


Introduction
Papua New Guinea (PNG) is the largest Pacific Island country, with the majority (86.8%) of its 9.5 million population living in rural and remote areas1,2. The country is ethnically, culturally, geographically and linguistically diverse with over 800 languages across a geographically challenging landscape and remote areas only accessible by foot, boat or air1.
PNG is a low–middle-income country (LMIC) with a GDP annual growth of 2.7% in 20233. Despite annual GDP growth the combination of economic volatility and weak fiscal management has resulted in unpredictable government spending on social programs and services delivery. This unpredictability disproportionately impacts rural populations, especially women4.
Most people in the country earn their living through subsistence farming, especially through agricultural activities, which contribute nearly 30% of PNG’s GDP. The agricultural sector is dominated by subsistence farmers who produce cash crops such as coffee, palm oil, cocoa, and the informal sectors through gardening and livestock, especially poultry and fishing5.
Immunisation is a cost-effective public health intervention to reduce child mortality and morbidity. In 2018, the estimated global population of children under 5 years was 679 million out of which an estimated 700,000 children died of vaccine-preventable diseases. Nearly all of these deaths occurred in LMICs6. Globally, about 2.5 million deaths of children are prevented by childhood immunisation every year7.
In PNG, routine childhood immunisation activities are challenged by multiple factors: difficult environmental conditions; inadequate infrastructure; deteriorating rural health facilities; and expensive, unreliable communication systems8,9. The national immunisation program for children in the first year of life consists of vaccines for preventable diseases including tuberculosis, tetanus, diphtheria, pertussis, poliomyelitis, measles, meningitis, rubella, pneumonia and hepatitis B. While childhood immunisation services are delivered at health facilities, outreach points and special vaccination events, the provision of these services is impacted by chronic shortage of health personnel and unreliable medical supplies, cold chain and vaccines10 as well as problems with infrastructure such as electricity and water supplies.
PNG’s persistent low immunisation coverage of 39% among children between 12 and 23 months is the underlying causes of vaccine-preventable disease outbreaks7,10,11. Examples include a pertussis outbreak in 201112, a measles outbreak in 2013 that saw as many as 75,000 cases13, and 26 cases of poliomyelitis were confirmed during a 2018 outbreak14. In 2022, the estimated coverage for the first dose of measles-containing vaccine (MCV1) was 41%, the third dose of diphtheria–tetanus–pertussis-containing vaccine (DTP3) was 36% and the third dose of oral polio vaccine was 36%9.
In LMICs, the completion of routine childhood immunisation programs depends on many factors. Research findings indicate barriers to immunisation programs such as lack of awareness and distrust of vaccines, family and economic priorities, sociocultural factors and gender norms, communication with health workers and living in remote locations, which influence vaccination-seeking behaviour7,15.
In PNG, a recent study examined factors that influence childhood immunisation uptake and suggested strategies to improve childhood immunisation coverage16. This study focused on health systems factors such as staff knowledge and service delivery practices. Ishida et al (2022) identified the relationship between travel time and economic status to immunisation uptake17. When families live distant from health facilities, children in lower income households are less likely to complete vaccinations compared to wealthier households.
Decisions in relation to health-seeking behaviour is strongly influenced by divisions of roles and responsibilities of men and women within the family18,19. In relation to quality of care, Namuigi and Phuanukoonnon (2005) identified the relationship of health workers with caregivers as barriers to complete vaccinations when caregivers felt they have not been treated in a respectful manner20.
There is a gap in understanding the complex individual, interpersonal, institutional and societal determinants that affect the uptake of childhood immunisation services – understandings that would assist policymakers and health personnel to implement effective immunisation programs.
In this study we adapted the ecological model of health promotion/primary prevention21 because it enabled us to understand the interconnections of individual, interpersonal, organisational and sociocultural factors to create or diminish demand for immunisation of children under 5 years among primary caregivers21-23. The model was easily adapted to the political and cultural context of PNG and its original application to gender was suitable for studying vaccination in PNG. The research question derived from the model was ‘How do individual, interpersonal, organisational and sociocultural factors influence the use of immunisation services for children under the age of five?’
Methods
Study design
This qualitative study was informed by the epistemological foundation of constructivism, which accounts for multiple realities and is consistent with the ecological model24. Constructivism and the ecological model were combined to allow an exploration of socially constructed meanings of factors influencing immunisation services from the individual level to interpersonal relationships, the community, organisational and broader societal level and its interconnectedness21,24. The ecological model was also used as the basis for data analysis and discussion, and adapted to the PNG context.
The study was carried out at the immunisation clinic sites of two rural health centres in the Lufa district of the Eastern Highlands Province in PNG. Data were collected in Tok Pisin by the first author, a Papua New Guinean who is familiar with the settings and has extensive qualitative data collection experience. As the study area is part of the first author’s location of work, regular reflection meetings with the second author were carried out throughout the data collection process to identify and critically reflect possible power dynamics of researcher–participant relationships in the construction of knowledge25,26.
Recruitment and data collection
Purposive sampling was used to recruit participants for individual interviews and focus group discussions27 at the two rural health facilities to consider mothers with children aged under 5 years who experienced the provision of immunisation services. After consultation with community leaders and health workers the first author approached the mothers at the waiting areas of the health facilities, explained the purpose of the study and invited mothers to participate.
A total of 28 mothers between the ages of 19 and 40 years were recruited: 12 participated in individual face-to-face in-depth interviews, while two groups of eight women took part in focus group discussions. Interviews and focus group discussions followed semi-structured question guides with probes derived from the research questions, which were in turn informed directly by the ecological model. The question guides were translated into Tok Pisin, tested and adopted accordingly.
The interviews were carried out in a quiet room at the health facilities and lasted between 30 to 60 minutes.
Two focus group discussions, one at each health facility, each with eight participants, were conducted to discuss with mothers of children aged under 5 years their different and unique experiences in utilising immunisation services. The discussion was supported by a semi-structured guide with open-ended questions including probes to explore interpersonal, organisational and sociocultural factors, and how the interaction across these different levels influences immunisation-seeking behaviour.
The duration of the focus group discussions was between 90 minutes and 2 hours.
All data were collected in Tok Pisin, the local language, between April and June 2021, 1 month before the COVID-19 pandemic significantly affected the area.
Participation was voluntary and participants were verbally briefed about the purpose of the study before they gave informed written consent at the time of interviews and focus group discussions. Confidentiality was maintained throughout data collection, analysis and presentation of findings. Participants were assigned pseudonyms to protect identity.
Data analysis
All data collected were audio-recorded, transcribed verbatim and translated from Tok Pisin into English by the first author. Data were analysed thematically as a combined inductive and deductive process that started with the transcripts of the first interviews28. We read transcripts, thoroughly coded them, and identified and revised patterns, which were organised into themes and subthemes27. We analysed the results by mapping emerging themes against the ecological model of health promotion to examine the interrelationship and influences of the different levels on the uptake of immunisation services, noting no new themes outside the model21. The findings are presented using the ecological model’s levels of themes: individual level, interpersonal relationships, institutional relationships and societal relationships.
Ethics approval
Ethics approval was obtained by the Faculty of Medicine and Health Sciences Research Committee at Divine Word University (FRC/MHS/83-20) and the Eastern Highlands Provincial Health Authority.
Results
Individual level
Knowledge and beliefs about childhood immunisation
Participants shared individual-level factors and explained the importance of bringing their children for immunisation. They described that immunisation prevents and protects children from diseases, which may lead to death. Interview participant Hagivi, a mother of six children, said immunisation is very important and ‘I am happy for what immunisation does to my children. I do not want them to get sick and die’.
A few participants said when they see children admitted to the hospital with serious illnesses they wonder if these children have been fully immunised.
Although the majority of participants support immunisation, knowledge of side effects of immunisation influenced adherence to the monthly immunisation schedule. During the focus group discussion, participants mentioned fear of side effects of fever, swelling at the injection site, crying and unable to move legs for days.
Side effects like fever, swelling at the injection site, crying and irritability in the afternoon prevent us from bringing children to immunisation services. (Fatigi)
Some believed that vaccine-induced side effects would reduce a child’s growth.
Vaccines spoil the child’s growth, and the child will not grow properly because of the bad effects like fever and crying a lot. We will not bring the children again for vaccination. (Dareva)
Luanga, a mother aged 27 years with two children, lamented that although her daughter received vaccines, she was often sick. Although understanding that immunisation prevents diseases, she felt fooled by health workers. According to Luanga, ‘vaccines are the gateway to bring diseases to the children rather than preventing them. My child continues to be sick. For this reason, at times I do not bring my child for immunisation’.
During the focus group discussion, one participant referred to the COVID-19 pandemic. She said many mothers believe that the routine vaccines are like the coronavirus vaccine and are afraid that the vaccine’s ingredients will have a negative effect in the children’s lives.
Trust in medical knowledge and a higher power
A few mothers in both focus group discussions and interviews trusted the health workers as trained people with experience. When the workers promote vaccines, participants trust and follow their advice.
I am from the village with limited knowledge and trust whatever information given by health workers and follow it. (Boavi)
During two interviews and both focus group discussions, mothers highlighted the importance of trusting God first. According to them, God is the giver of knowledge so that health workers can provide good immunisation services.
As for me when I take my child to be vaccinated, I know that God gave the health workers and those who produce vaccines the knowledge to do their job. (Yofa)
Interpersonal relationships
Family and community
In PNG, on an interpersonal level, good relationships and support from family members contributed to mothers bringing children to immunisation services. Some participants mentioned that their partners and relatives encourage them to bring the children for immunisation and receive financial support for the bus fare.
However, not all women experience such support. Fivaro, a single mother, must save money from her small income to pay for transport to bring her child to receive vaccination.
No, my family members do not support me. They say that we have no money. What little you get from the market use it wisely so they don’t give money for transport to access immunisation services. (Fivaro, interview participant)
Participants discussed gender roles of women and men in the family. Women are responsible for the domestic sphere including taking care of children, animals and working in the garden as well as being responsible for harvesting. Focus group participant Borua explained that ‘my husband is very supportive; for example, now I am here, he is picking coffee and taking care of the animals’.
Interview participant Manginoro, who has two children, described that she did not receive support from relatives or her spouse. She views her husband as unsupportive since he considers it as women’s responsibility to care for the children and bring children for immunisation services.
Only one participant explained how she and her husband share responsibility.
My husband brings the child for vaccination, while I do household chores and other livelihood activities. (Mary)
Participants highlighted the division of labour between men and women. Most participants grow coffee, and it is their role to harvest and sell the coffee. Some mothers even live in huts built in the coffee garden, located far from the village.
During coffee season I am busy and don’t stay in the village. I live in garden huts to work and pick coffee. (Kukunu, interview participant)
As women described their high workload, a typical response formulated by Luanga indicated the reason for not attending immunisation services: ‘I am busy selling vegetables and store goods and not able to bring my child for immunisation’.
Participants described how relatives and older women discouraged them from bringing their children for immunisation. One participant (Lyn, focus group discussion participant) said she was told ‘vaccines spoil the child’s knowledge. The child will not learn well in school and will perform poorly later in life’. However, she rejected these local views and added ‘I tell them, I will bring my child to clinic so that when they get vaccine it prevents them from dangerous illness like polio’. The pressure from relatives and demonstrating resistance to this influence, shared a mother of four children.
My relatives discourage me from vaccinating my child. I tell them it is good and beneficial for my child because I don’t want her to be sick. (Lobu, interview participant)
Institutional relationships
Relationship with health workers
On an institutional level, health service providers influence the utilisation of immunisation services. Participants discussed the relationship with health workers in detail. Some described health workers as impolite und unfriendly, so when ‘health workers get angry at us mothers for not regularly attending immunisation services, I don’t come because they are not polite and shouting at us’ (Rosa, focus group discussion participant). Another reason for non-attendance is poor communication when ‘we don’t receive information of health workers’ visit and don’t come for vaccination … our children miss a dose’ (Sena, focus group discussion participant).
Oripa, a mother aged 23 years, added information about the tension with health workers: mothers who do not attend antenatal clinics or have close interpregnancy intervals were scared to attend immunisation services due to the unfriendly way they were treated.
Mothers are shy because they have children with close inter-pregnancy intervals and do not attend antenatal clinics. They are scared to come for vaccination when health workers talk to them harshly. (Oripa, interview participant)
In addition, participants wanted health workers to be professional, promote a healthy lifestyle and behave as role models. Participants dislike health workers who – as interview participant Manginoro, a mother of two children pointed out – ‘chew betel nut or smoke while working and talking to me’.
Participants were concerned about long waiting times as well as late arrival and early departure of health workers in the village. Mothers expressed frustrations when ‘health workers pretend to be busy, and we are told to come back the next day’ (Anita, focus group discussion participant). Mothers living in remote areas are especially affected when health workers leave early as they must walk long distances to come to the immunisation points. When they finally arrive, health workers have already left.
The health workers don’t wait to see if some mothers are still coming. They serve those who are waiting for them and then go. If a child comes late, the nurses have already left. (Kukunu, interview participant)
Participants discussed the importance of health workers taking time to educate them about the importance of immunisation, effect of vaccines and its side effects. Only two mothers reported that they received health education.
When health workers come for immunisation services, I hardly heard them doing any awareness regarding immunisation. It’s zero. Such information must come first before serving us with medicine and vaccines. (Lobu, interview participant)
Societal relationships
Culture, values and norms
Social relations linked to culture, values and norms appeared to influence uptake of childhood immunisation services. Participants nominated cultural obligations as key in family and community life, including church meetings, weddings and funerals.
Most identified attending funerals of relatives or community members as barriers to attending childhood immunisation services. Attending the Haus Krai – the gathering place (in Tok Pisin) to remember and mourn the loss of a loved one, friend or community member – and funerals are seen as social and cultural obligations. This event may take place for at least a week or even longer. Non-attendance of the Haus Krai and funerals indicates no respect for the deceased. This leads to conflict and gossip from relatives, especially relatives in-law, with a negative effect on the women.
When there is a death in the village it prevents me from attending immunisation clinic. In our culture we have to show respect to the death. If I don’t show respect, then the village elders and my in-laws will get angry by gossiping and degrading me. (Boavi, interview participant)
Oripa, a mother of two children, pointed out that priority must be given to children despite all sociocultural obligations and events. When the child is sick it is the mothers who will face the consequences.
Priority must be given to my child. It will be my fault, and I face the effect when my child is sick. Social events like parties, deaths and funerals or weddings must be given second priority.
Other social problems such as repeated tribal fights and sorcery-related violence within and between communities reduce immunisation uptake by mothers.
When there are tribal fights due to sorcery related killings it prevents mothers from fighting villages [from attending] immunisation clinic. (Yofa, focus group discussion participant)
Discussion
A socioecological model to explore factors influencing childhood immunisations of caregivers has been used elsewhere in vaccine research22,29. However, to our knowledge this is the first study to explore factors influencing the utilisation of childhood immunisation services using the ecological model in PNG, although other qualitative studies have provided similar results. This study contributed to understanding that decisions to vaccinate a child are influenced by mothers, from individual determinants to interrelationships with family and community, from an institutional to a broader sociocultural level and its interconnectedness.
Figure 1 presents the four levels of the ecological model of primary prevention.
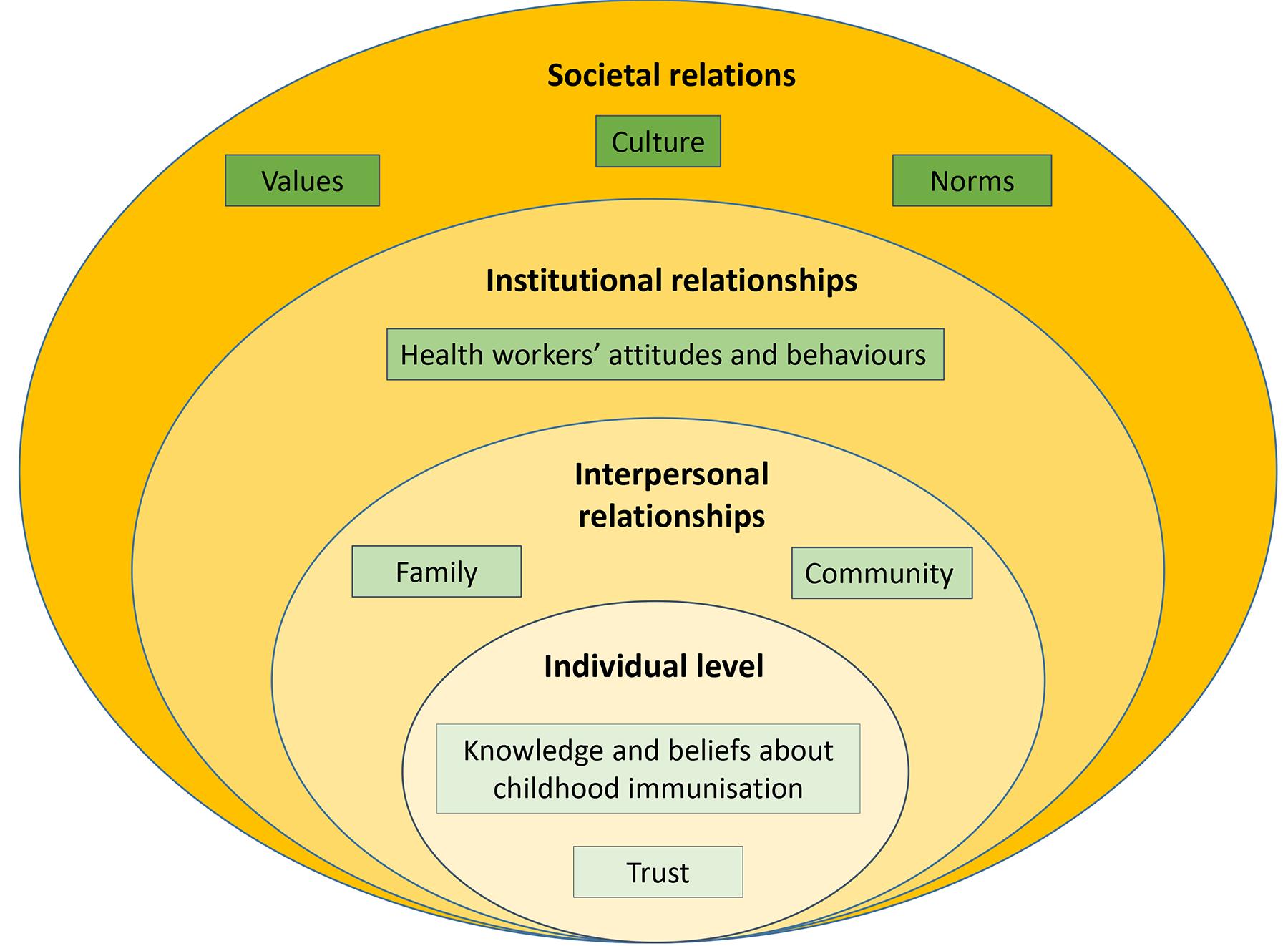 Figure 1: Summary of themes and subthemes of the four levels of the ecological model. (Adapted from Keleher21)
Figure 1: Summary of themes and subthemes of the four levels of the ecological model. (Adapted from Keleher21)
Participants demonstrated understanding about the importance of childhood immunisation but counterbalanced their understanding of the benefits of childhood immunisation and expressed concerns about side effects of vaccines.
Mothers shared their holistic view of health and illness by integrating a spiritual dimension and a recognition that the source of all knowledge is God. While mothers trust the health workers’ biomedical knowledge, the trust in health workers was based on a relationship of familiarity in this particular context15,30. However, mothers’ accounts of God as the source of all knowledge reveal their belief as relational action, with powerful effects in their everyday lives31. This finding is in contrast with the study of Bell et al (2022), stating that the belief in God’s protection may lead to rejection of immunisation services22.
At an interpersonal level, this study is consistent with existing knowledge on the relational influence of the husband and relatives on childhood vaccination15,22,29. This study adds understanding about the positive influence of the immediate family in a patriarchal society in the decision to bring a child for immunisation services. At the same time, our study reveals the influence of gender-based power relations of a patriarchal society in which unequal household and economic responsibilities contribute significantly to women not bringing their children for immunisation services20.
Women’s limited bargaining power and a high labour burden place them at a disadvantaged position in decision-making regarding their children’s vaccinations, illustrating the power dynamics within close relationships32,33. This research shows unequal division of labour. Women are predominantly responsible for much of the labour-intensive manual work in coffee crop production including planting, tending and harvesting. However, the women demonstrated agency, with individual decision-making capacity to act and attend immunisation services34.
Participants’ interpersonal relations, especially with older women’s and relatives’ beliefs about immunisation, were affected by tensions as mothers distanced themselves from misconceptions of older women about childhood immunisation. In this context, mothers created agency and, based on their personal convictions of the benefits of immunisation, decided that their children would receive vaccination35,36.
Our findings suggest that mothers felt some health workers did not always treat them in a polite and respectful manner. Consistent with previous studies15,22,37, unsupportive health workers’ attitudes are barriers that influence mothers’ vaccination attendance decisions38,39. When health workers discount women’s realities, they publicly humiliate women, reinforce existing gender inequalities and ignore the women’s limited decision-making power34,40.
The participants in our study felt they received insufficient explanations on the importance of vaccination, side effects and their management, and the vaccine schedule, as found in other studies37,41.
The misconception about childhood vaccines containing substances of the COVID-19 vaccine, highlighted by one mother, was linked with fear of immunisation services, thus increasing vaccine hesitancy. This issue requires further studies to design culturally appropriate communication strategies21.
Sociocultural and religious factors affect caregivers’ decisions to bring children for immunisation42. Most participants mentioned cultural obligations, such as attending funerals, as compelling time constraints to their children attending the monthly immunisation clinics, delaying vaccine schedule completion. Cultural rituals are crucial and take up to 4 weeks. Not fulfilling these obligations causes disrespect to the deceased, and disharmony in the family and community20. The need to attend to funerals is similar to the commitment in Aboriginal and Torres Strait Islander communities in Australia to attend to Sorry Business43.
Repeated intertribal fights remain a serious social problem in PNG, especially in the highlands20,44. Understandably, study participants raised this concern as an access barrier for mothers and children to utilise immunisation services.
Strength, limitations and quality of the study
The strength of this study was the use of the ecological model to design the study and analyse and interpret the results. This produced a rich understanding of the individual, interpersonal, organisational and sociocultural relationships influencing the utilisation of childhood immunisation from a caregiver perspective. The interviews were conducted in Tok Pisin without any language barriers, which encouraged women to freely express their views.
Limitations included that the study was conducted at two health facilities of one district in the Eastern Highlands Province. The sampling method of our study included only participants who attended immunisation services. Therefore, further research using the ecological model could include caregivers who do not attend immunisation services for their children under 5 years to expand empirical data and develop theories for generalisability.
Conclusion
Decision-making by mothers as primary caregivers is influenced by multirelational factors with families and communities, interactions with healthcare workers, and the sociocultural environment that shapes the utilisation of childhood immunisation. In PNG, culturally significant gender-power relations at interpersonal, institutional and societal levels require close attention within the family, the healthcare setting and the societal environment, suggesting that dialogue around childhood immunisation should take a collaborative approach involving parents, extended families and communities.
The findings of our study suggest that understanding the multirelational factors of the socioecological model that influence decision-making of mothers should be taken into account when redesigning immunisation programs. Initiatives that include health professionals, families and communities have the potential to improve utilisation of immunisation services use and, ultimately, rates of childhood immunisation in PNG. This study adds to evidence for changes in immunisation policies and practice.
Acknowledgements
Particular thanks are due to the women who agreed to participate in this study for their support, openness and for their time in sharing opinions and experiences. Many thanks go to Priscilla Robinson for her assistance in editing the manuscript.
Funding
The authors did not receive funding for this study.
Conflicts of interests
The authors declared no potential conflict of interest with regards to the research, authorship, and/or publication of this article.
AI disclosure statement
No generative AI or AI-assisted artificial tools were used in the conduct of this research or the preparation of this manuscript.