



Introduction
Policymakers are under growing pressure to implement effective healthcare delivery models that enhance access to health services, especially in rural areas1. Innovative models are being adopted worldwide to enhance access to essential health services in rural areas2,3. Nevertheless, implementing these models can prove challenging, particularly in low-resource countries. This difficulty arises from various factors, such as insufficient funding, underdeveloped infrastructure, and a lack of leadership and skilled labour. Furthermore, government instability and corruption within the healthcare system can impede the successful implementation of policy2,4. These systemic problems remain significant obstacles to attaining universal health coverage worldwide3. This scenario could make vulnerable groups more prone to increased infection rates as well as preventable disabilities and deaths, underscoring the critical necessity for effective healthcare delivery models3,5,6. This problem partly stems from the inadequate implementation of the healthcare policy framework7. Therefore, it is crucial to investigate the perspectives of health workers, communities and policymakers to fully understand the challenges in implementing healthcare policy to improve rural health services.
In Papua New Guinea (PNG), health services are provided by the government and churches, with the majority of funding coming from the state. Nevertheless, the funding processes tend to be fragmented and insufficient. Although the public sector provides primary health care (PHC) services at no cost, health funding has been insufficient since 2010, leading to considerable challenges in access8,9. Health policy planning and implementation in PNG follow a 10-year cycle; currently, the National Health Plan 2021–2030 is supported by Corporate Plans (2022–2026) and Provincial Health Authorities (PHAs). Health services operate under a decentralised model managed by PHAs. This approach was implemented to enhance healthcare access in rural and remote regions within a cohesive board system9. PNG’s strategic plan for the health sector highlights the government’s dedication to enhancing rural health services, emphasising equity in health care.
The PHA policy was introduced in PNG in the early 2000s as part of broader health system reform aimed at strengthening the effectiveness, efficiency and accountability of health services provision. It was officially launched in 2007 and serves as a crucial foundation for the government’s aim of creating a healthy, wealthy and prosperous society by 205010. PHA policy has been implemented at the subnational levels such as the provincial and district healthcare system. The PHA outlines the roles of national and subnational entities, as well as key stakeholders responsible for implementing this policy framework and delivering health services to PNG’s rural population. This framework is in effect across all 22 provinces of PNG, with Madang Province adopting it in 2019. In 2014, a decade later, the national government established the District Development Authority (DDA) policy to enhance local service infrastructure and delivery. The DDAs oversee funding for the District Service Improvement Program and the District Infrastructure Program. Moreover, the DDA was created to eliminate bureaucratic obstacles, provide districts with increased funding and enhance local services for communities11. However, there is limited information about the application of these two policy frameworks and the challenges affecting their implementation in rural districts.
This research utilises public health theory, particularly the socioecological model (SEM), to construct its research questions and goals. It also serves as an analytical framework, offering a comprehensive perspective on the factors that affect policy implementation across various levels of the healthcare system in PNG. Numerous researchers have previously used SEM to evaluate the factors influencing policy, such as the implementation of tuberculosis control programs12, access and utilisation of health services by young people13, the effectiveness of nutritional programs14 and the implementation of diabetes education programs15.
Although PHA and DDA have been introduced in recent years within the PNG health sector, little is known about the socioecological factors shaping their implementation in rural districts of Madang Province. Through qualitative interviews and group discussions with administrators, clinicians and community members, our study provides a unique perspective from those who have experienced the translation of policy into practice and are end users of health services in rural areas. This study argues that the implementation of health policy is influenced by multiple actors at different tiers of the health system. Therefore, understanding these actors and their impact on policy implementation is critical to the effective delivery of health services, particularly in rural areas.
Methods
Study design
An exploratory qualitative study16,17 was conducted among health workers, public servants, and the community in three rural districts in Madang Province: Madang, Sumkar and Bogia. Among the six rural districts in the province, these study sites were purposively selected for their relevance to PHA policy implementation and their capacity to provide context-rich data on how the PHA policy has been implemented in the districts18. Furthermore, these facilities are located in the six rural districts where the PHA policy has been actively implemented, making them appropriate for exploring contextual realities, challenges and outcomes. The exploratory qualitative research was chosen to gain a comprehensive understanding of the factors influencing the implementation of PHA and DDA in rural health facilities across the districts of Madang Province, marking the first study since the roll-out of these policies in PNG10. An exploratory study is a research approach aimed at elucidating how a phenomenon manifests, and it is particularly valuable for revealing the full nature of a poorly understood phenomenon. Hunter et al11 concur, suggesting that a qualitative exploratory design enables researchers to investigate a topic with limited existing literature while encouraging active participation from research participants in developing new knowledge in the study area. Rural districts were selected for this research because policy implementation occurs at the district level, and a significant portion of the PNG population resides in rural and remote districts12,19. This research holds significant importance because it addresses the challenges encountered by numerous healthcare systems operating in highly competitive and volatile environments. Qualitative research is crucial for exploring organisational and administrative challenges11. In collaboration with health workers, public servants and the community, this research employed multiple data collection techniques, including interviews, focus group discussions and field observation notes.
Topic guides
Topic guides were developed for participant and key informant interviews, incorporating insights from SEM theories. The lead investigator drafted the interview topic guides, which included open-ended questions addressing the implementation of PHA and DDA, drawing on SEM insights. Subsequently, the topic guides were presented at the Health Management and Systems Development staff meeting. It is one of the departments within the Faculty of Medicine and Health Services at Divine Word University, Madang campus, where the researchers are employed. The researchers revised the topics accordingly. The revised topic guides were then used in the data collection.
SEM as a theoretical framework
SEM is a public health theory developed from Bronfenbrenner’s ecological systems theory20. It is widely used by researchers in health systems and public health to understand the interactions among multifaceted factors, including governance, organisational capacity, cultural norms and resource limitations, that influence the implementation of health policies, especially in developing countries13. The outcomes of implementing health policies are not determined solely by individual actors, but by different tiers of the healthcare system, community dynamics, policy context and macro sociopolitical environments. The SEM provides a structured method to investigate these multifaceted influences and their relationships (Fig1). This framework serves as the overarching structure for the study, providing practical implications by outlining the context in which the PHA and DDA policy frameworks are implemented in the rural districts of Madang Province, along with the environmental factors that drive their implementation to deliver health services to these communities. The SEM framework demonstrates how broader social and ecological factors, as well as micro-level influences, affect the implementation of PHA and DDA strategies in the province14. It is crucial to understand the policy context and the environmental issues affecting their roll-out to effectively assess the implementation of the PHA and DDA policies. This understanding stems from the interplay between intrapersonal, interpersonal, institutional, community and public policy factors21. These levels of the SEM guided the development of study variables, interview guides, focus group discussions, and data coding and thematic categorisation during the analysis. The rationale for adopting this theory is to provide a solid foundation for further investigation into the determinants of the implementation of the PHA and DDA policies across various levels of the health system in Madang Province. Understanding the contextual factors that shape the implementation of key national health policies in a real-world environment is vital, as the effects of these factors differ across different tiers of the healthcare system22,23.
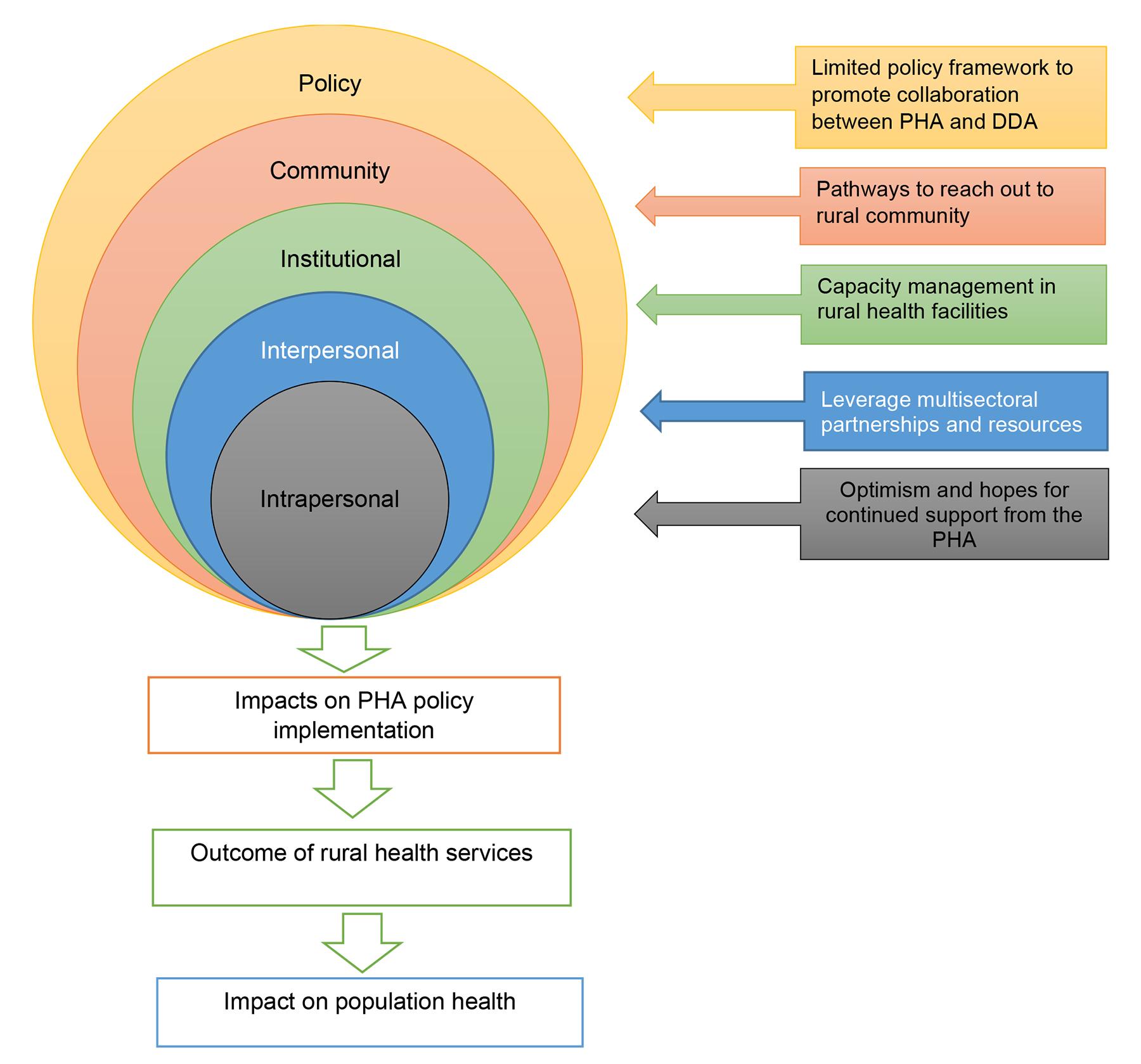 Figure 1: Conceptual framework of the SEM and its impact on PHA policy implementation. DDA, District Development Authority. PHA, Provincial Health Authority.
Figure 1: Conceptual framework of the SEM and its impact on PHA policy implementation. DDA, District Development Authority. PHA, Provincial Health Authority.
Participants
Participants for this study included key informants from rural health facilities, district administrations, and community and policymakers across Madang, Sumkar and Bogia in Madang Province. Participants included doctors, nurses, community health workers, health extension officers, district administrators and provincial health administrators (directors and program managers) aged 18 years or older, employed for more than 2 years in the districts and province, and experienced in implementing the PHA policy. Individuals with less than 2 years of work experience and no experience with PHA policy implementation were excluded from the study. Participants were recruited through convenience sampling, and selected on the basis of their accessibility to the researchers. This sampling technique was employed in this study because of challenges in reaching diverse participants through other means, such as email, given considerations of geographical proximity, availability at specified times, and willingness to engage in the research24. Policymakers were recruited by scheduling workplace appointments and were interviewed at suitable times.
Data collection
The researchers collected data from June 2024 to December 2024. Participants were contacted using the researchers’ contact details. Thirty participants were interviewed through a well-structured, rigorous semistructured interview guide, carefully designed to align with the research objectives and the SEM framework. Data collection continued until data saturation was reached with participant 20; no new ideas or concerns emerged from additional interviews and group discussions25. However, we continued the interviews with available participants to determine whether any new issues arose. We used multiple data collection methods, including focus group discussions to capture collective perspectives and group dynamics regarding PHA policy implementation, and in-depth interviews to provide deeper insights into individual experiences and sensitive issues. The sample sizes for both focus group discussions and in-depth interviews were guided by qualitative research principles and were deemed sufficient once theoretical saturation was achieved and recurring themes emerged across participants. Before the interviews, the researchers explained the purpose of the study and encouraged participants to ask questions during the sessions. The principal investigator and coresearchers conducted all participant interviews. The research team comprised two males and three females, all trained and experienced in mixed-methods and qualitative research in PNG. Each interview lasted 30–60 minutes.
Data collection drew on three primary sources to triangulate the information – semistructured interviews, focus group discussions and field notes – enhancing the credibility of the research. The interview and focus group discussion guides were developed based on the study objectives, research questions and the SEM, and were informed by relevant literature. The tools comprised six sections covering key areas at the sociodemographic, policy, community, interpersonal, institutional and intrapersonal levels, with approximately seven open-ended questions and probes to facilitate deeper examination. The final revised version, refined after pilot testing, was used for data collection. Semistructured interviews and focus group discussions were recorded and transcribed verbatim for each participant. Where interviews were conducted in the local language (Tok Pisin), transcripts were translated into English by all researchers, who are very familiar with both languages. All members of the research team verified the transcription and translation processes, and the principal investigator checked the data for accuracy through cross-examination of selected recordings and transcripts to ensure consistency and quality. Additionally, field notes were taken throughout the interviews and group discussions to summarise key points and capture the information highlighted by participants. Member checking of the synthesised data was conducted by emailing participants a summary of the results to confirm whether they aligned with their views. Table 1 presents the profiles of the study participants.
Table 1: Number of study participants
| Health sector level | Number of participants |
|---|---|
| Public policy | Curative Health Services manager (6) Director of Public Health (1) Director of Curative Health Services (1) Director of Corporate Health Services (1) |
| Community level | Patients (6) |
| Institution level | HIV program manager (2) Officer in charge – health centre (2) Hospital administrator (1) Director of Nursing Service (2) |
| Interpersonal level | 0 |
| Intrapersonal level | Bogia Health Centre staff (3) Malala Health Centre staff (2) Yagaum Rural Hospital staff (3) |
Data analysis
A hybrid deductive–inductive thematic analysis was adopted to analyse the data26. This study utilised predetermined themes and categories from the SEM while incorporating emerging themes from the fieldwork. Interviews and group discussion data were analysed manually. Thematic analysis was employed to identify, analyse, interpret and report themes within the dataset. The researchers followed a systematic approach based on the five steps of thematic analysis as theorised by Clarke and Braun27. First, the transcribed data were read and reread to explore meanings and connections across key themes and to categorise the data according to the SEM framework. Subsequently, the data were compared and discussed as a team. Then, the investigation team convened regularly to review the codes and identify, develop and refine themes until consensus was achieved. Finally, the researchers refined each theme and extracted quotations from the dataset to support each theme.
Credibility, dependability, transferability and confirmability
We maintained credibility through triangulation of data collection methods (focus group discussions, in-depth interviews, field notes), extended engagement with participants, and iterative questioning to verify participants’ responses. Furthermore, the research team met regularly and compared emerging themes to enhance the accuracy and trustworthiness of the explanations and interpretations28.
Dependability was ensured by maintaining a clear record of the research process, including sampling decisions, data collection, coding and analysis stages. This was done to ensure that the process was transparent and to promote transferability of the study to other settings16.
Transferability was maintained by providing in-depth details of the study contexts, respondents and settings, allowing audiences to determine the applicability of the findings to similar contexts16.
Confirmability was supported through reflexive practices, including acknowledging the research team’s positions and using participants’ exact words (verbatim) to support the interpretations. Moreover, the principal investigator reviewed the data independently and discussed them with the research team during a group meeting to ensure that the findings were grounded in the data rather than in the researchers’ assumptions28.
Ethics approval
This research received approval from both the Faculty of Medicine and Health Sciences at Divine Word University, Madang campus (FRC/MHS/51-24) and the Madang Provincial Health Authority Research Committee (MAPHA REC No: 09.24) to conduct assessments in rural health facilities and among healthcare workers in Madang Province. Local protocols and requirements were followed during access to these health facilities. Before the interviews, written informed consent was obtained from the participants. The researchers explained the purpose of the study and obtained consent by having participants sign the consent form, thereby indicating their voluntary agreement to participate. Participation was completely voluntary, participants being free to withdraw from the study at any time without repercussions. They were also informed of their right to decline to answer any questions.
Results
The study participants provided insights into the implementation of the PHA and collaboration with the DDA, as well as the perceived factors influencing the effective implementation of these two significant government policies aimed at sustaining rural health services in PNG. They shared experiences of common factors, including a willingness to help others, optimism and hopes for ongoing support for the PHA (intrapersonal), the limited influence of PHA leadership at the district level, leveraging multisectoral partnerships and resources (interpersonal), capacity management in rural healthcare facilities (institutional), pathways to engage with rural communities (community), a limited policy framework to enhance collaboration between the PHA and DDA, leadership in enforcing and ensuring policy implementation at the macro level, and fragmentation of responsibilities at the subnational level (policy). These perceptions regarding the implementation of the PHA and DDA are presented using the five levels of SEM. Table 2 summarises the emergent themes, subthemes and participants’ quotes.
Table 2: Hybrid deductive–inductive analysis of emergent themes and subthemes of socioecological factors affecting implementation of PHA and DDA in Madang Province
| Themes | Subthemes | Illustrative quote(s) |
|---|---|---|
| Public policy | Providing leadership in enforcing and ensuring policy implementation at the macro level | ‘So, if the leadership at the district and provincial levels is well established, they can plan, lead and organise the health services in the province and district.’ (Participant 022) |
| Fragmentation of responsibilities at the subnational levels | ‘No help from each other, province and district and that traditional partnership has been there, and we help each other; however, even as I say about the reform and the changes that are happening till now and as policy implementers in Madang, there is a considerable challenge. There is a massive gap between the provincial health authority, district administration and partners.’ (Participant 011) | |
| Limited policy framework to promote collaboration between PHA and DDA | ‘What we face here is that our leaders and our program managers are not open to collaborating or working with the member of parliament to discuss our problems with him. No policy is in place to guide the PHA and district administration.’ (Participant 019) | |
| Community | Pathways to reach out to rural communities | ‘It is difficult for us to get to health facilities to seek medical care, so I think health workers strengthen programs for communities like immunisation and other programs. In that way, they can reach us because we cannot travel to the health centre.’ (Participant 017) |
| Caring for staff as an inhibitor to recovery | ‘I was unconscious when they brought me to the health centre. However, at the health centre, nurses and doctors attended to me with a smile and a caring attitude. I felt much better when I saw them. They also treated me with the correct medication.’ (Participant 012) | |
| Institutional | Capacity management of rural health facilities | ‘They should review the program managers’ positions and other positions at the district level; if these officers are established well, they can be better able to plan and organise the health services at the district level.’ (Participant 029) |
| Organisational operations and management support | ‘So if we want to get medical supplies, we must fund our travel to Madang/Lae. We have no transport, and this logistics [company] usually do not bring/transport our medical supplies to us at the health facility.’ (Participant 023) | |
| Interpersonal | Limited influence of PHA leadership at the district level | ‘I see that there is a big gap, so there is a need to have a policy in place to support the collaboration between PHA and DDA. So the PHA only assists most of the time with program activities such as immunisation programs but not with the recurrent expenses support or support the health facility operations.’ (Participant 019) |
| Leverage multisectoral partnerships and resources | ‘Anything like fuel for clinic runs, or any of that sort, we refer them to DDA, but after member [name withheld] was put to court, all of this assistance came to a halt. We no longer receive help from DDA. PHA, for family health service, maternal health through UNICEF and WHO programs in partnership with PHA, through that, they come to run our mobile clinics throughout our catchment area from time to time.’ (Participant 013) | |
| Intrapersonal | Giving oneself to help others | ‘One strategy or comment I would like to make is that, especially with TB, I used my pocket money to provide TB care services and to mobilise and reach out to the community with TB. We went to several places within the district without providing food, transport or a travelling allowance, which was nil. We have used our own money for the sake of our people.’ (Participant 015) |
| Optimism and hopes for continued support from the PHA | ‘Two or three weeks ago, the chairman of PHA met with us, so hopefully, we will continue well until the end of the year and next year. I believe in service delivery to reach the most remote parts, I believe in the new PHA management, and I believe things are looking good for the years to come.’ (Participant 021) |
DDA, District Development Authority. PHA, Provincial Health Authority.
Intrapersonal factors
Giving oneself to help others
Health workers have perceived a lack of support from the PHA, which has had personal implications for their health at the service level. Despite the limitations of PHA in implementing rural health services, health workers have taken the initiative to mobilise their resources to reach out to rural communities. The participants have underscored the critical importance of promoting health equity to humanity and reducing health inequality among disadvantaged populations, highlighting the urgency of this issue:
We can’t delay any further. Similar to the TB program, we are deeply worried about the health of rural communities because we lack the resources to encourage mobility. For the sake of humanity, I personally funded my travel to these communities to conduct follow-ups. (Health facility staff 014)
Optimism and hopes for continued support from the PHA
Despite the challenges, health workers are keen to cooperate and support the implementation of the PHA policy in rural districts. They have shown their readiness to follow clear instructions and directives from the policy level. The participants believe that the leaders of the healthcare system need to step up and provide the necessary clarity and guidance for implementing the PHA policy:
We are prepared to implement the PHA in accordance with the provincial health authority’s requirements. If they choose not to move forward with the PHA and offer us support, we will be left without action, simply waiting for progress. We need guidance and clear directions to follow. (Health facility staff 007)
Interpersonal factors
Limited influence of PHA leadership at the subnational level
Leaders are both relationship- and task-oriented, with collaboration depending on the strength of those relationships. Health workers believe this is best achieved through sustained partnerships with the DDA and by leveraging the DDA’s leadership skills. They argue that effective collaboration is most strongly influenced by leaders who excel at developing and maintaining relationships with their teams, thereby creating an environment in which colleagues can foster close working relationships. The role of leaders in shaping such an environment is vital, as it directly influences the quality of collaboration. However, they note that limited district-level leadership is a barrier to effective cooperation and partnerships with key stakeholders, such as the DDA. Participants expressed concerns about the lack of visibility of PHA leadership at the district level:
We, the public servants and program managers, meet to discuss which political resources they could support. PHA is not present at the district level and therefore cannot influence political decisions. (Participant 023)
The district authority (DDA), a political body, frequently does not invite our program managers and health facility managers to their meetings. They are rarely invited, making it difficult for them to influence decisions. Typically, our managers are excluded from their meetings and planning sessions. Provincial leaders need to collaborate with district administrations. (Participant 019)
Institutional factors
Capacity management in rural healthcare facilities
Participants emphasised that providing sufficient healthcare resources is not merely a matter of policy implementation but is a lifeline for rural communities. They underlined the importance of timely, consistent provision of healthcare resources to achieve the goal of rural health services. However, the lack of essential healthcare resources was a significant barrier to rural health services, directly affecting the health and wellbeing of rural communities. The health workers perceive that factors such as staff resourcing challenges, supply chain issues, slow leadership, and internal processes hinder the PHA’s ability to respond to demand at the district level:
Since the introduction of PHA, they have not provided the resources we need, such as transport or separate vehicles for family health services, because this program plays a significant role in providing data and statistics for Madang Province. We do not have an ambulance; they do not provide one. The very slow appointment of senior officers at the provincial level also affects healthcare services in rural districts. (Health facility staff 003)
Organisational operations and management support
Many participants reported that organisational operations and management support are key facilitators of effective policy implementation. They also highlighted the complexity of these operations, which arise from multiple tasks and processes, and the need for their valuable expertise and skills. Participants perceive the primary function of the PHA as promoting policy implementation to ensure that health services can survive, develop and function optimally. Additionally, participants believe there is a deficit in the management of PHA operations, including operations management, logistics, implementation and the production and delivery of health services:
We no longer provide outreach clinics, follow-up care, or medications to TB patients who have been discharged and have not returned for medical consultation, or to default cases. We cannot conduct follow-ups without management’s support. (Participant 015)
If we wish to obtain our medical supplies, we must arrange funding for our travel to Madang or Lae. We currently lack transport, and the logistics company engaged to deliver drug supplies typically does not transport our medical supplies to the health facility. (Participant 009)
Community factors
Pathways to reach out to rural communities
Participants emphasised the importance of reaching out to rural communities. They explained that primary healthcare programs, such as childhood immunisation, maternal and child health services, community hygiene, health education and awareness, and outreach programs, provide rural communities with opportunities to access basic health services. They elaborate that if these programs are effective, they act as a conduit for rural communities to access essential health services. However, participants stressed that multiple socioecological determinants, including infrastructure deficiencies and poor road and transport access, exacerbate implementation challenges. One participant, in particular, highlighted the importance of strengthening the capacity of health centres to mobilise and engage with communities. However, they reiterated that these services cannot be provided effectively because of limited capacity at health facilities:
I cannot seek health care here at this facility without an ambulance. I pay a small ambulance fee, which I consider reasonable. Otherwise, I can’t afford it. The workers should visit our villages, conduct child immunisations, and treat sick children at home, making it much easier for us. However, these programs are sometimes cancelled, and there may be no money to purchase fuel. (Participant 023)
Policy-level factors
Limited policy framework to promote collaboration between PHA and DDA
Participants considered the DDA an essential ally in providing rural health services, which probably reassured and bolstered confidence among the community. They acknowledged the need for continuous collaboration between the PHA and the DDA. The insights indicated that there is no clear policy delineating the roles and responsibilities of these two significant government departments. While there is some informal collaboration at the individual level, the partnership between the PHA and DDA lacks clarity at the policy level. One participant refers to the DDA as a lifesaver, given limited resources:
When we realised that PHA’s funding and support were delayed, we contacted DDA for assistance. Since there’s no policy guiding cooperation with the district administration, we make our own decisions. They assist us in acquiring medical supplies when our stock runs low and purchase the necessary medications for us. (Health facility staff 014)
Providing leadership in enforcing and ensuring policy implementation at the macro level
Participants stressed that such leadership is crucial to the complex task of policy implementation. Health workers responded that policymakers at the PHA level predominantly influence resource allocation to enforce and strengthen rural health services. However, they also noted that other external structural factors, including conflict of interest in discharging the roles and responsibilities and political influence, are inherent characteristics of the socioeconomic and political environment and are visible in the management of the Madang PHA:
Suppose only the PHA leaders, who hold the necessary authority, can come to our district, review and assess our situation, and provide adequate support in areas such as MCH [maternal and child health], TB and disease control programs. If they can assist us, we can perform well in these areas. However, conflicts of interest have resulted in significant financial mismanagement. (Participant 022)
Fragmentation of responsibilities at the district level
Participants emphasised that the fragmentation of responsibilities at the district health management level is a critical issue. Having two district health managers – one appointed politically and the other selected through the PHA’s public employment process – has created a disjointed structure. Numerous participants have noted that this fragmentation significantly affects the district’s organisational framework and healthcare delivery systems. Additionally, the allocation of responsibilities for health service delivery and management is vital. One participant stressed:
It’s essential to emphasise our program manager’s active involvement in district management team meetings. Their commitment and dedication to discussing issues and collaborating with political leaders to enhance health services at the district level are commendable. However, the dual responsibilities and appointments of the politically appointed health officer and the program manager continue to obstruct effective communication and collaboration in the district. (Health worker 025)
Discussion
This qualitative study explored the perspectives of health workers and the community on the factors influencing the implementation of the PHA and DDA in Madang Province. Our findings reveal that the execution of the PHA policy framework is shaped by factors at multiple levels, as illustrated in the socioecological framework (Fig1). This framework, which we regard as the backbone of our study, is essential for understanding the factors that affect policy implementation across different tiers of the health system, empowering policymakers and implementers to make informed decisions. The insights we have gathered are crucial to understanding how PHA policy implementation and the DDA could work together to enhance rural health services in the province. We aim to provide a comprehensive perspective on the implementation of PHA and DDA models in Madang Province, with the SEM playing a vital role in these endeavours4,29.
Intrapersonal level factors
Giving up self for others
Our research indicates that the motivation, self-commitment and sacrifices of health workers are crucial to implementing policies, despite the constraints of current social and environmental structures. As a result, health workers frequently forgo their income to serve in rural communities. This aligns with the work of Odhus et al7, who suggest that health workers who are fully dedicated to their professional responsibilities and ethics can excel, even when facing structural and systemic challenges. This suggests that personal sacrifices bring fulfilment and joy when they resonate with one’s values, purpose and authentic desires. For instance, health workers who voluntarily make sacrifices at their own expense, such as conducting follow-up visits to community members with tuberculosis in rural and isolated regions, experience a heightened sense of purpose, meaning and satisfaction. However, these sacrifices can also adversely affect an individual and their family’s financial stability, leading to financial stress. Subsequently, such stress can impair workplace performance by reducing employee health, commitment and productivity, while also escalating work–family conflicts and deviant behaviours2,30.
Interpersonal level factors
Limited influence of PHA leadership at the district level
Most participants perceive that limited leadership at the district level impedes policy implementation and they emphasise the importance of strong leadership in enforcing health policy measures. A key driver of effective leadership is collaborating with stakeholders and influencing them to secure their support. Participants believe that being recognised by colleagues and district leadership is crucial to successful implementation. Frequently, health workers associate recognition with a sense of belonging, which promotes cohesion and collegiality between health workers and other key stakeholders. This finding is supported by Peixoto Santos Mendes and Campos Aguiar26, who suggested that policy implementation is influenced by numerous actors responsible for the process, as well as the worldviews of these actors, including governmental officials, represented by bureaucrats and politicians, and non-governmental entities, consisting of lobby groups, political parties and the media. This illustrates that implementation is not a one-time event but an ongoing decision-making process involving critical stakeholders operating in complex policy and institutional environments, under pressure from both interested and opposing groups. Therefore, motivation, information flow and the balance of power and resources among key actors significantly affect policy implementation. Overall, overcoming obstacles to policy implementation requires commitment and perseverance from various stakeholders, potentially over an extended period of collaboration and partnership with key stakeholders31.
Community-level factors
Pathways to reach out to rural communities
Participants underscored the need to strengthen connections with rural communities, ensuring access to essential health services. Their insights are crucial for shaping these strategies. This can be accomplished by improving public health initiatives and enhancing the capacity of healthcare institutions to engage and reach rural populations and communities. This aligns with the findings of Marme et al4, who suggest that empowering individuals in rural areas can lead to significant positive health outcomes. This can be supported by public health programs, including child immunisation, water supply and sanitation, health promotion and housing. Moreover, the participants emphasised the need to strengthen the health systems responsible for delivering health services. The limitations of healthcare facilities have significant implications for the coordination and organisation of rural health services.
Institutional-level factors
Capacity management in rural health facilities
Managing the capacity of rural health facilities is recognised as a significant enabler of health policy implementation. Most participants emphasised that while health facilities play a vital role in delivering primary healthcare services, the failure to strengthen their capacities – including healthcare resources, governance and management structures – has serious and urgent implications for the effective implementation of national and provincial health plans. In line with previous studies from other countries, we found that health institutions serve as agents of health policy implementation. They are pivotal in translating national health policies into healthcare services23. This indicates that implementing policy depends on the mechanisms, resources and relationships linking health policies to program activities. It involves both technical and interpersonal dimensions, relying on healthcare institutions responsible for implementation to ensure that health facilities can implement health policies while fostering cooperative relationships among entities such as DDAs. Thus, grasping the context where policy is executed is essential, as global evidence reveals that adopted policies aren’t consistently implemented as planned and may not produce the anticipated results32.
Policy-level factors
Limited policy framework to promote collaboration between PHA and DDA
Access to health services is vital for maintaining good health, and these services must be accessible and readily available. Nevertheless, individuals in rural areas face numerous barriers to accessing care. Many participants noted that a significant obstacle is the insufficient enforcement of comprehensive policy frameworks by the PHA and the DDA in these areas. Past research shows that successful policy implementation requires clear strategic guidance, maximising the roles of individuals responsible for policy translation, adhering to proper governance and hierarchical structures, ensuring sufficient financial resources, facilitating access to supportive implementation agencies, and support from critical stakeholders such as district authorities21,23. Healthcare workers in this study perceived limited guidance from provincial and district health authorities, leaving them in a predicament that could undermine the effective execution of health policies and strategies. Nonetheless, there is optimism. Participants recognised that substantial improvements could be achieved if the efforts of other sectors, such as the DDA, were combined to improve health outcomes.
Fragmentation of responsibilities at the subnational level
The dual appointments of district health managers have not only been a matter of debate; they have also caused significant anxiety among health workers. They have raised concerns about whether this arrangement is ideal or disrupts the current structure of health delivery mechanisms. Some argue that it is easier to seek support from the DDA, represented by the political appointee, while others see this as a critical constraint to the governance structure. These results echo those of Goodman33, who found two opposing camps regarding the costs and benefits of the fragmentation of responsibilities. One group, known as institutional reformers, contends that greater fragmentation will cause unnecessary duplication of efforts and heightened deficiencies. Conversely, proponents of public choice theory or localism assert that the emergence of multiple positions, driven by competitive forces, will enhance the efficiency of local health service delivery33.
Limitations
This study, which covers three of the six districts in Madang Province, has limitations that must be acknowledged for transparency and honesty. First, focusing on a single province underscores the need for replication in other provinces to gain a broader perspective. Second, reliance on predetermined theories may have constrained the discovery of new themes. Third, as is typical in qualitative research, the results cannot be generalised to other provinces given their specific contexts. Nevertheless, the extensive application of the PHA and DDA within the PNG health system means that, despite these limitations, the findings could still play a crucial role in decision-making and planning.
Conclusion
This research aimed to explore policymakers’ and implementers’ perspectives on the implementation of healthcare policy frameworks. Our findings indicated a critical need for a collaborative approach to dedicated PHA systems that enhance district partnerships with DDAs. What is new and important about this study is that healthcare providers and policymakers support intrapersonal factors that align with WHO’s strategy for improving access to health services in rural and remote areas34. However, while healthcare providers underscored the importance of interpersonal and institutional factors, policymakers focused on health system factors. This difference raises concerns for policy implementation. Therefore, health authorities must recalibrate their health policies to align with implementers’ expectations. This is crucial because implementers serve as agents for policy implementation and engage with local communities at the district level. Policymakers could prioritise allocating healthcare resources at the institutional level to bolster their capacity to effectively implement key national health policies in rural and remote districts. This approach will probably reduce health inequalities and improve access to health services in rural and remote areas.
Acknowledgements
We appreciate the time and support of all the study participants in the three rural and remote districts.
Funding
This study receives no funding.
Conflicts of interest
The authors declare no conflict of interest in this study.
AI disclosure statement
The authors used ChatGPT (OpenAI) to assist with language editing and enhance clarity, but all conceptualisation, analysis, explanation, interpretation of findings, and final content are solely the authors’ responsibility.
References
You might also be interested in:
2020 - The 'Snake song': a pilot study of musical intervention in Eswatini
2009 - A new model to understand the career choice and practice location decisions of medical graduates