

Introduction
Background
The unequal geographic distribution of healthcare workers relative to populations and, in particular, the struggle to attract and retain healthcare workers in rural and remote areas, is well documented worldwide1-5. Canada is not immune to these challenges6,7, including the province of Alberta8, home to the community program evaluated in this study. As of 2022, roughly 18% of Albertans live in rural areas, yet only 6.6% of medical physicians practice in these rural communities9-11. Unsurprisingly, over 75% of open physician jobs advertised in 2023 were in communities outside the province's two metropolitan centers12. In an attempt to attract more medical school graduates to rural communities, Alberta recently followed the lead of other jurisdictions, offering sizable bursaries to individuals willing to practice in rural areas13.
The probability that healthcare workers choose to practice in rural areas is increased by multiple factors. Research shows that people from rural backgrounds are more likely to practice in rural settings14-17. However, people with urban backgrounds still make up most of the rural healthcare workforce18,19. Consequently, having sufficient exposure to rural practice during healthcare training also increases the probability of working in rural areas5,20-29 and is most influential for urban-raised people18,27. When rural background and training are combined, the probability of rural practice significantly increases18,30-39, with these factors working synergistically to increase the impact more than either would independently40,41. With training, the probability of rural practice increases with rural exposure23,29,33,36,42,43. However, concerns have arisen that overabundant rural healthcare training may cause social isolation and leave a negative impact15.
Less is known about how such factors affect the intent of potential healthcare workers in pre–post-secondary education age groups. Intent is described as an important factor in choosing rural practice15,32,44; however, very little research has considered the effectiveness of programing designed to shape this intent prior to individuals entering post-secondary institutions. Given the importance of rural background, encouraging rural youth to consider a career in health care seems like a natural strategy to increase the number of rural healthcare workers. However, as Mytting et al note, rural youth often face greater barriers to enter healthcare fields compared to urban youth, including having to travel farther distances for schooling, having fewer personal connections to healthcare ‘role models’, and often expressing less confidence in their ability to succeed in the profession45. Thus, programs aimed explicitly at shaping the intent of rural youth that are located in rural areas, decreasing the schooling barriers to healthcare fields, offering access to rural healthcare ‘role models,’ and involving practical activities designed to instill confidence in participants may represent an incredibly important model to addressing the scarcity of healthcare workers in rural areas across multiple countries. This study narrows in on the effects of just this kind of pre-adolescent healthcare career program by evaluating the effectiveness of an Alberta-based program that promotes rural healthcare careers in rural areas to local students in grade 8 (aged approximately 14 years).
Young Medical Minds
Young Medical Minds (YMM) was founded in 2015 in Camrose, Alberta (population 18,772) by a local family physician, a registered nurse, and an Alberta Health Services school health promoter. YMM introduces grade 8 students from the surrounding rural areas to the health care field for 6 weeks by following STAN – a fictitious grade 8 student who has injured themselves. The biannual program takes 12 students every semester and exposes them to careers such as emergency medical services, doctors, diagnostic imaging, nursing, and rehabilitation. The program is a joint effort between Alberta Health Services, Covenant Health, the University of Alberta’s rural-based Augustana Campus, and community volunteers from emergency medical services, a local physician clinic, the local hospital, and other community services. Additionally, Augustana Campus students interested in youth, health care, or education volunteer and assist in the student’s learning.
Students are recruited to the program by a tour of the local schools, where the next year’s grade 8 students are given a presentation on the premise of the program. YMM is also advertised on public social media pages and spread through word of mouth in the community. Students who apply express reasons for their interest in the program, which can range from them exploring various careers to a specific interest in health care.
The program is designed to showcase the vast opportunities in health care with a focus on possible healthcare careers in rural Alberta. Recognizing that rural exposure and background contribute to the probability of practicing and living in rural Alberta, selection of students is from Camrose and the surrounding area.
Some aspects of YMM are shared across similar programs and others more unique to YMM. YMM is the only program known to the authors (other than Project HOPE46) that provides meaningful exposure to different areas of the healthcare field for more than a few days to students as young as 14. Most other programs focus on high school students for only a day47-51. Additionally, YMM is the only program, to the authors’ knowledge, that provides the students with a prolonged eventful experience and tangible story that they can relate to and remember for many years.
YMM relates to other programs with its emphasis on interactive hands-on learning techniques such as suturing and casting, which programs such as Australia’s Broken Hill Regional Health Career Academy Program48 and Aspire2Health49 employ. The program aims to provide the information at a level the students understand and appreciate, in the hopes that it sparks an interest in a healthcare career, specifically in a rural environment. Similar to the Broken Hill Regional Health Career Academy Program and Aspire2Health, YMM is operated by professionals in their field who volunteer their time to provide expertise and act as role models to the students48,49. While some programs focus more on specific careers in health care51, YMM takes a similar approach to programs that promote health care in general by showcasing many careers, specifically those that STAN encounters on his journey through the healthcare system47-50. Acknowledging that not only content and hands-on activity are important for an immersive experience, each YMM session is held in a healthcare facility that corresponds with that session’s occupation. This unique feature is most similar to programs that feature tours of workplaces and hospitals47-49. Recognizing the importance of rural training, YMM culminates with a tour of the Augustana Campus wherein the participants are introduced to the undergraduate opportunities available in a rural setting prior to further healthcare training. Travelling to post-secondary institutions is uncommon in similar programs46. YMM is one of the only programs known to the authors that emphasizes the importance of rural post-secondary education.
Study aims
Overall, the goals of YMM are to spark an interest in health care, highlight the large number of healthcare-related career opportunities in rural settings, and encourage an interest in rural educational institutions. After 9 years of the program's operation, many of the students who participated in YMM have entered into professional lives and careers, although many are younger and still in school. The objectives of this study are to determine if, after taking YMM, there is an increase in participant interest and desire to
- enter the healthcare field and/or practice in rural communities
- stay or return to rural areas for work or living
- attend a rural post-secondary institution like Augustana Campus.
Methods
We conducted a retrospective cross-sectional study of the past participants of YMM by sending out an email survey in the summer of 2024 enquiring about their life choices and reflections on the program.
Survey design
The survey was created using Qualtrics XM (https://www.qualtrics.com). To avoid influencing survey responses, the survey was anonymized for responses and tailored to ask questions based on previous responses, which allowed respondents to receive questions only on their specific role with the program. The survey was designed to examine, among other topics, participant demographics and YMM impacts concerning participant interest in healthcare professions, rural areas, and rural educational institutions.
With these pillars in mind, the survey design was built around Kirkpatrick’s four-level evaluation model for evaluating surveys using a combination of multiple-choice questions, Likert questions, and matrix questions, often with the option of elaborating through open-ended text-boxes52. The participants were asked a series of 36 questions in a 10–20-minute survey that they were able to save and return to if needed. Questions pertained to participants’ reactions to the program (if it piqued interest in different healthcare and academic fields, and the efficiency, time-management, and organization of the program), their learning from the program (activities completed, and attitudes changed from the program relating to school, the healthcare field, and rurality), their behavior after the program (whether their life course trajectory was impacted), and participants’ eventual career paths (who chose health care and in what fields). The survey was reviewed and tested with the YMM administrative team for clarity, focus, and overall layout before being sent to the participants. The data presented in this study represent a subset of these survey results, focusing specifically on student participants.
Definition of ‘rural’
Due to the focus on health care, we defined ‘rural’ based on the magnitude and capacity of healthcare options available, the distance to major centers, and the population size of the community. For this study, we defined ‘rural’ as any place outside of the metropolitan areas of Edmonton, Calgary, and Red Deer based on their Index of Remoteness53. For the Index of Remoteness, we used the Jenks natural breaks classification method and classified rural as all areas 0.2002 and higher (‘accessible area’ and up)54. Although not consistent with Statistics Canada’s definition of ‘rural’55, our classification was similar to all population areas excluding census metropolitan areas56.
Survey procedure
From past records of participation in the program, our team identified and collected the names, email addresses, and phone numbers of 173 student participants from all of the program’s past sessions except for September–October cohort of 2015 as those records were lost. Information was obtained from YMM’s administrative team, who kept records of all past participants who signed the confidentiality agreement and media release form. All previous students in the program were eligible to participate regardless of age. However, if participants felt they were too young to answer the question or unsure of their response, they were given the option to skip it or self-identify as ‘too young’ or ‘not sure’. Of the 173 identified program participants, seven had specified no email address, bringing the total emailing list to 166. These identified program participants were emailed a Qualtrics survey that detailed the purpose of the study and how to complete it. Seven of those emails were not successfully delivered due to inactive email addresses. Participants were given 4 weeks to complete the survey and could close out and return to it as they pleased.
Sixty-six participants responded to the survey, with two withdrawing consent for a final response rate of 64 out of 159 (40.25%) people responding. Consent was collected from each of these 64 identified program participants at the beginning of the survey after participants read the implied consent form outlining the study. Participants aged less than 18 years were asked for both their parent’s consent and the underage participant’s assent. At the end of the survey, participants were once again asked if they wished to continue or withdraw consent for their participation in the study. Any respondents who answered the survey partially and did not reach this final question were not included. Because responding to questions was optional, the number of people who answered each question varied.
Data analysis
After the completion deadline, responses were downloaded and analyzed in Microsoft Excel. Those who had not completed the survey did not have their answers recorded and individuals who revoked consent midway through the study were deleted from analysis. Simple descriptive statistics were compiled into a results sheet, with any Likert questions being transformed into proportional response by taking the proportion of individuals who answered ‘probably yes’ or ‘definitely yes’ to the question.
All statistical analysis and calculations were conducted using R v4.4.1 (R Foundation; https://www.r-project.org) with an alpha of 0.05. A Monte Carlo χ2 test was used in place of a χ2 goodness-of-fit test (due to many semesters having counts less than five) to determine that there was no difference between the semesters that the respondents attended YMM (χ2=17.683, p=0.35). Due to the small sample size and extreme proportions in the survey results, we used the package ‘binom’57 to calculate Jeffreys confidence interval for standalone 95% confidence intervals. Similarly, due to the small sample size and extreme proportions, the non-parametric Fisher’s exact test, exact binomial test, and exact McNemar test were used to compare proportions to pre-existing values, demographic data, and before and after measurements, respectively. The exact McNemar test was conducted through the package ‘exact2x2’58 while the other two were from the base R program.
Some tests required external values that were not collected by the survey. When testing if the proportion of YMM participants who went to university was larger than the rural student average, we used the value of 72% with a standard deviation of 0.01 reported by Wells et al59 as their definition of ‘rural’ was similar to that of this study. For data from census or government data, the definition of ‘rural’ was those living in census agglomerations and below, which is similar to excluding Calgary, Edmonton, and Red Deer in Alberta. To test if the proportion of YMM participants returning to rural areas to live and work was larger than the provincial average, we used the proportion of Albertans who lived9,10 and worked60 in rural Alberta in 2023: 25.66% and 20.26%, respectively. Additionally, to test if the proportion of YMM participants who went or were going into health care is larger than the provincial average, we used the 2021 statistic that 11% of the Alberta workforce is in health care61. Similarly, to test if the proportion of YMM participants who went or were going into rural health care was larger than the provincial average, we used the 2011 statistic that 30.85% of the healthcare workers in Alberta practiced in rural areas8.
Ethics approval
The University of Alberta Ethics Board approved this study (Pro00140951).
Results
Participants’ evaluation of Young Medical Minds
Overall, most of the YMM participants self-identified that the program played a role in who or where they were today (88.71%) and that the program impacted the career they had, or were going into (74.55%; Fig1). Less than a quarter of the participants noted that YMM changed their perception of rural life (19.15%). As a result, half of participants after YMM could consider rural life as a possibility for them (50.00%; Fig1).
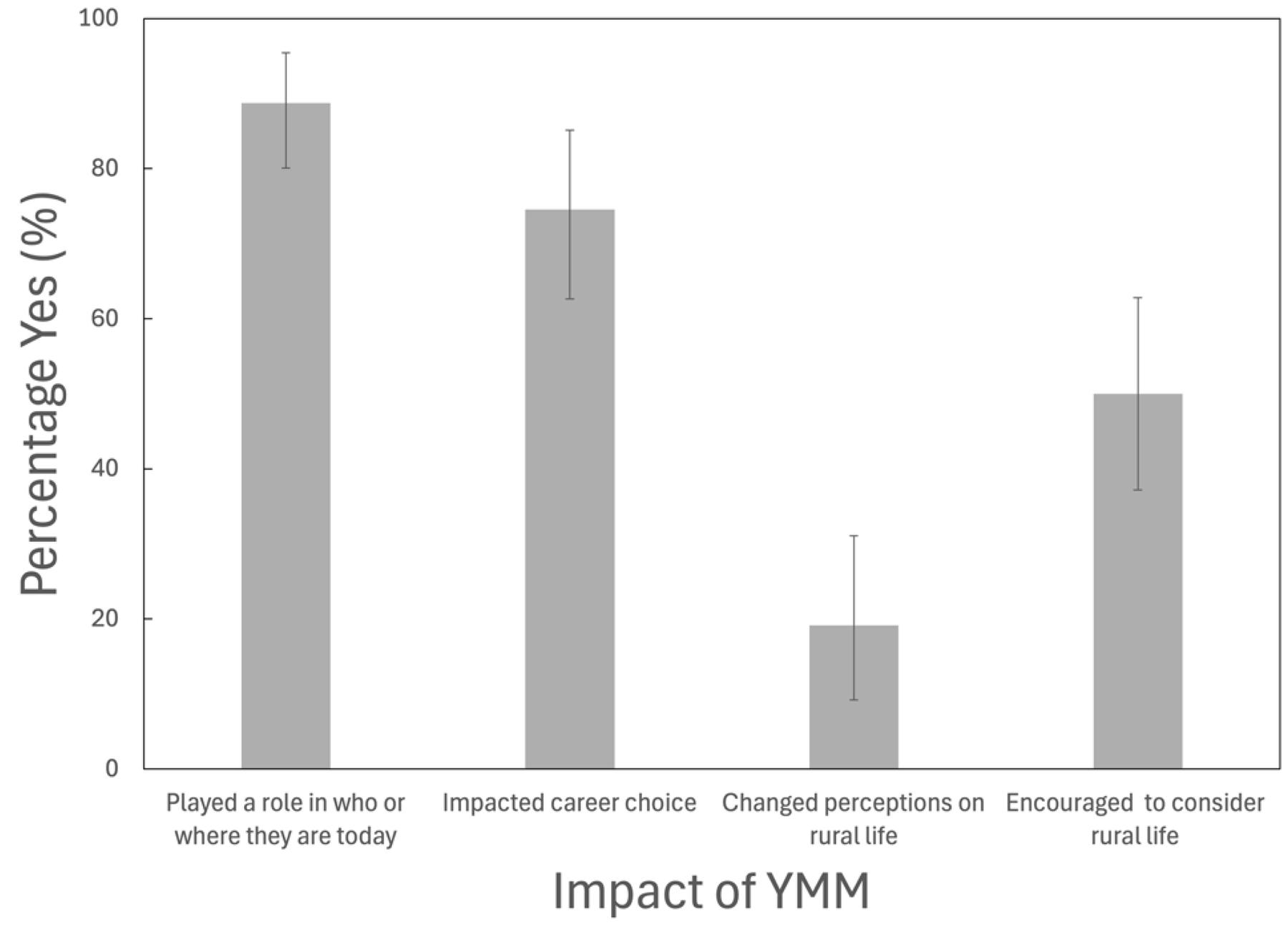 Figure 1: Proportion of Young Medical Minds participants who self-identified ‘probably yes’ or ‘definitely yes’ to the question about Young Medical Minds impacts. Error bars represent 95% Jeffreys confidence intervals, with upper bound not exceeding 100%. Questions (asked verbatim from left to right) are ‘Would you say Young Medical Minds has played a role in who or where you are today?’; ‘Did Young Medical Minds have an impact on the career choice you made or are planning for?’; ‘Did Young Medical Minds change your perception of rural life?’; ‘Has Young Medical Minds encouraged you to consider rural life as a possibility for you?’ YMM, Young Medical Minds.
Figure 1: Proportion of Young Medical Minds participants who self-identified ‘probably yes’ or ‘definitely yes’ to the question about Young Medical Minds impacts. Error bars represent 95% Jeffreys confidence intervals, with upper bound not exceeding 100%. Questions (asked verbatim from left to right) are ‘Would you say Young Medical Minds has played a role in who or where you are today?’; ‘Did Young Medical Minds have an impact on the career choice you made or are planning for?’; ‘Did Young Medical Minds change your perception of rural life?’; ‘Has Young Medical Minds encouraged you to consider rural life as a possibility for you?’ YMM, Young Medical Minds.
Young Medical Minds impacts
Overall, there was a significant increase in the proportion of participants who changed their minds towards the healthcare field (39.22%, χ2=19.42, p<0.001), careers in rural environments (24.00%, χ2=9.84, p=0.002), attending rural post-secondary (19.15%, χ2=6.51, p=0.01), and attending Augustana Campus at the University of Alberta after taking YMM (19.64%, χ2=12.16, p<0.001; Table 1). However, there was no significant increase in the proportion of participants who changed their minds towards living in a rural environment (13.33%, χ2=3.47, p=0.06; Table 1).
Table 1: Proportion of Young Medical Minds participants who changed their goals and views towards the respective characteristics†
| Type of change | n (%) | 95%CI | χ2 | p-value |
|---|---|---|---|---|
| Career goal changed towards health care (n=51) | 20 (39.22) | 26.45–52.62 | 19.42 | <0.001 |
| Changed view towards having career in rural environment (n=50) | 12 (24.00) | 13.25–36.33 | 9.84 | 0.002 |
| Changed view towards living and/or staying in rural environment (n=45) | 6 (13.33) | 4.97–24.21 | 3.47 | 0.06 |
| Changed view towards attending rural post-secondary institution (n=47) | 9 (19.15) | 9.21–31.08 | 6.51 | 0.01 |
| Changed view towards attending Augustana Campus (n=56) | 11 (19.64) | 10.31–30.63 | 12.16 | <0.001 |
† Jeffreys 95% confidence interval, χ2 value, and p-value are shown beside each proportion. From a McNemar exact test, the p-value indicates if the proportion is significantly greater than zero.
CI, confidence interval.
Choices after Young Medical Minds
Health care and rural health care
The proportion of YMM participants who went into or were training for a career in the healthcare field was significantly greater compared to the provincial population (33.87%, p<0.001; Fig2). However, there was no difference in the proportion of YMM participants who chose to or were planning on going into health care and working in a rural environment compared to the provincial average (47.62%, p=0.08; Fig2).
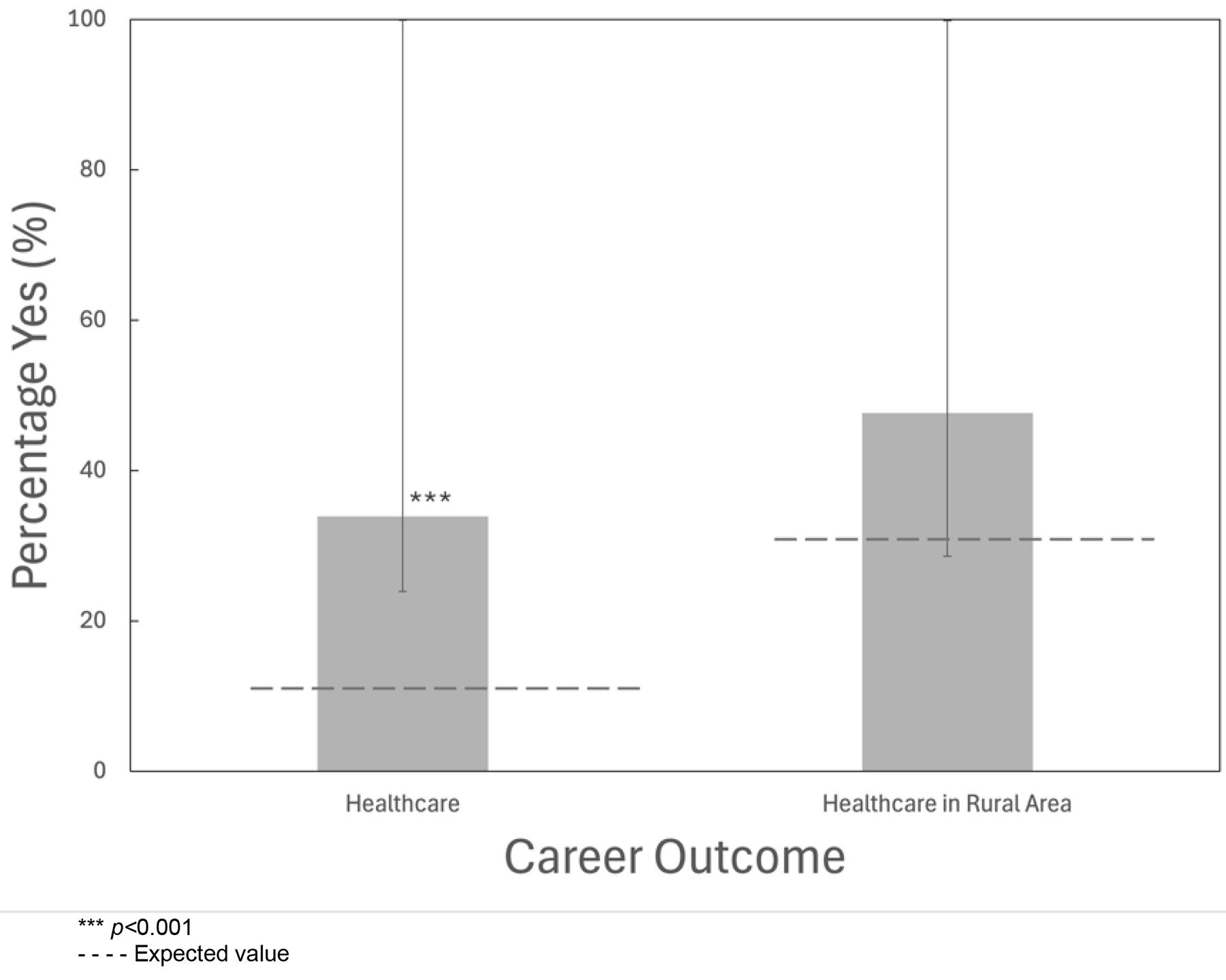 Figure 2: Proportion of Young Medical Minds participants who chose to or planned to have a career in health care and a career in rural health care. Asterisks indicate significance, by exact binomial test, above the expected values of 11%61 and 30.85%8, respectively, given by the gray dotted line. Error bars represent Jeffreys 95% confidence intervals, with the upper bound not exceeding 100%. Left bar represents the question, ‘I went into a career in the healthcare field or am training for a career in the healthcare field’. Data for the right bar were calculated from ‘yes’ responses to the previous question and to the question, ‘I chose to work/plan to work in a rural environment.’
Figure 2: Proportion of Young Medical Minds participants who chose to or planned to have a career in health care and a career in rural health care. Asterisks indicate significance, by exact binomial test, above the expected values of 11%61 and 30.85%8, respectively, given by the gray dotted line. Error bars represent Jeffreys 95% confidence intervals, with the upper bound not exceeding 100%. Left bar represents the question, ‘I went into a career in the healthcare field or am training for a career in the healthcare field’. Data for the right bar were calculated from ‘yes’ responses to the previous question and to the question, ‘I chose to work/plan to work in a rural environment.’
Rural life and work
The proportion of YMM participants who chose or planned to live in a rural environment was significantly greater compared to the provincial average (47.62%, p<0.001; Fig3). Similarly, the proportion of YMM participants who chose to work or planned to work in a rural environment was significantly greater compared to the provincial average (39.68%, p<0.001; Fig3).
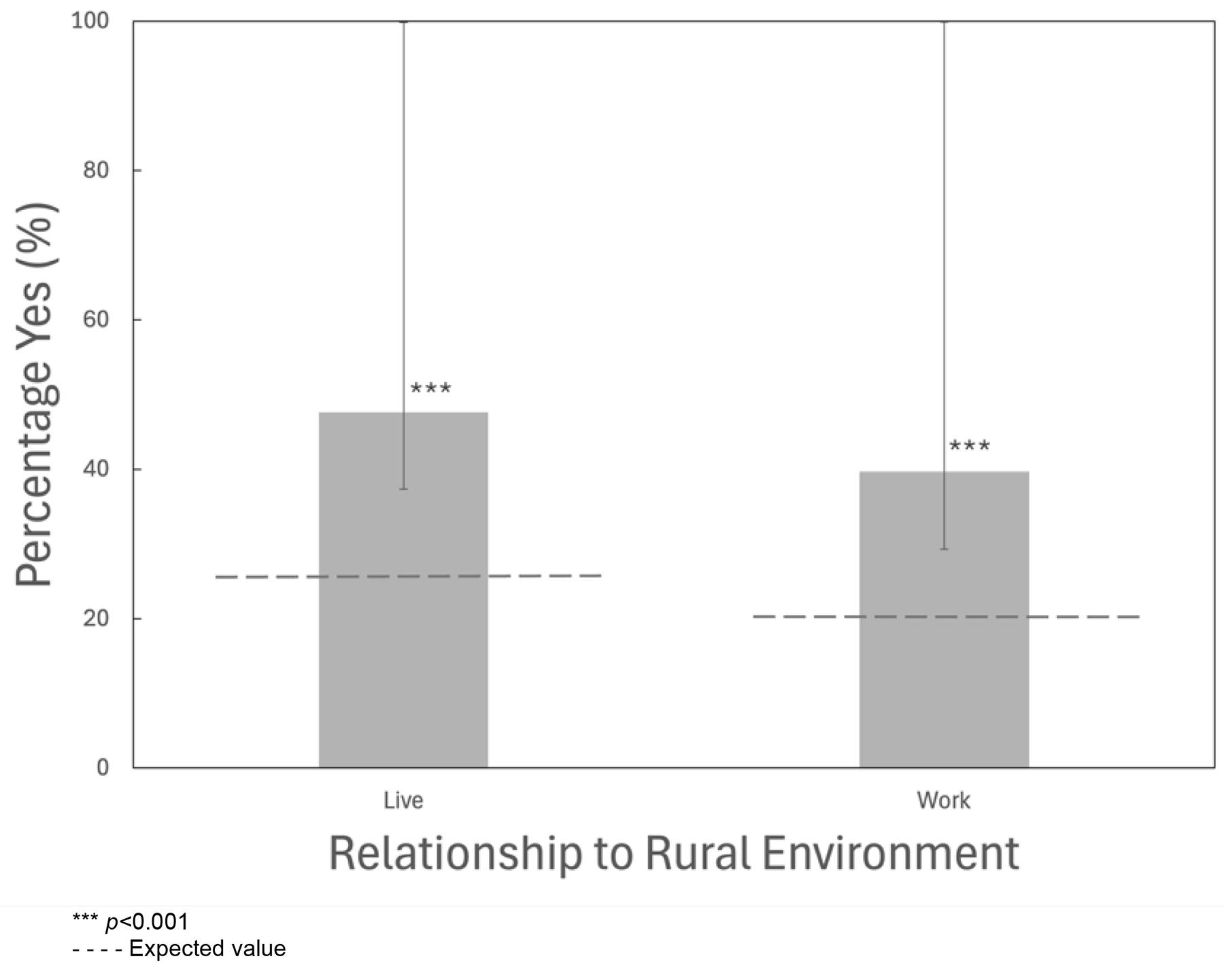 Figure 3: Proportion of Young Medical Minds participants who lived or planned to live in a rural environment and worked or planned to work in a rural environment. Asterisks indicate significance, by exact binomial test, greater than the predicted values shown by the gray dotted line, which are 25.66%9,10 and 20.26%60, respectively. Error bars represent 95% Jeffreys confidence interval, with the upper bound not exceeding 100%. Data for the columns left to right were calculated from ‘yes’ responses to the questions, ‘I chose to live/plan to live in a rural environment’; ‘I chose to work/plan to work in a rural environment.’
Figure 3: Proportion of Young Medical Minds participants who lived or planned to live in a rural environment and worked or planned to work in a rural environment. Asterisks indicate significance, by exact binomial test, greater than the predicted values shown by the gray dotted line, which are 25.66%9,10 and 20.26%60, respectively. Error bars represent 95% Jeffreys confidence interval, with the upper bound not exceeding 100%. Data for the columns left to right were calculated from ‘yes’ responses to the questions, ‘I chose to live/plan to live in a rural environment’; ‘I chose to work/plan to work in a rural environment.’
Rural institutions
The proportion of YMM participants who attended or planned to attend post-secondary institutions was significantly greater compared to other rural students (90.00% and 95.65%, p=0.005; Fig4). Less than half of the total participants who attended or planned to attend post-secondary institutions went to a rural institution (41.67% and 18.18%, respectively); however, over half of those individuals went to or planned to attend Augustana Campus (60.00% and 50.00%, respectively; Fig4).
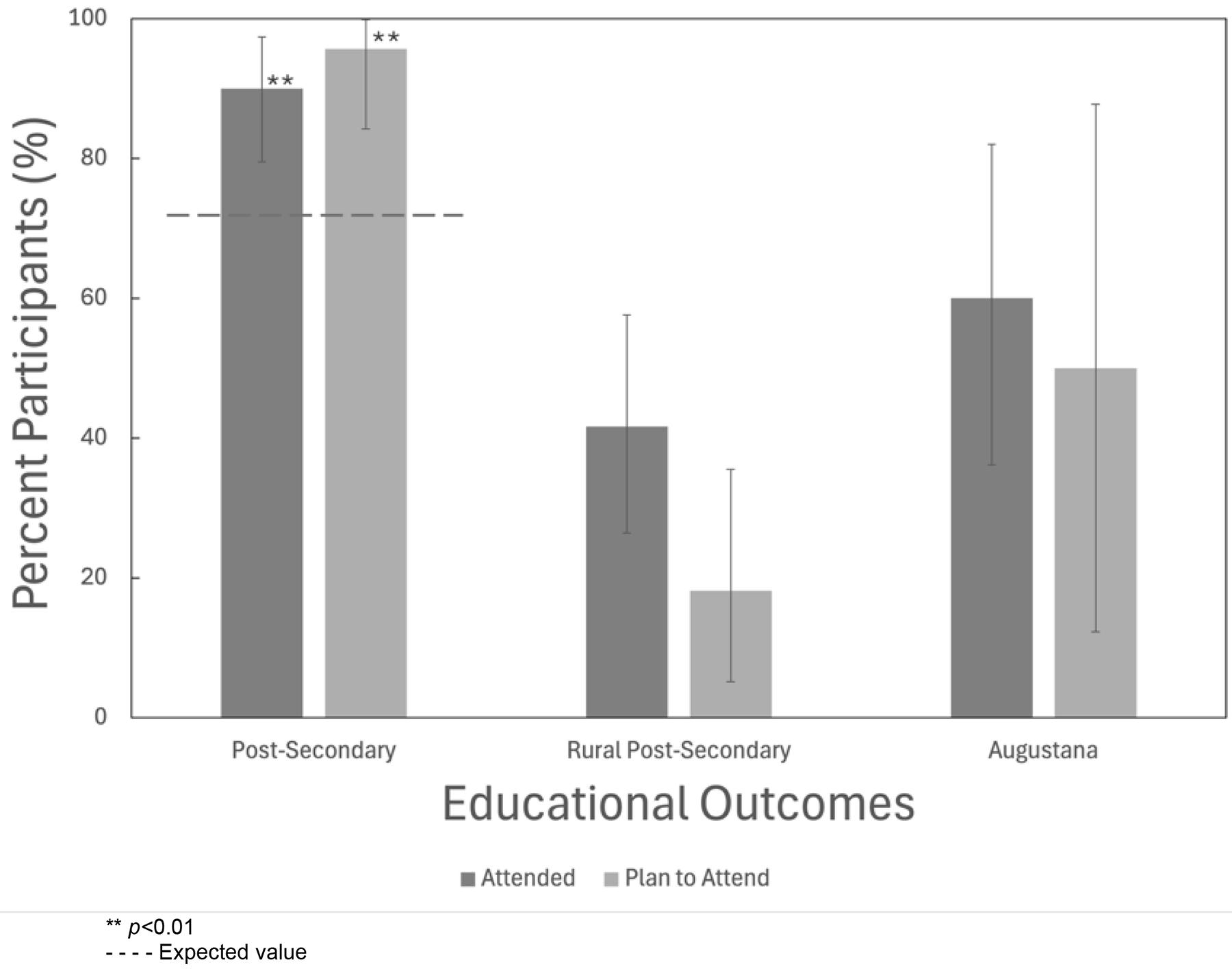 Figure 4: Proportion of Young Medical Minds participants who attended or planned to attend a post-secondary institution, rural post-secondary institution, and Augustana Campus as that rural post-secondary institution. Asterisks indicate significance, by Fisher’s exact test, above the expected value of 72%59, shown by the gray dotted line. Error bars represent Jeffreys 95% confidence intervals, with the upper bound not exceeding 100%. Data for the columns left to right were calculated from ‘yes’ responses to the questions, ‘Did you attend a post-secondary institution?’; Did you attend a rural post-secondary institution or plan on attending a rural post-secondary institution?’; ‘Did you attend or plan to attend Augustana as your rural post-secondary institution?’
Figure 4: Proportion of Young Medical Minds participants who attended or planned to attend a post-secondary institution, rural post-secondary institution, and Augustana Campus as that rural post-secondary institution. Asterisks indicate significance, by Fisher’s exact test, above the expected value of 72%59, shown by the gray dotted line. Error bars represent Jeffreys 95% confidence intervals, with the upper bound not exceeding 100%. Data for the columns left to right were calculated from ‘yes’ responses to the questions, ‘Did you attend a post-secondary institution?’; Did you attend a rural post-secondary institution or plan on attending a rural post-secondary institution?’; ‘Did you attend or plan to attend Augustana as your rural post-secondary institution?’
Discussion
This study demonstrates that YMM participants had an increased interest in careers in the healthcare field, rural communities, and rural institutions. Using Kirkpatrick’s four-level evaluation model, we found evidence that the YMM program impacted multiple levels of the model. From the learning level, we saw that individuals changed attitudes and perspectives on career paths and of rural life. YMM participants also demonstrated behavioral impacts by changing their goals and views towards health care, working in rural areas, and attending rural institutions like Augustana. YMM also had favorable participant results, with many entering healthcare fields, working and living in rural environments, and attending post-secondary institutions – with less than half attending or planning to attend rural institutions.
Promoting health care and rural health care
Consistent with our expectations, our results suggest that YMM increased the number of participants who planned or were going into the healthcare profession. A statistical McNemar exact test supports these findings and we reject the notion that YMM participants changed their minds towards the healthcare field by chance, and conclude that there is a significant increase in participants who changed their career goals towards health care after taking YMM. Similarly, our findings indicate that the proportion of YMM participants who went into or were training for a career in health care was significantly higher than the provincial average.
Our findings support the studies of Robinson et al51, Garrison et al46, and Oshiro et al62, which looked at the effects of interventional youth programs on students’ interest in health care. Similar to our findings, they found that, both significantly and descriptively, there was an increase in students’ interest in health care after taking the interventional program. These studies, combined with our own, increase the knowledge that rural youth initiatives that focus on recruitment in health care can increase the number of students interested in and entering the healthcare field.
However, since many of the respondents were young or still unsure about where they hoped to practice, and the sample size of YMM participants who were currently in the healthcare field and living in rural environments was small, the results of our study cannot speak to the degree that YMM affects the probability of participants actually practicing health care in rural environments. However, the responses do demonstrate that many of the YMM participants going into the healthcare field hoped to practice in rural environments.
Promoting rural life and jobs
Consistent with our expectations, our results suggest that YMM increases participants’ interest and goals towards living and working in a rural environment. Although half of participants identified the program as encouraging them to consider a rural life, the proportion of participants who lived and worked or planned to live and work in rural environments was significantly larger than the provincial average. However, considering these participants come from rural backgrounds, these results are somewhat expected. Conversely, and possibly more importantly, a significant proportion of participants changed their minds towards having a rural career. A statistical McNemar exact test supports these findings and we reject the notion that the proportions changed due to chance, and conclude that there is a significant increase in participants who want to work in rural communities after participating in YMM. However, not entirely unexpectedly, participants were less likely to change their minds towards living in a rural environment – although values approach significance. This is likely because most have had significant rural experiences before participating in YMM. Therefore, our results indicate that, while participants are open to working in rural areas, other factors may contribute to participants being wary about staying in a rural area – these two factors are usually intuitively linked but are not linked in this case.
The success of promoting rural life through youth programs has not always been clear. Mytting et al investigated whether a traveling roadshow that promoted healthcare careers and rural communities would encourage students to stay in rural communities45. Although not as long as the YMM program, the goals of the two programs are similar. Mytting et al found that many participants believed that the program worked although it lacked pre- and post-program analysis for statistical testing45. A study by Oshiro et al tested the effects of an online mentoring program designed to allow students to discuss semi-structured rural and health topics with a professional62. Although not significant, in that study there was an increase in students interested in rural work. Since the YMM program is in-person and more interactive, it may explain why YMM received a more significant outcome than that reported by Oshiro et al62. These studies, along with our own, support the notion that exposure of students at a young age to the benefits and opportunities of rural communities, in the hopes that they stay or return one day, is important.
Promoting rural institutions
The results of our study support the expectation that YMM positively changes participants' views towards attending rural institutions like Augustana Campus. A statistical McNemar exact test supports these findings and we reject the assumption that YMM participants changed their minds towards rural institutions by chance, and conclude that there is a significant increase in participants who attended or wanted to attend rural institutions like Augustana Campus after taking YMM. Additionally, since YMM can increase the chances that participants will attend a rural institution like Augustana Campus, the literature indicates they will also have an increased chance of returning to rural life after they graduate. Therefore, YMM may also inadvertently increase the number of students who return to rural areas by promoting rural institutions. Consequently, our study supports the inclusion of rural institutions in programs like YMM since they provide a significant benefit to the goals and outcomes of the program.
Limitations
While this study provides meaningful contributions to the literature regarding the contributions of YMM to the healthcare field and rural communities, there are limitations. First, the small sample size and many categories leading to even smaller counts within tests are a possible source of error. However, the statistical tests used were chosen to best mitigate these potential limitations of a small sample size. Also, the lack of a control group devalues Fisher’s exact test as it does not conform entirely to conditions since external values are used. Therefore, for interpretive reasons, the McNemar exact test is a more accurate display of the program’s results. Similarly, we can only determine association and not causality in this study because it lacks randomized sampling and a control group.
Second, although there are likely a range of motivating factors that lead students to participate in YMM – such as trying out new things or being forced by a parent – the majority of students enter YMM because they have a pre-conceived interest in health care. As such, this may introduce bias or confounding variables that make comparison to provincial averages difficult. However, since there is a high variability in adolescent career expectations after grade 863, these intentions likely shift greatly; thus, early targeted programs like YMM still offer meaningful influence in possibly decreasing this variability.
Third, our unique definition of ‘rural’ is one of many in a vast array of different definitions64. Although we defined it for our context, our unique definition makes it difficult to compare to other literature not using the same operational definition.
Finally, the difference between outcomes and intent is large. For most questions, the proportion of participants who completed the outcome or intended to complete the outcome are grouped together. While this lack of separation may influence our results slightly, since intent is an important factor for entering health care15,32,44, and individuals unsure or too young to confidently reply were given the option to abstain, we do not believe it will significantly alter results or the impression/validity of the study and impacts of the program.
Future directions
As this is the first study on the impacts of YMM, there are multiple directions for future research. First, replication of the study using a control group (randomized individuals who did not partake in the program) and the treatment group (individuals who took YMM) could increase the power and validity of this study and introduce a causality aspect. Second, although retrospective studies have merit, doing prospective studies on participants for their perspectives immediately before and after taking YMM could provide more short-term results while larger retrospective studies provide more concrete results in the far future. Third, although a large focus of the study is on the YMM participants, the university student volunteers who contribute to the program are also impacted. While all other program contributors (such as administrators, instructors) are already in the healthcare field, the university student volunteers provide a second group that are possibly impacted by YMM. Investigating the effects of YMM on university volunteers and comparing the effects of YMM participants versus volunteers could help illuminate the programs impacts on older individuals already enrolled in a bachelor’s degree and the program’s effectiveness to different target demographics.
Conclusion
This study demonstrates that, through hands-on, extended, interactive, and tangible learning of the rural healthcare field, YMM participants had an increased interest in careers in the healthcare field, rural communities, rural jobs, and rural institutions. Thus, we submit that investing in programs like YMM, which are designed to encourage rural-based adolescents to consider a variety of healthcare careers in rural settings, is worthwhile for policymakers struggling to solve the issue of recruiting and retaining healthcare professionals in rural and remote settings. Additionally, through promoting rural institutions and communities, programs similar to YMM can directly influence the likelihood that participants eventually attend rural-based educational institutions and/or stay in rural communities. While studies on pre-adolescent rural healthcare programming continue to develop, the broader impacts on all participants should be studied – such as those on the YMM university volunteers who may also be encouraged from the program to pursue paths into health care. Therefore, programs such as YMM hold much promise in terms of supporting both the healthcare profession and rural communities alike.
Acknowledgements
The authors wish to thank the journal editors and anonymous reviewers for their constructive comments during the peer review process, the Rural Pathways Internship program at the Augustana Campus of the University of Alberta for funding this work, and the whole Young Medical Minds team for their cooperation and assistance throughout the project.
Funding
This project was funded by a summer internship grant provided by the Rural Pathways Internship program at the Augustana Campus of the University of Alberta.
Conflicts of interest
The authors declare no conflicts of interest.
AI disclosure statement
The authors did not use generative AI or AI-assisted technologies in the research or writing of this manuscript.