures
A list of SB-PHCS clients within the primary school age range who received at least one occasion of service during 2019 was extracted from the electronic medical records system. Research nurses reviewed the Community Health and Outpatient Care program records of children on the list and excluded those who did not have a health or development concern identified, were not attending a public primary school in 2019, or their initial referral to the service was not made during 2019.
Data extraction
Data were extracted by research nurses using a purpose-designed data collection form on the REDCap web platform27 (Research Electronic Data Capture, https://projectredcap.org) hosted at The University of Sydney. Data used in this analysis include:
- demographics (date of birth, sex)
- presenting problems
- challenges to accessing care evident in record
- details of referrals to other services (service, date of referral, type of SB-PHCS support provided, service use).
Presenting problems were coded using the International Classification of Primary Care28. Problems under code ‘P22 Child behaviour symptom/complaint’ were subcoded into ‘speech/language’, ‘behaviour/social’, and ‘learning’ to specify frequently observed issues in this population. For analysis, problem codes were grouped into categories (see Supplementary table 1 for code categorisations).
Evidence of challenges to accessing care documented in progress notes were categorised as family-related or service-related. Family-related challenges included not appreciating the need for care, needing help to identify services, lacking resources such as transport and money, and needing help to communicate with services. Service-related issues included low availability of local services, long waitlists, eligibility criteria and referral pathways, and the skill sets of available practitioners.
Referrals to other services were categorised as ‘SB-PHCS supported’ if the PHCRN had:
- made the referral
- encouraged or supported a third party (such as a teacher or parent) to make the referral
- made a referral to a GP to facilitate a referral to a specialist
- liaised with a service to ascertain and/or negotiate the status of a referral
- followed up with the family to ascertain the status of a referral
- supported the family to act on the referral and attend the appointment.
Details of up to six referrals were collected. This subanalysis examines the records of children who had at least one SB-PHCS-supported referral.
Data were exported from REDCap to the Statistical Package for the Social Sciences v26 (IBM Corp; https://www.ibm.com/products/spss-statistics) for analysis. Data were summarised using descriptive statistics including counts, proportions, and medians.
Ethics approval
Ethics approval for this study was granted by the Greater Western Human Research Ethics Committee (GWAHS 2020/ETH01239). A waiver of consent was approved in accordance with the National Statement on Ethical Conduct in Human Research29, based on the study’s minimal risk to participants, the potential benefits outweighing that risk, and the implementation of appropriate privacy safeguards. All data were de-identified prior to analysis. Given the small size of the community, particular care was taken to ensure that the data presented could not lead to re-identification.
Results
A total of 270 children were referred to the SB-PHCS in 2019, representing 20% of the total enrolments across the six participating primary schools25. Of these, 146 children had at least one SB-PHCS-supported referral, representing 54% of those seen by the SB-PHCS and 11% of total enrolments (Fig1).
‘Speech and language’ issues were the most frequent presenting problem, identified in 37% of children who received support for a referral (Table 1). Descriptions of presenting problems tended to be non-specific, for example ‘speech concern’, ‘behavioural concern’, or ‘mental health’. Examples of specific issues were in relation to articulation problems, anxiety, fine motor skills, problem-solving skills, medication management, and a traumatic event. Evidence of challenges to accessing care were found in 60% of records, with 27% of children who received support for a referral experiencing both family-related and service-related challenges.
The SB-PHCS supported service use for 258 referrals. PHCRNs supported families to act on referrals and attend appointments in a variety of ways (Table 2), the most common being the provision of basic information, support, and encouragement (66% of referrals), making the referral (58%), and following up with the family to check services had been accessed (56%).
Service use was higher for medical and mental health services (75–100%) than for allied health services (39–63%) (Table 3). Available data suggest that a considerable proportion of those referred to full speech pathology and occupational therapy services were still awaiting services at the end of the data collection period (41% and 48% respectively). The median time on a waitlist was 306 days.
Seventy-six percent of referrals for children with family-related (but not service-related) barriers to care resulted in service use during the study period (Table 4). Fewer referrals (68%) for children with service-related (but not family-related) barriers to care resulted in service use during the study period. Referrals for children with both family and service-related barriers had the lowest service use (48%) and highest proportion on a waitlist (36%).
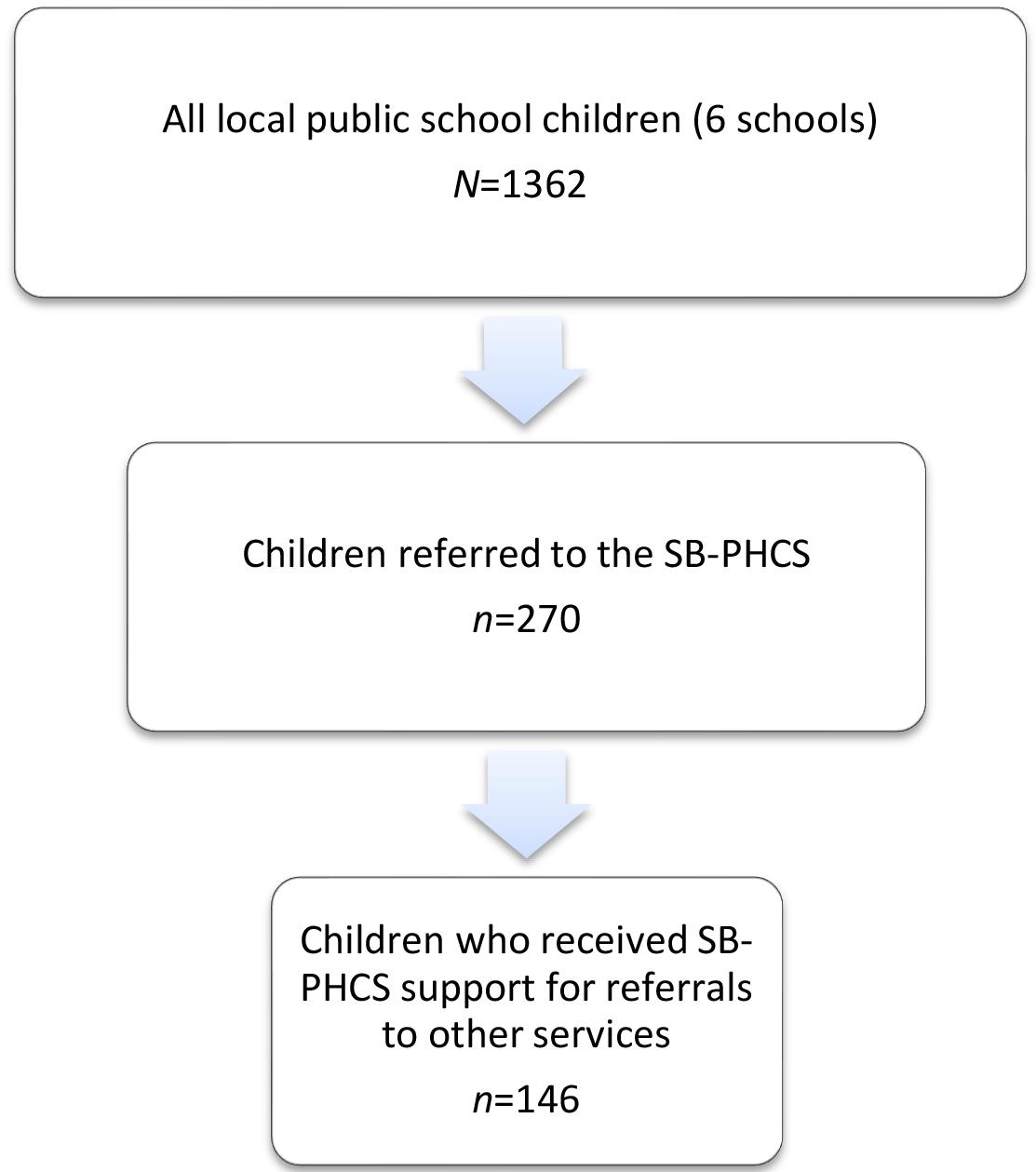 Figure 1: Study population, sample, and subsample of the medical record review of children referred to the School-Based Primary Health Care Service, Broken Hill, NSW in 2019. SB-PHCS, School-Based Primary Health Care Service.
Figure 1: Study population, sample, and subsample of the medical record review of children referred to the School-Based Primary Health Care Service, Broken Hill, NSW in 2019. SB-PHCS, School-Based Primary Health Care Service.
Table 1: Sex, age, presenting problems, number of referrals, and challenges to accessing care of the 146 children with referrals supported by the School-Based Primary Health Care Service, Broken Hill, NSW, 2019
| Characteristic | Variable | n (%) |
|---|---|---|
| Sex | Male | 84 (58) |
| Female |
62 (42) |
|
| Age at referral to SB-PHCS (years) | 4–5 | 58 (40) |
| 6–7 |
33 (23) |
|
| 8–9 |
37 (25) |
|
| 10–11 |
14 (10) |
|
| 12–13 |
4 (3) |
|
| Presenting problem† | Speech/language | 54 (37) |
| Learning |
32 (22) |
|
| Behaviour |
31 (21) |
|
| Metabolic/nutrition |
22 (15) |
|
| Sensory/motor skills |
18 (12) |
|
| Mental health |
16 (11) |
|
| Eyes/vision |
13 (9) |
|
| Unspecified development/behaviour¶ |
13 (9) |
|
| Attention deficit hyperactivity disorder |
7 (5) |
|
| Ear/hearing |
6 (4) |
|
| Family/social issue |
5 (3) |
|
| Asthma |
4 (3) |
|
| Autism spectrum disorder |
4 (3) |
|
| Other§ |
23 (16) |
|
| Number of referrals supported per child | 1 | 81 (56) |
| 2 |
34 (23) |
|
| 3 |
21 (14) |
|
| 4 |
5 (3) |
|
| 5 |
4 (3) |
|
| ≥6 |
1 (<1) |
|
| Evidence of challenges to accessing care (total) |
87 (60) |
|
| Evidence of challenges to accessing care (total) | Family-related challenges only | 29 (20) |
| Service-related issues only |
18 (12) |
|
| Both family and service issues |
40 (27) |
† Individuals could have multiple concerns; totals do not equal 100%.
¶ Occupational therapy need not specified, developmental concern not specified.
§ Dental, diabetes, miscellaneous medical, skin, toileting, sleep, attendance, epilepsy/seizures, allergy.
SB-PHCS, School-Based Primary Health Care Service.
Table 2: Type of support provided by primary health care registered nurses for the 258 referrals supported by the School-Based Primary Health Care Service, Broken Hill, NSW, 2019 (followed to June 2020)
| Type of support provided† | n (%) |
|---|---|
| Basic information, support, and encouragement to attend appointment | 170 (66) |
| Made referral | 149 (58) |
| Provided follow-up | 143 (56) |
| Supported Learning Support Team or another to make the referral | 32 (13) |
| Liaised with service to ascertain and/or negotiate the status of a referral | 29 (11) |
| Booked appointment | 26 (10) |
| Made primary referral (eg to GP) to enable referral | 14 (6) |
† Several types of support could be provided for one referral; percentages do not total to 100.
Table 3: Service use for the 258 referrals supported by the School-Based Primary Health Care Service, Broken Hill, NSW, 2019 (followed to June 2020)
| Service referred to | Number of referrals supported by PHCRN | Number of referrals with documented service access outcome | Service use n (% of referrals with documented outcome) | Median days on waitlist (min–max) | ||
|---|---|---|---|---|---|---|
|
Attended service |
Did not attend service | On waitlist | ||||
| Speech pathology – full services | 24 | 22 | 12 (55) | 1 (5) | 9 (41) | 315 (126–495) |
| Speech pathology – student-led service | 34 | 5 | 4 (80) | 1 (20) | 0 | Not applicable |
| Occupational therapy – full services | 39 | 31 | 12 (39) | 4 (13) | 15 (48) | 299 (32–613) |
| Occupational therapy – student-led service | 13 | 6 | 3 (50) | 0 | 3 (50) | 291 (291–291) |
| Other allied health† | 61 | 27 | 17 (63) | 7 (26) | 3 (11) | 333 (328–473) |
| Mental health services¶ | 41 | 34 | 29 (85) | 3 (9) | 2 (6) | 207.5 (207–208) |
| Paediatrician | 25 | 21 | 17 (81) | 1 (5) | 3 (14) | 167 (109–344) |
| GP | 9 | 8 | 8 (100) | 0 | 0 | Not applicable |
| Other medical specialist | 4 | 4 | 3 (75) | 0 | 1 (25) | Not available‡ |
| Other§ | 8 | 2 | 2 (100) | 0 | 0 | Not applicable |
| Total | 258 | 160 | 107 (67) | 17 (11) | 36 (23) | 306 (32–613) |
† Audiology, dietetics, oral health, exercise physiology, optometry, pharmacy, physiotherapy.
¶ Includes public, private, school-based, and NGO services.
§ Specialist teams/organisations and social/welfare service.
‡ Days on waitlist not able to be calculated due to missing referral date.
NGO, non-government organisation. PHCRN, primary health care registered nurse.
Table 4: Service use for the 258 referrals supported by the School-Based Primary Health Care Service by evidence of challenges to access to care, Broken Hill, NSW, 2019 (followed to June 2020)
| Evidence of challenges to access to care | Number of referrals supported by PHCRNs | Number of referrals with documented service access outcomes |
Service use n (% of referrals with documented outcome) |
||
|---|---|---|---|---|---|
|
Attended service |
Did not attend service | On waitlist | |||
| None | 78 | 35 | 31 (89) | 1 (3) | 3 (9) |
| Family-related challenges only | 57 | 42 | 32 (76) | 5 (12) | 5 (12) |
| Service-related challenges only | 31 | 19 | 13 (68) | 1 (5) | 5 (26) |
| Both family and service issues | 91 | 64 | 31 (48) | 10 (16) | 23 (36) |
| Total | 258 | 160 | 107 (67) | 17 (11) | 36 (23) |
PHCRN, primary health care registered nurse.
Discussion
One in five public primary school children in this rural community were referred to the SB-PHCS for a health or developmental problem. The SB-PHCS supported referrals to other services for just over half of these children, with some requiring support for referrals to multiple services. Thirty-seven percent of children who received support for referrals had speech or language problems, 21% had behaviour problems, and 11% had mental health issues. Our data show that many children in this disadvantaged rural community also face family-related and service-related barriers to accessing appropriate treatment and therapy services.
Sixty-seven percent of supported referrals with a documented referral outcome resulted in service use during the study period; however, 23% were still on a waitlist at the end of follow-up. Speech pathology and occupational therapy, in particular, had high proportions of referrals still on waitlists. Extended wait times not only impact on health and educational outcomes, particularly for developmental problems that limit children’s ability to engage and achieve in school, but are also a source of fear, frustration, and stress for families30. Long waits for these services reflect high demand but also challenges in attracting and retaining allied health professionals to rural areas. During the study period, several public allied health positions were vacant for extended periods, and this is a relatively frequent occurrence. One local response to this longstanding challenge is the establishment of allied health service learning programs31, where allied health students provide services to children, under the supervision of a qualified practitioner. While these programs have gone some way to addressing chronic shortages in rural allied health workforces, gaps remain. Student-led clinics rotate between schools each term but are not available to individual children year-round, and student practitioners are not able to work with children with severe or complex problems. Additionally, in recent years, COVID-19 travel restrictions and cost of living pressures have reduced the number of students who are able to undertake these rural placements. Challenges in recruiting allied health academics to coordinate programs have further limited program activity.
Many children in this study experienced some sort of challenge to accessing care, with almost half of records showing evidence of family-related challenges, including difficulty identifying a need for services, lack of material resources, and low health literacy. A higher proportion of referrals for children with family-related (but not service-related) challenges used the referred service than referrals for children with service-related (but not family-related) challenges. This suggests that the PHCRNs were more successful in overcoming personal barriers to care than system barriers, and is in line with qualitative findings on the PHCRNs’ role in addressing healthcare candidacy. High proportions of referrals with service-related barriers to care were on a waitlist at the end of the follow-up period, reflecting low availability of services.
Addressing candidacy is essential to facilitate service use in less-advantaged groups; however, service use cannot occur if appropriate services are not available. While candidacy theory predominantly addresses person-centred barriers to health care and helps to explain how school-based nurses can facilitate access in less-advantaged populations, Penchansky and Thomas’ access theory offers a lens through which to understand service-centred barriers32,33. The modified dimensions of access map closely to those of candidacy theory, in parts offering the opposite side of the same coin (Table 5). For example, candidacy theory’s domains of ‘navigation’ and ‘permeability’ of services identify the difficulties or ease of use experienced by potential service users, while access theory offers ‘awareness’, ‘adequacy’, and ‘affordability’ to describe the service characteristics that contribute to the service users’ experience. Similarly, candidacy theory’s domain ‘offers and resistance’ is mirrored by access theory’s ‘acceptability’ of services. However, access theory offers two additional domains: ‘accessibility’ and ‘availability’. Accessibility refers to a service that is in reasonable proximity to the prospective client, while availability refers to services having sufficient resources to meet the volume and needs of the community they serve.
School-based PHCRNs are well placed to address the seven domains of healthcare candidacy and some domains of access theory, but they have less influence on the availability and accessibility of treatment and therapy services. The PHCRNs’ embeddedness in the school community and the relationships developed with schools and families allows them to identify issues, help families to recognise that their child requires a health service18,34 (‘identification of candidacy’), and raise awareness of available services in the school community. Their positioning within, and knowledge of, the health system allows PHCRNs to assist families to identify and access available services (‘navigation’, ‘permeability’, ‘acceptability’, ‘offers and resistance’), and prepare families for appointments (appearances at service). The PHCRN may also, to some degree, influence how other service providers assess and interact with families (‘adjudications’, ‘acceptability’, ‘operating conditions’). However, although the SB-PHCS has experienced some success in influencing the accessibility of existing services18,35, PHCRNs’ ability to influence the availability of services is limited. In cases where services are not available, or not able to meet community need within an acceptable time frame, one must ask: are we ‘kicking the can down the road’ by identifying problems and encouraging families to seek further assessment and treatment? Does this break a foundational principle of health screening – that facilities for diagnosis and treatment should be available36?
Addressing the availability of services requires systems-level responses to workforce and other resource challenges to improve service access in rural areas. Given the identified high need for speech and occupational therapy services and their pertinence to education, one solution is the integration of school-based allied health professionals into the SB-PHCS team. The essential role of allied health in education and the value of integrating such services within schools is well recognised in other jurisdictions. In the US, 40% of speech–language pathologists and 13% of occupational therapists work in schools and are directly employed by educational services37,38. This model increases the accessibility of services and allows therapists to work with class groups and influence teaching practices through cross-disciplinary knowledge sharing, thereby building the capacity of the whole educational team. In Australia, the presence of allied health practitioners in schools varies. While Queensland’s and Victoria’s departments of education directly employ therapists to work in public schools39,40, NSW’s Specialist Allied Health and Behaviour Support Provider Scheme requires individual schools to enter into contracts with providers and pay for services from existing school budgets41. This presents a quandary for school leaders about the use of general education funding to provide health interventions, and questions about where the responsibility for these services lies.
In many rural contexts, discussions of models for school-based allied health positions is largely hypothetical because rural and remote areas face the same recruitment and retention issues with these positions as they do for other healthcare roles42. Rather than employing additional providers, some rural communities have improved service accessibility by establishing school-based health centres, where existing community-based services are relocated to deliver care to students and families onsite12
Other approaches suggested by a recent report on improving access to allied health services in rural Australia include models of care that incorporate allied health assistants and/or telehealth42. Telehealth interventions increase service access for rural students, reduce time away from school, and parental burden, and have been found to be feasible and effective43,44. However, concerns have been raised about the risks of telehealth replacing on-the-ground positions in rural communities45, which could remove expertise, knowledge transfer, and ultimately people from regions. Caution must be exercised so that telehealth is employed to complement, rather than replace, local services, ensuring that local capacity is maintained and built. Langbecker et al46 and Lincoln et al47 describe school-based speech and occupational therapy telehealth service models that utilise therapy assistants from within local school communities. Individuals fulfilling these roles included teachers, education support officers, and parent volunteers. Therapy assistants, particularly those whose substantive role was in learning support, felt their participation in the telehealth program helped them to develop knowledge and skills that they could utilise in their work with other students47. This cross-disciplinary knowledge transfer is an additional benefit of such programs that has the potential to improve the educational outcomes of not only of the students receiving individual therapy, but also of other students in the school. A school-based therapy assistant model could also be used to increase the capacity of locally based face-to-face allied health services, boosting rural health workforces and forming part of the rural allied health workforce pipeline48.
Nationally, there is a persistent gap in educational and life outcomes between urban and rural children1,4. Australia is ranked in the bottom third of wealthy countries in relation to levels of educational equality49. Late last decade, the Australian Government commissioned an independent review into rural and remote education4. One of its recommendations was to decrease educational inequities in rural areas: ‘Work needs to be done to drastically shorten the time it takes to have a child with a potential learning difficulty properly assessed and a specific program designed for them’. Health professionals, particularly in allied health, frequently contribute to these assessments and programs. Our findings show that while PHCRNs can facilitate access to services, wait times for allied health services in this rural community are still significant, limiting the service’s ability to improve educational equality for rural children.
Table 5: Domains of candidacy theory, and Penchansky and Thomas’ theory of access and primary health care registered nurses’ ability to address each domain
| Domains of theory | PHCRNs’ ability to address domain | |
|---|---|---|
| Candidacy theory11 | Access theory32,33 | |
|
Identification of candidacy How people recognise that they have something that requires medical attention. Subthemes include normalisation of symptoms, health crisis and lack of preventive health use. |
The relationships developed with schools and families18 enables PHCRNs to identify health and developmental problems, and to assist families to recognise that their child requires a health service. School entry health checks that are integrated with literacy and numeracy assessments also contribute to identification34. |
|
|
Navigation of services The difficulties people face using services. They might not be aware that services exist or experience difficulties trying to negotiate their way into the service. |
Awareness† Communication and information A service maintains awareness through effective communication and information strategies with relevant users (clinicians, patients, the broader community), including consideration of context and health literacy. |
The relationship with families and positioning in the health system18 allows PHCRNs to assist families to identify appropriate services, navigate eligibility criteria, referral pathways, and the practical and logistical aspects of getting to a service. |
|
Adequacy (accommodation) Organisation An adequate service is well organised to accept clients, and clients are able to use the services. Considerations of adequacy include hours of operation (after-hour services), referral or appointment systems, and facility structures (wheelchair access). |
||
|
Permeability of services How easy it is for people to use the services. Services can vary from being impermeable to very porous. Cost can render a service impermeable to vulnerable people, as can low levels of health literacy. |
||
|
Affordability Financial and incidental costs Affordable services examine the direct costs for both the service provider and the consumer. |
||
|
Appearance at services How people make a case for why they require medical attention. |
PHCRNs are able to prepare families to attend appointments and communicate their needs to health professionals. |
|
|
Adjudications by professionals The judgements of health professionals. Vulnerable people may be judged as being less eligible for some interventions or they may be dismissed by the health professional. |
The school-based PHCRNs’ links with the health system can also influence other providers in their assessments of clients’ eligibility for services. |
|
|
Offers and resistance Whether patients agree to accept referrals. |
Acceptability Consumer perception An acceptable service responds to the attitude of the provider and the consumer regarding characteristics of the service and social or cultural concerns. For instance, a patient’s willingness to see a female doctor may determine whether a service is acceptable or not. |
The relationships developed with families enables PHCRNs to work through hesitations and concerns and encourage families accept referrals to services. |
|
Operating conditions The local responses and resources to address the issue of candidacy in the local population. |
PHCRNs represent a key resource to influence how candidacy is addressed in the local system. They not only address candidacy directly with individual patients and families but also influence how other practitioners and services view and interact with patients to enable appropriate service access. |
|
|
Accessibility Location An accessible service is within reasonable proximity to the consumer in terms of time and distance. |
Limited. There has been some success in influencing an existing service to relocate to more accessible locations18. |
|
|
Availability Supply and demand An available service has sufficient services and resources to meet the volume and needs of the consumers and communities served. |
Limited. There is potential to leverage relationships with other services, service data, and in-depth knowledge of community needs to advocate for resources35, but rural workforce challenges and long waitlists remain. |
|
† Added to the original theory by Saurman (2016)33.
PHCRN, primary health care registered nurse.
Limitations
This study used existing medical records that were not designed for the purpose of research. The level of detail documented for each child varied between clinicians, particularly regarding family context, and our identification of challenges to accessing care may be conservative. Service access outcomes were not always documented, resulting in missing data. One school’s SB-PHCS service did not begin until June 2019 and there were changes to services in 2020 due to the COVID-19 pandemic, so our data may not reflect typical activity during the latter part of the follow-up period. The PHCRNs were redeployed during the COVID-19 response for 4 weeks. Some health and social care services also abruptly shifted to telehealth during the last 3 months of the follow-up period, which may have affected some families’ willingness to engage with services.
Conclusion
While care navigation services are essential to improving service access in less-advantaged communities, they are only part of the access puzzle in under-resourced rural communities. Rural health workforce shortages are a longstanding issue and alternate models of care, such as telehealth and the use of paraprofessional staff, need to be considered to fill service gaps, improve access to health services, and reduce inequities in health and education for rural and remote children.
Funding
The Broken Hill University Department of Rural Health is funded by the Australian Government Department of Health. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
Author KHS was employed as a PHCRN in the SB-PHCS and author RS managed the SB-PHCS during the study.
AI disclosure statement
No generative AI or AI-assisted artificial tools were used in the conduct of this research or the preparation of this manuscript.
References
Supplementary material is available on the live site https://www.rrh.org.au/journal/article/9622/#supplementary
You might also be interested in:
2019 - Partnership integration for rural health resource access
2018 - Managing qualitative research as insider-research in small rural communities
2010 - Parental attitudes towards childhood immunizations in Eastern Uganda