



Introduction
Rural health and importance
There are significant differences in health outcomes for those living in rural areas compared to those living in urban areas in Aotearoa New Zealand, and these differences are exacerbated by ethnic disparities1. Differences in health outcomes between urban and rural areas are caused by a range of factors, including but not limited to demographic differences, increased risk factors such as social determinants of health, and ill-designed health systems that are not fit for purpose for rural communities1,2. Currently in New Zealand there is a lack of rural medical professionals, which compounds other health system factors. Pathways for increasing the workforce in regional and rural areas of New Zealand have been implemented in professional health programs at universities. The importance of these pathways to workforce development is due to the strong evidence that students from a rural background have a higher likelihood of working in a rural setting 5 to 8 years following graduation3. Ensuring that rural origin entry pathways appropriately include ‘rural’ New Zealand is therefore critical.
Defining ‘rural’
Currently there is no standard international definition of ‘rural’ for health or education purposes. Commonly, rural areas are defined as those areas that are not urban or metropolitan4,5. The lack of a standard, international definition of rurality has resulted in the development of numerous definitions internationally and in New Zealand. These definitions are usually developed based on a set of (country-specific) criteria. As noted by Hart et al there is no perfect definition of rurality and a certain amount of error is inevitable in any definition6. A poorly chosen definition of rurality may incur bias in research results and may lead to inequitable distribution of resources when applied to policy7.
In the context of rural pathways for professional health programs, a poorly defined rural classification can contribute to inequitable access to educational opportunities for rural students, where the rural pathway can benefit urban students and disadvantage rural students, and not increase rural student numbers. Widening access for students from rural origins is an established concept in increasing the rural workforce3. Additionally, misclassification of rural status through a poorly chosen rural classification can contribute to inequitable access to educational opportunities for students of Indigenous ethnicities, who are often likely to constitute a greater proportion of a rural population and may therefore be more likely to choose to work in rural areas following graduation.
Literature review of ‘rural’ definitions in Aotearoa New Zealand
In the New Zealand context, existing definitions of rurality are commonly based on population data sourced from the official New Zealand censuses. Examples of existing definitions include the current official urban–rural classification, the Statistical Standard for Geographic Areas (SSGA) 20188, and the preceding official classification, the New Zealand Standard Areas Classification 1992 (NZSAC92)8. For these definitions, the classification of locations to urban or rural can change depending on the boundaries of census areas used to aggregate population counts, or changing area geographies between censuses. This can lead to confounding of comparisons of rural and/or urban areas across time, and affect the results of research, commonly known as the modifiable areal unit problem in geography9,10.
Several other urban–rural classifications have been released by the official statistical organisation of New Zealand, Stats NZ. In order to provide a more suitable classification of rurality for research and healthcare purposes, Stats NZ released two classifications based on the SSGA 2018: the urban accessibility classification 2020 (UA 2020)11 and the functional urban areas classification 2021 (FUA 2021)12. These classifications take into account urban influence and urban accessibility, where the SSGA 2018 classification does not. This is similar to a non-official experimental urban–rural area definition, the Urban Rural Experimental Profile (UREP) –released in 2004 and re-released in 2006 by Stats NZ – which also classified areas based on both the workplace and home addresses of residents13. There are also a number of non-official rurality classifications for New Zealand that have not been developed by Stats NZ. These classifications are usually developed to address specific uses, such as health purposes, health research or policy development. One example of this is the recently released Geographic Classification for Health (GCH) developed by a team at the University of Otago14. The GCH uses a combination of driving access to urban areas alongside population size and density to classify areas in New Zealand. Other rurality definitions exist for New Zealand, which have been developed for purposes such as measuring relative rurality for health research15 and measuring rurality using urban accessibility, based on the Stats NZ UREP 20064,16.
Rural admission pathways
The development of a rural strategy at Waipapa Taumata Rau | The University of Auckland (hereafter the University of Auckland) highlighted the importance of having a social mission and developing rural pathways into medical programs. Issues were identified in the strategy in the rural pathway used at the university such as a poorly defined rural admission pathway17. Both the University of Otago and the University of Auckland use rural admission pathways to increase the rural and, in the case of the University of Auckland, regional medical workforces. While there are no studies investigating the ‘best’ definition of rurality for rural pathways for professional health programs in New Zealand, numerous studies are investigating the relationship between rural background and the outcome career location for medical students, some of which consider the effect of different rural definitions on this relationship18-20. This can range from acknowledging the effect of the definition of rurality18 to exploring the association between different rurality definitions and career locations19. One study found that while all rurality definitions had a relationship with intention to work rurally, those definitions that were too restrictive had a reduced number of eligible students19. Similar studies have been conducted investigating the location graduate medical students work in for medical programs in Australia21,22. These studies show a strong relationship between rural origin and an eventual rural work location.
At the time of starting this study the rural pathway, or admission scheme, for rural students to professional health programs at the University of Auckland was a Regional Rural Admission Scheme (RRAS). The RRAS defined urban students as school-leavers from within the territorial local authority boundaries of Auckland, Hamilton, Tauranga, Wellington, Porirua, Upper Hutt, Hutt, Christchurch and Dunedin city councils; and rural students as school-leavers from within all other territorial authorities. Students qualified for the scheme based on attending a school in the regional/rural area, either 5 years in a qualifying primary school or 4 years in a qualifying secondary school. Approximately 50 places were set aside for RRAS out of a class of 250 at the time of starting this study. A recent review of admission of medical students suggested that the RRAS was not providing equitable opportunities for students from a rural background as originally intended23. The definition of ‘rural’ and ‘urban’ used by the RRAS means that students from regional cities are eligible to apply for the RRAS under the ‘rural’ definition, potentially crowding out students from rural backgrounds. The use of territorial authority boundaries also means that students from rural areas of city councils are ineligible to apply for the RRAS.
Therefore, the definition used in the RRAS should aim to include as many students as possible who self-identify as having a regional or rural origin, as these students may be more likely to have an intention to work regionally or rurally. However, the definition should be updated to prioritise students with a rural origin, addressing the regional advantage of the existing RRAS. This article, therefore, aims to create a more genuine regional rural admission scheme for the University of Auckland that may more strongly contribute to developing a regional and rural workforce.
Methods
Data
A de-identified applicant dataset for those enrolled in the medical program (MBChB) at the University of Auckland from 2017 to 2023 was provided from the University of Auckland (n=1984). The dataset included both domestic and international applicants, but only students with an Aotearoa New Zealand Schools address were included in the analysis (n=1808). Students' school addresses were geocoded using Google API and the location was matched to the candidate definitions. Additionally, data at the Statistical Area 1 (SA1) level from the New Zealand 2018 Census, for those aged 15–29 years and those aged 15–29 years of Māori ethnicity (grouped total response) were used to compare the distribution of classification24.
A methodological framework was developed for determining the most suitable candidate definitions of rurality in New Zealand for updating the RRAS (Fig1).
The methodological framework comprises two sections, the first being an extensive literature review identifying candidate rural definitions, and the second an evaluation of those candidate definitions. From these definitions, an initial selection was made based on a set of criteria, where selected definitions use a combination of these criteria.
These criteria are:
- population size/density, where an area is considered rural as it has a smaller number of people per area unit, or has lower concentration of residential buildings
- geography/distance, where an area is considered more rural as distance increases from more developed or built-up urban areas
- urban accessibility, where areas with less access to urban services, such as health services, are considered more rural
- commuting patterns of resident population, where areas are considered rural if the majority of the resident population does not commute to urban areas for work.
Candidate definitions that used a combination of these criteria were most suitable for the purposes of this article and were selected for further consideration. From the selected definitions, further refinement was made based on a second set of criteria required for the RRAS. Most definitions had multiple categories for ‘urban’ and ‘rural’, so variations were explored to create a two-group urban–rural classification, or a three-group urban–regional–rural classification, and were named ‘modified’ for comparison with the original definitions. In the second phase of the analysis (Fig1) we explored the geographic distribution of each candidate definition using GIS software and undertook data analyses using the anonymised student dataset.
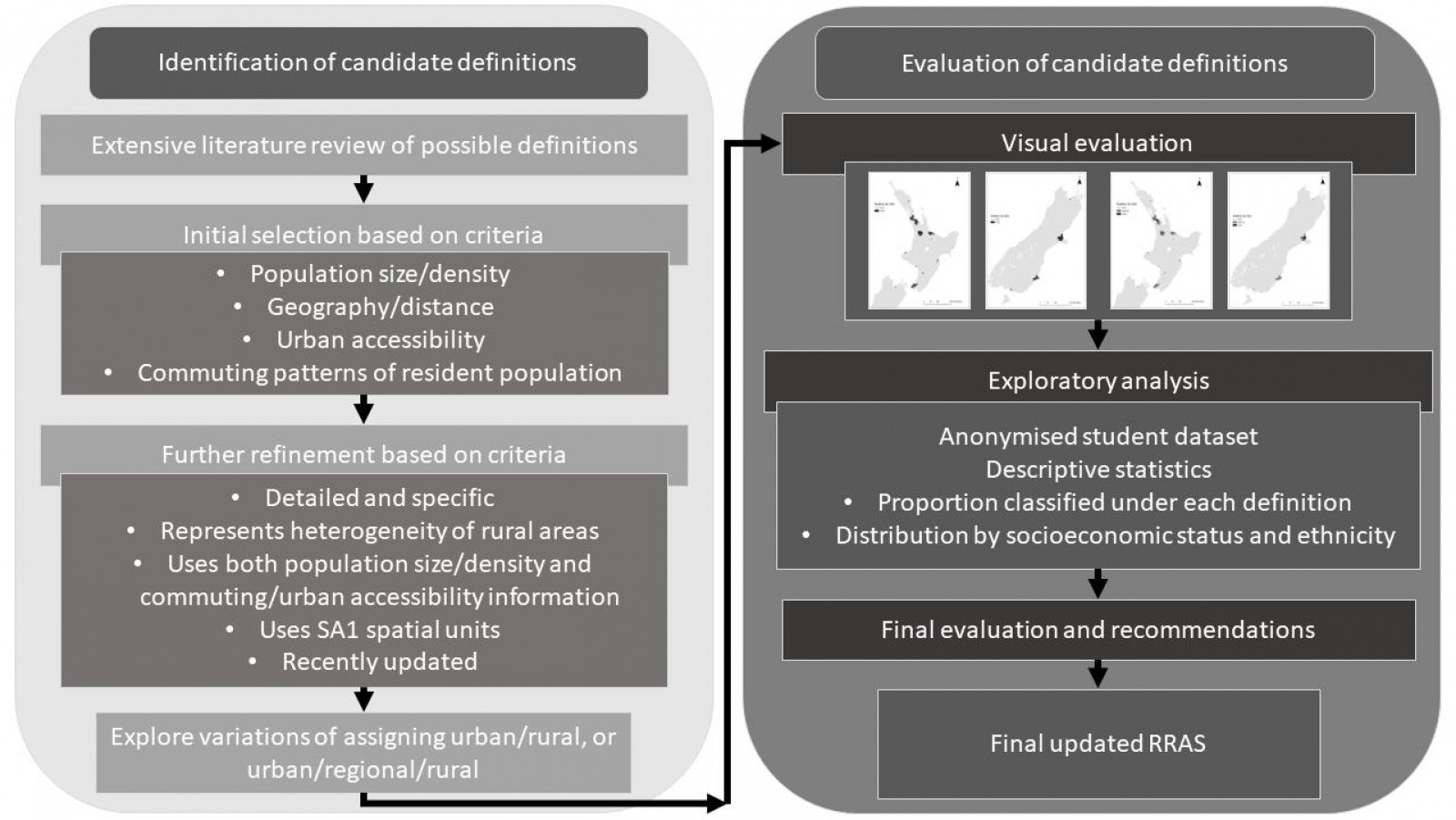 Figure 1: Methodological framework for determining the most suitable candidate ‘rural’ definitions, and evaluating these for recommendation to update the Regional and Rural Admission Scheme ‘rural’ definition at the University of Auckland, New Zealand. RRAS, Regional and Rural Admission Scheme. SA1, Statistical Area 1.
Figure 1: Methodological framework for determining the most suitable candidate ‘rural’ definitions, and evaluating these for recommendation to update the Regional and Rural Admission Scheme ‘rural’ definition at the University of Auckland, New Zealand. RRAS, Regional and Rural Admission Scheme. SA1, Statistical Area 1.
Exploratory analysis
A de-identified student cohort dataset of applicants enrolled for the MBChB from the University of Auckland covering 7 years was used to calculate descriptive statistics and summaries for the proposed options and variables of interest. This provided a realistic estimate of the distribution of students under the proposed options.
The count and proportion of students by the existing RRAS and the modified versions of the candidate definitions ethnicity, year of admission and sex were calculated. Summary tables were produced of students by area deprivation quintile and region. Proportions were calculated for students enrolled in the MBChB who would be considered rural, regional or urban by the modified versions of the candidate definitions. Breakdowns by regions and for those students of Māori ethnicity were also calculated.
We used the 2018 Index of Multiple Deprivation25 to assess the distribution of students classified as rural by area deprivation status.
For each proposed definition of ‘rural’, we calculated the proportion of students classified as rural, subset by level of deprivation using Index of Multiple Deprivation quintiles in which quintile 1 represented the least deprived 20% of areas in New Zealand and quintile 5 identified the most deprived 20% of areas nationally.
Ethics approval
Ethics approval was granted for this project through the University of Auckland Human Participants Ethics Committee (UAHPEC25706). Students gave consent for their enrolment details and demographic information to be used in research on enrolment into the medical program.
Results
Identification of candidate definitions
After an extensive review of the literature and existing rurality definitions used in New Zealand over the past 20 years, five rurality definitions were chosen for initial consideration based on the combination criteria (Table 1). These definitions were sourced from both official Stats NZ classifications, definitions based on one of the Stats NZ classifications, or from a non-Stats NZ source. Of these five candidate definitions, three were selected based on the second set of criteria (Table 1). These three definitions are the most recent, detailed and specific for rural areas. Existing definitions used for rural pathways into professional health programs at other New Zealand institutions were included. While all these three rurality definitions were more comprehensive than the current RRAS definition of rurality, some of these three chosen candidate definitions better represented the heterogeneity of rural areas than others. For these three candidate definitions, the methodology and purpose of each definition was analysed, using the established set of criteria. The similarities and differences between each candidate definition were compared (Table 2), as well as the potential suitability for the RRAS.
The three candidate definitions use a finer resolution of geographic scale of units than the current RRAS rurality definitions and use at least two or more criteria in classifying areas as urban or rural (Table 2). All definitions have been released within the past 2 years and use the latest geographic scale of units/area geography, the SA1 2018.
Modified versions of the three definitions, if applicable, were considered, where multiple urban–rural categories were given a two- or three-group classification that could be suitable for a rural definition for the RRAS. For brevity, the final modified versions of the candidate definitions are shown in Table 3, with the aggregation of categories described. A three-group (urban–regional–rural) classification is produced alongside a two-group (urban–rural) classification due to feedback from medical program leads, who did not want regional students to be ‘lost’ in a binary definition.
Table 1: Initial candidate definitions selected for consideration, and further refined based on criteria from the methodological framework†
| Candidate definition | Source |
|---|---|
| Geographic Classification for Health – GCH | University of Otago, 2021/202214 |
| Statistical Standard for Geographic Areas (SSGA2018) Urban Rural 2018 classification – UR 2018 | Stats NZ, 20188 |
| Urban accessibility classification – UA 2020 | Stats NZ, 202011 |
| Functional urban areas classification – FUA 2021 | Stats NZ, 202112 |
| Urban Rural Experimental Profile – UREP 2006¶ | Stats NZ, 200613 |
† Definition chosen based on the second set of criteria.
¶ Also used for the University of Otago rural pathway, the New Zealand Rural Origins subcategory.
Table 2: Comparisons of similarities and differences between the current Regional and Rural Admission Scheme at the University of Auckland and candidate rurality definitions, after second selection†
| Candidate definition | Population size/density | Geographic scale of units | Commuting patterns and urban accessibility | Temporality of dataset | Classification of areas |
|---|---|---|---|---|---|
| Current RRAS | N/A | Territorial Authority. Regional scale. | N/A | Territorial Authority boundaries updated as required by Stats NZ. | Urban, Rural. Rural: those areas outside the boundaries of Auckland, Hamilton, Tauranga, Porirua, Upper Hutt, Hutt, Wellington, Christchurch, Dunedin Territorial Authority boundaries. |
| GCH | Based on UR 2018. U1 class Major Urban area, U2 class Large Urban category. Uses population size, density. | SA1 2018 units. Neighbourhood scale. | Drive time from location to urban area, drive time to the edge of an urban area. 25 min, 60 min, 90 min thresholds. | Released 2021. Uses 2018 Census data. | U1, U2, R1, R2, R3. |
| UR 2018 | Rural settlement 200–1000 population, ≥40 residential dwellings. Urban areas ≥1000 population, high population density, high coverage built structures. Classifies urban areas by population size. | SA1 2018 units. Neighbourhood scale. | N/A | Released 2018. Uses 2018 Census data. | Major, Large, Medium and Small urban areas, Rural settlements, Rural other. |
| UA 2020 | Major, large and medium urban areas based on UR 2018. | Based on SA1 2018 units. Regional scale. | Potential urban accessibility, estimated drive times to closest urban area. Rural and small urban areas classified by drive to major, large and/or medium urban area(s). | Released 2020. Uses 2018 Census data. | Major, Large, Medium and Small urban areas, High/Medium/Low urban accessibility, Remote, Very Remote. |
| FUA 2021 | Activity space of population, classifies FUA types and FUA components by population size. Areas included in the FUA have >5000 people, or have ≥40% of workers commute to an urban area. | Based on SA1 2018 units. Regional scale. | Actual urban accessibility and commuting, actual commuting information to closest urban area. Workplace address and usual residence address of population. | Released 2021. Uses 2018 Census data. |
FUA components: Urban core, Secondary urban core(s), Satellite urban core(s), Hinterland. FUA types classified by population size: Metropolitan area, Large/Medium/Small regional centre. All other areas: area outside FUA. |
† Although the UR 2018 definition is not included in the final candidate definitions, it is included here for reference as other candidate definitions are based on it.
FUA, functional urban areas. GCH, Geographic Classification for Health. N/A, not applicable. R, rural. SA1, Statistical Area 1. U, urban. UA, urban accessibility. UR, urban rural.
Table 3: Descriptions of final modified candidate definitions, for two-group (urban–rural) and three-group (urban–regional–rural) versions
| Candidate definition | Urban–rural | Urban–regional–rural | |||
|---|---|---|---|---|---|
| Urban categories | Rural categories | Urban categories | Regional categories | Rural categories | |
| Modified GCH | U1, U2 | R1, R2, R3 | U1 | U2 | R1, R2, R3 |
| Modified UA 2020 |
Major urban area, Large urban area High urban accessibility |
Medium urban area Medium urban accessibility, Low urban accessibility Remote, Very remote |
Major urban area |
Large urban area High urban accessibility |
Medium urban area Medium urban accessibility, Low urban accessibility Remote, Very remote |
| Modified FUA 2021 | Metropolitan area (all), Large and Medium regional centres (urban core) |
Hinterland and other urban areas of Large and Medium regional centres All of Small regional centres Areas outside FUA |
N/A | N/A | N/A |
FUA, functional urban areas. GCH, Geographic Classification for Health. N/A, not applicable. R, rural. U, urban. UA, urban accessibility.
Evaluation of candidate definitions
In the second section of the methodological framework, the modified candidate definitions are evaluated using visualisation (that is, mapping). The three candidate definitions were mapped for all of New Zealand and for key locations of interest to compare similarities and differences in the geographic distribution of urban–rural and urban–regional–rural for the modified definitions (Figs 2 and 3, respectively).
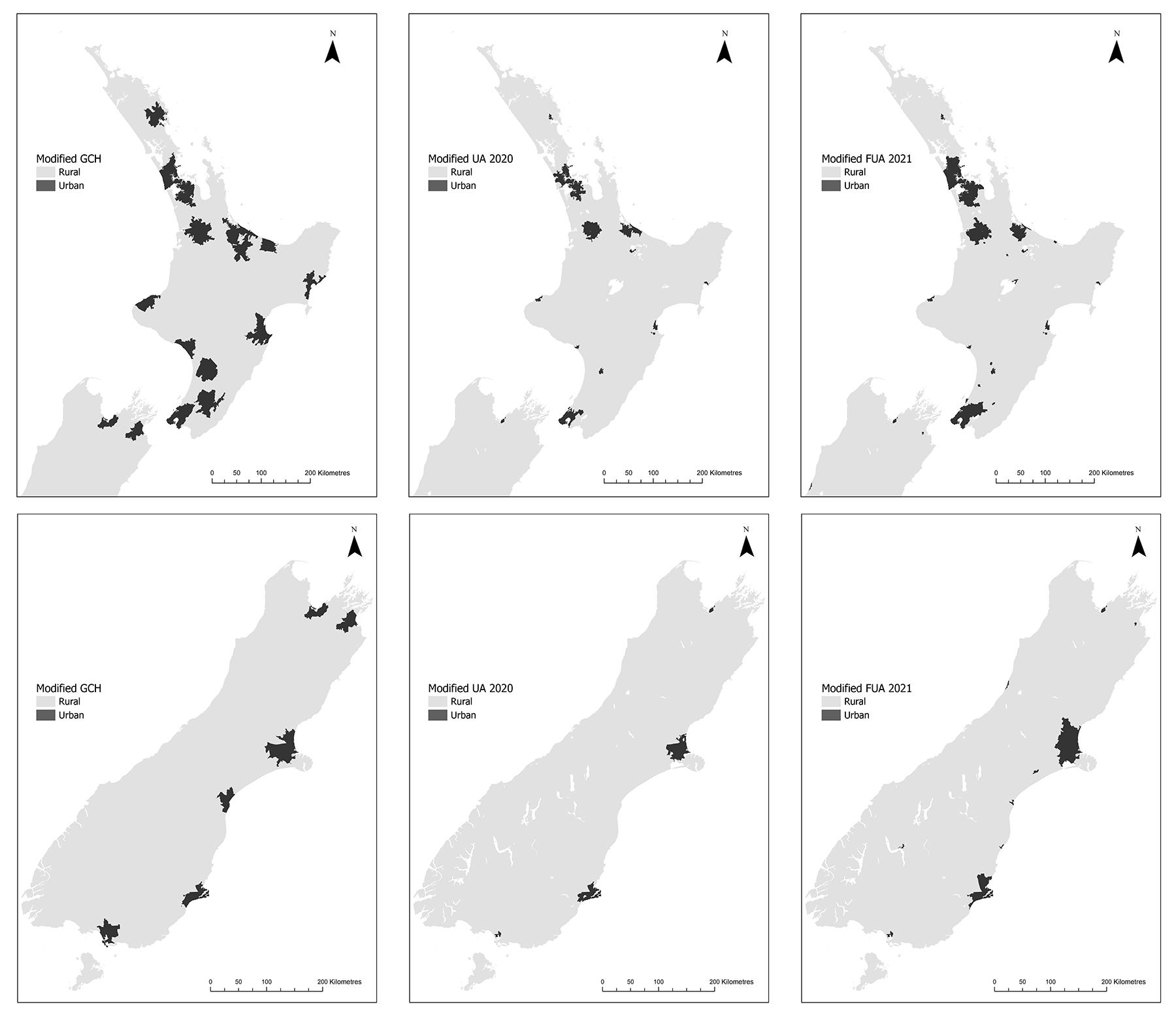 Figure 2: Maps of the two main islands of New Zealand (North Island above; South Island below) showing urban–rural classification for the three modified candidate definitions. Left to right: GCH, UA 2020, FUA 2021. The Chatham Islands are excluded from these maps, but are classified as rural under all definitions. FUA, functional urban areas. GCH, Geographic Classification for Health. UA, urban accessibility.
Figure 2: Maps of the two main islands of New Zealand (North Island above; South Island below) showing urban–rural classification for the three modified candidate definitions. Left to right: GCH, UA 2020, FUA 2021. The Chatham Islands are excluded from these maps, but are classified as rural under all definitions. FUA, functional urban areas. GCH, Geographic Classification for Health. UA, urban accessibility.
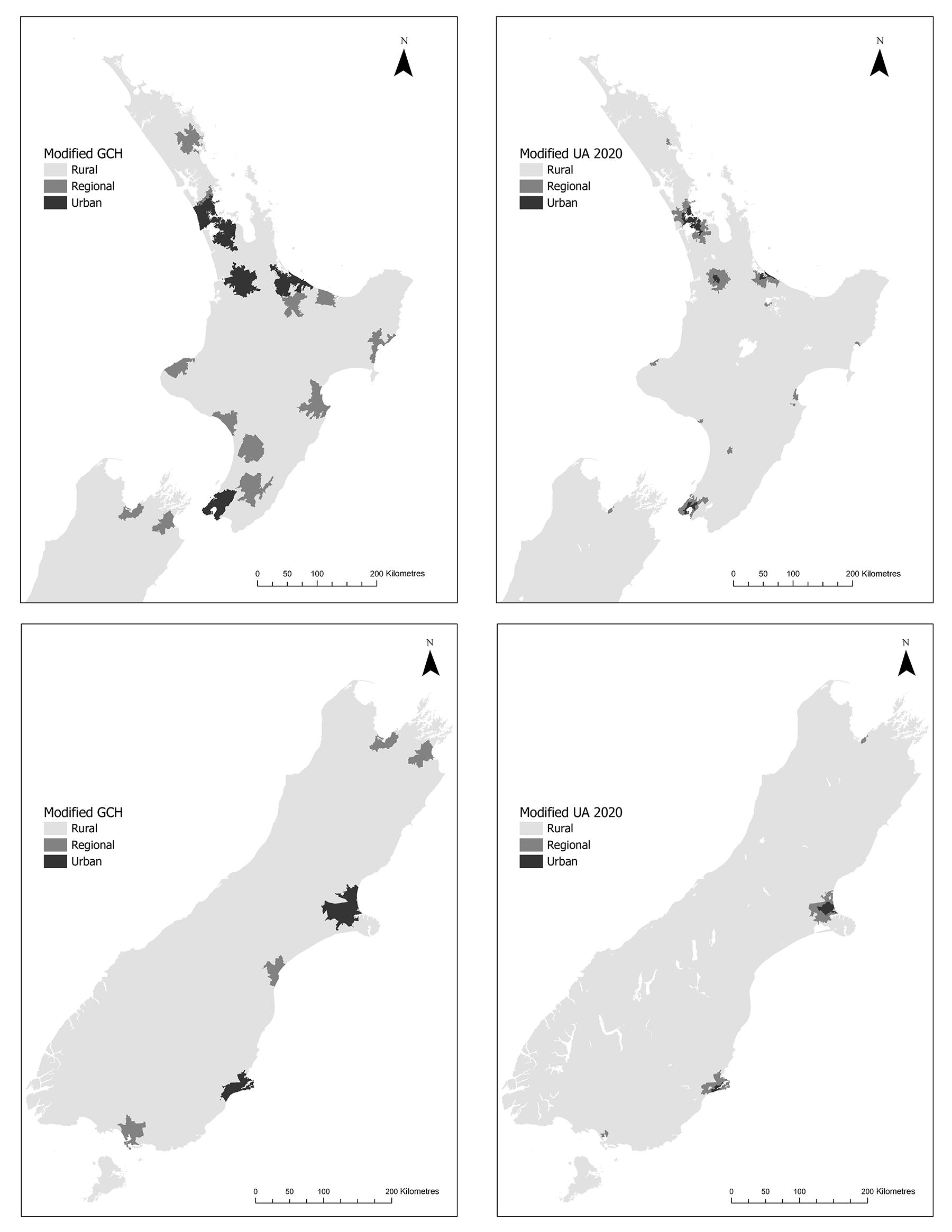 Figure 3: Maps of the two main islands of New Zealand (North Island above; South Island below) showing the urban–regional–rural classification for the two modified candidate definitions. Left to right: GCH, UA 2020. The Chatham Islands are excluded from these maps, but are classified as rural under all definitions. GCH, Geographic Classification for Health. UA, urban accessibility.
Figure 3: Maps of the two main islands of New Zealand (North Island above; South Island below) showing the urban–regional–rural classification for the two modified candidate definitions. Left to right: GCH, UA 2020. The Chatham Islands are excluded from these maps, but are classified as rural under all definitions. GCH, Geographic Classification for Health. UA, urban accessibility.
To compare the modified candidate definitions, case study locations were selected throughout New Zealand (Fig4). Under the current RRAS, Whangārei is classified as rural despite being the largest town in the Northland region, Warkworth is classified as urban despite being a small settlement surrounded by rural locations, and Cambridge and Rangiora are classified as rural, despite having high urban accessibility. An ideal updated RRAS would classify these locations with higher accuracy than currently exists.
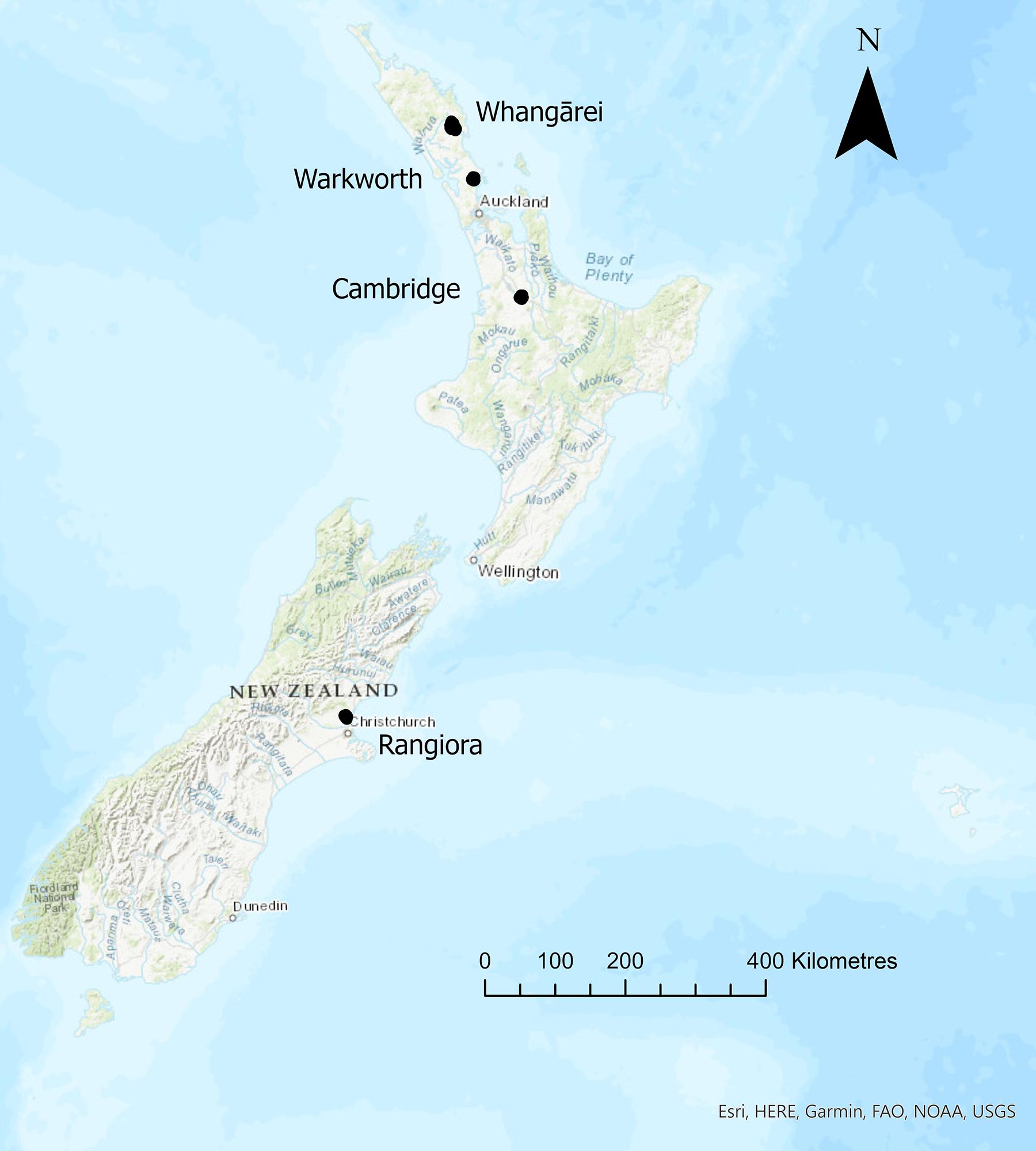 Figure 4: Case study locations for comparing modified candidate definitions.
Figure 4: Case study locations for comparing modified candidate definitions.
The binary modified GCH and FUA 2021 definitions appear to classify a larger land area as urban than the modified UA 2020 (Fig2). In the North Island, the case study location of Whangārei is classified as urban in all three definitions, with a larger surrounding urban area under the modified GCH. Warkworth is classified as rural under the modified UA 2020 and modified FUA 2021, but is classified as urban under the modified GCH. Cambridge is classified as urban under the modified GCH and modified FUA 2021, but is classified as rural under the modified UA 2020. In the South Island, Rangiora is classified as urban under the modified GCH and the modified FUA 2021, but is classified as rural under the modified UA 2020.
Given the same core locations are classified as urban under the modified UA 2020 as the modified FUA 2021, but the modified UA 2020 has a larger land area overall in New Zealand classified as rural, the FUA 2021 was not considered for recommendation. This decision was supported by stakeholder feedback, which agreed that the modified versions of the GCH and UA 2020 definitions were more suitable than those of the FUA 2021. Therefore, a three-group version of the modified FUA 2021 was not produced. An interactive web app visualising the existing RRAS and the three-group modified versions of the GCH and UA 2020 definitions is available at https://uoa.maps.arcgis.com/apps/webappviewer/index.html?id=37eadd5dcf974b25ba8a384662c3774c.
Similar to the two-group versions, the three-group modified GCH appears to classify more land as urban or regional compared to the modified UA 2020. In comparison to the two-group versions, many of the areas classified as urban under the modified GCH are now classified as regional under the regional version. In particular, the case study locations of Whangārei and Warkworth are now classified as regional. This is suitable for the purposes of the RRAS. Similarly, the regional version of the modified UA 2020 classifies Whangārei as regional where it was previously urban. Across New Zealand, the core centres of urban cities and towns remain as urban, but the surrounding areas are regional, as well as many smaller cities. In the South Island, much of the land area is classified as rural under both three-group regional definitions, and the only urban areas are Christchurch and Dunedin (the whole city under the modified GCH, and only the urban core in the modified UA 2020). The case study location of Rangiora is classified as urban under the three-group modified GCH and rural under the three-group modified UA 2020.
Considering that the current RRAS does not distinguish between regional and rural populations, the modified UA has a combined larger percentage of students with an Aotearoa New Zealand Schools address who were enrolled in the MBChB classified as regional or rural than the current RRAS, while the GCH has a smaller percentage (Table 4). A larger percentage of students who were enrolled in the MBChB are classified as urban compared to the expected population of those aged 15–29 years in the New Zealand 2018 Census (Table 4), regardless of the classification definition used. The percentage of students enrolled in the MBChB classified as rural is much lower than the expected population of those aged 15–29 years in the New Zealand 2018 Census, regardless of the classification definition used.
While Table 4 includes students of Māori and Pacific ethnicity, Māori and Pacific students typically apply for professional health programs at the University of Auckland through the Māori and Pacific Admission Scheme. We also classified those students who were enrolled in the MBChB and of Māori descent.
Again, the modified UA 2020 classifies a higher proportion of Māori students who were enrolled in the MBChB program as rural than both the modified GCH and the current RRAS. A larger percentage of Māori students who were enrolled in the MBChB program were classified as urban compared to the expected population of those aged 15–29 years of Māori ethnicity in the New Zealand 2018 Census (Table 5).
The percentage of the expected population of Māori ethnicity classified as living in regional or rural areas is higher than the percentage of the expected population of any ethnicity. The same difference exists for the students enrolled in the MBChB program; however, the difference is less pronounced than for the expected population.
Regardless of the classification, there is a higher proportion of students classified as regional or rural in the more deprived quintiles. However, the modified UA 2020 classifies a higher proportion of students as regional in the more deprived quintiles. The modified UA 2020 has a more even distribution of proportions across the Index of Multiple Deprivation quintiles for the rural classification, compared to the modified GCH.
Table 4: Classification of the expected population of those aged 15–29 years in the 2018 New Zealand Census (Statistical Area 1), and students with an Aotearoa New Zealand Schools address enrolled in the University of Auckland MBChB†
| Classification |
Expected population¶ of those aged 15–29 years, in New Zealand 2018 Census (n=820,170) n (%) |
All students, Aotearoa New Zealand Schools address, enrolled in MBChB (n=1808) n (%) |
||||
|---|---|---|---|---|---|---|
| Urban | Regional | Rural | Urban | Regional | Rural | |
| Current RRAS | 543,885 (66.31) | 276,285 (33.69) | 1388 (76.8) | 420 (23.2) | ||
| Modified GCH | 574,257 (70.02) | 128,274 (15.64) | 117,651 (14.34) | 1429 (79.0) | 292 (16.2) | 87 (4.8) |
| Modified UA | 490,227 (59.77) | 135,564 (16.53) | 194,376 (23.70) | 1363 (75.4) | 251 (13.9) | 194 (10.7) |
† Using enrolment through the current Regional and Rural Admission Scheme and the modified versions of the candidate definitions for updating the scheme.
¶ Counts for the expected population were obtained from the 2018 Census tables from the Integrated Data Infrastructure. Cell counts may not add exactly up to the total count due to random rounding methods applied for data confidentiality purposes.
GCH, Geographic Classification for Health. RRAS, Regional and Rural Admission Scheme. UA, urban accessibility.
Table 5: Classification of expected population of those aged 15–29 years of Māori ethnicity in the New Zealand Census 2018 (Statistical Area 1 level), and Māori students with an Aotearoa New Zealand Schools address enrolled in the University of Auckland MBChB †
| Classification |
Expected population¶ of those aged 15–29 years of Māori ethnicity in the New Zealand Census (n=65,913) n (%) |
All Māori students, Aotearoa New Zealand Schools address, enrolled in MBChB (n=286) n (%) |
||||
|---|---|---|---|---|---|---|
| Urban | Regional | Rural | Urban | Regional | Rural | |
| Current RRAS | 30,483 (46.2) | 35,430 (53.8) | 188 (65.7) | 98 (34.3) | ||
| Modified GCH | 33,339 (50.6) | 17,439 (26.5) | 15,135 (23.0) | 193 (67.5) | 64 (22.4) | 29 (10.1) |
| Modified UA | 27,279 (41.4) | 16,476 (25.0) | 22,164 (33.6) | 182 (63.6) | 51 (17.8) | 53 (18.5) |
† Using enrolment through the current Regional and Rural Admission Scheme and the modified versions of the candidate definitions for updating the scheme.
¶ Counts for the expected population were obtained from the 2018 Census tables from the Integrated Data Infrastructure. Cell counts may not add exactly up to the total count due to random rounding methods applied for data confidentiality purposes.
GCH, Geographic Classification for Health. RRAS, Regional and Rural Admission Scheme. UA, urban accessibility.
Table 6: Classification of all students with an Aotearoa New Zealand Schools address enrolled in the University of Auckland MBChB†, broken down by the New Zealand Index of Multiple Deprivation 2018 quintile
| Classification by IMD quintile rank | Urban¶ n (%) | Regional¶ n (%) | Rural¶ n (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |
| Current RRAS | 242 (17.4) | 453 (32.6) | 215 (15.5) | 326 (23.5) | 152 (11.0) | N/A | N/A | N/A | N/A | N/A | 46 (11.0) | 57 (13.6) | 52 (12.4) | 170 (40.5) | 95 (22.6) |
| Modified GCH | 244 (17.1) | 458 (32.1) | 215 (15.0) | 359 (25.1) | 153 (10.7) | 35 (12.0) | 44 (15.1) | 48 (16.4) | 88 (30.1) | 77 (26.4) | 9 (10.3) | 8 (9.2) | 4 (4.6) | 49 (56.3) | 17 (19.5) |
| Modified UA | 235 (17.2) | 443 (32.5) | 211 (15.5) | 324 (23.8) | 150 (11.0) | 18 (7.2) | 45 (17.9) | 34 (13.5) | 87 (34.7) | 67 (26.7) | 35 (18.0) | 22 (11.3) | 22 (11.3) | 85 (43.8) | 30 (15.5) |
† Using enrolment through the current Regional and Rural Admission Scheme and the modified versions of the candidate definitions for updating the scheme.
¶ 1 = least deprived, 5 = most deprived.
GCH, Geographic Classification for Health. IMD, Index of Multiple Deprivation. N/A, not applicable. RRAS, Regional and Rural Admission Scheme. UA, urban accessibility.
Discussion
This study used a two-stage methodological framework to identify and evaluate candidate rural definitions for updating the RRAS for the University of Auckland, aiming to create a more genuine admission scheme that may increase the rural and regional workforce.
The modified UA 2020 definition consistently classified a higher proportion of students as regional and rural compared to the current RRAS and the alternative proposed definition for the modified GCH. In addition, it classified a higher number of Māori students and those living in less-deprived neighbourhoods as rural than when using the other definitions. The modified UA 2020 definition also correctly classifies the case study locations as expected.
Recommendations
After reviewing the results of the visualisation and exploratory analysis, and feedback from the medical program leads, the three-group modified UA 2020 was selected as the recommended option to update the rural definition of the RRAS. The modified UA definition meets the criteria established in the first phase of the research, and because it was developed by Stats NZ the UA classification is to be updated regularly. Moreover, the modified UA 2020 classification is independent of access to healthcare definitions (ie GCH14), which may not be relevant in an education setting and captures the most students who would identify as being of rural origin. The modified UA 2020 will assist in addressing the under-representation of rural students admitted to professional health programs at the University of Auckland, while not disadvantaging regional students. This recommendation was accepted by the medical program at the University of Auckland. Twenty-three percent of the class intake is set aside for RRAS and the qualifying period of time for schooling was set at 8 years for primary schooling or 3 years for secondary schooling. A position of Associate Dean Rural Health was created, whose role includes annual monitoring of RRAS. Monitoring strategies include calculation of rural student percentages and distribution of origin of rural students.
Comparison to previous work
While there is little literature on choosing a suitable rural definition for a rural pathway for entry into professional health programs at tertiary institutions in New Zealand, some studies have explored the best way to choose a rural definition for research or policy19,26. There are also a number of studies exploring the relationship between the rural background of students and their intentions to work in rural locations.
One study in New Zealand used the RRAS alongside other constructed rurality definitions to assess whether the relationship between rural background of medical students and intention to work in a rural location varied depending on the rural definition used19. Poole et al found students classified as rural using those definitions that were more detailed and specific had a higher likelihood of intending to work in a rural location post-study19. This supports our findings here, where those rural definitions we considered for evaluation were those that were more detailed and specific. A limitation of Poole et al’s study was that the rural definitions used were all based on either simplistic definitions using only population size, or were based on an outdated Stats NZ urban–rural classification19. None of the definitions used by Poole et al would have been considered suitable using our methodological framework19. Future work could include replicating an analysis similar to that of Poole et al19, but using the candidate definitions presented here.
The methodological framework used in this study was based on two sets of criteria, which represented the most relevant elements of a rural definition to support rural professional health education pathways. Definitions chosen for consideration had to meet both sets of criteria, which included that the definitions are regularly updated and that the data are current and therefore available. This criteria choice is supported by other studies that discussed how best to choose rural definitions for applications such as health policy27, emphasising that the availability of data, and therefore the currency of the definition, is critical when choosing a rural definition.
Hart et al concluded that while there is never a perfect rural definition for all purposes, a suitable definition can be found for a specific purpose6. Similar to Coburn et al27, Hart et al6 emphasised that a suitable definition should be able to be replicated, be derived from current, high-quality data, and be checked for correctness against on-the-ground classification. In the present study, only those candidate definitions that met a specific criteria were considered for evaluation. Those criteria included these points made by Hart et al6, alongside other relevant criteria suited to the purpose of the definition. The validity of the classifications were checked using case study locations where ideal urban–rural classifications were known.
One limitation of the RRAS scheme and other similar schemes is that, regardless of the rural definition used, boundaries are still required to be chosen and areas delineated spatially in two-group (urban–rural) or three-group (urban–regional–rural) classifications. Future work could include exploring the possibility of using a rural index or continuous definition of rural (eg that of Zhao et al15), where a student’s ‘rurality’ is measured as a factor where the more ‘rural’ a student is, the more priority a student is given for admission to professional health programs. This is a concept that has been suggested in the literature (eg Matsumoto et al28, Bennett et al7), but to our knowledge not yet implemented.
Another consideration raised by Poole et al is that some students classified as rural using the RRAS definition will not see themselves as being rural, and therefore may not intend to move into working in a rural location post-study19. This highlights the importance of a rural definition that uses a combination of criteria to define rural origin as well as rural workforce intention. Examples used in other medical schools to capture rural workforce intention include volunteering in rural areas, previous rural employment, stated interest in primary care, commitment to working in underserved areas and altruistic beliefs29.
Wendling et al also raised the importance of capturing those students who define themselves as being from a rural background, suggesting that admission schemes to professional health programs could consider self-identification of rural background in entry requirements30. This was based on their findings that those who identify as being from a rural background are more likely to work in a rural location. While self-identification of rural background may not be possible to include in professional health program admission in New Zealand at this time, this is something that could be considered for further work and implementation.
Ideally, those students who gain entry to a professional health program through a rural pathway are both from a rural background and intend to work in a rural location after graduation. This would assist in developing the rural health workforce of New Zealand, and students who enter through this pathway could be provided with additional training for working in a rural setting.
In the context of the results presented in this study, Wendling et al’s findings30 support our criteria that a definition of rurality should be as specific and accurate as possible – a suitable definition should capture the population who consider themselves to be rural as well as those who are geographically remote.
While the modified UA 2020 selected for the RRAS is likely to capture the majority of students who self-identify as being rural, it has not been designed to account for educational disadvantage potentially experienced by rural students. Recent work demonstrates that the modified UA 2020 does highlight educational disadvantage in rural areas31.
Conclusion
This article aimed to create a more genuine rural admission scheme for the University of Auckland that may more strongly contribute to developing a rural workforce. A methodological framework was developed for determining the most suitable candidate definitions of rurality in New Zealand for updating the RRAS. The final definition recommended was the modified UA 2020, which included an additional regional category to facilitate access for regional students to professional health programs at the University of Auckland. The final definition, when implemented in a future version of the RRAS, will assist in addressing the under-representation of rural students admitted to professional health programs at the University of Auckland – which in the long term will supplement the professional rural medical workforce.
Funding
This work was not supported by any funding.
Conflicts of interest
The authors report there are no competing interest to declare.
AI disclosure statement
No generative AI or AI-assisted technologies were used in this research or in the preparation of this manuscript.
Disclaimer
These results are not official statistics. They have been created for research purposes from the Integrated Data Infrastructure Database (Longitudinal Business Database) (https://www.stats.govt.nz/integrated-data), which is carefully managed by Stats NZ.
Access to the data used in this study was provided by Stats NZ under conditions designed to give effect to the security and confidentiality provisions of the New Zealand Data and Statistics Act 2022. The results presented in this study are the work of the author, not Stats NZ or individual data suppliers.