

Introduction
Provision of equal access to medical services for all citizens is a challenge for public healthcare systems across many European countries. In many of them, rural areas and other peripheral regions are gradually turning into so-called ‘medical deserts’, whose inhabitants have obstructed access to health care. This leads to deterioration in quality of life and worse healthcare characteristics of the population. This problem, also experienced in Poland, is caused not only by the shortage of doctors but also by the suboptimal dislocation of the medical workforce1,2. While some older definitions focused strictly on personnel shortages, contemporary medical deserts are defined by an insufficient degree of fulfilment of inhabitants’ needs as regards widely understood medical services. Depending on local workforce distribution and service availability, medical desertification can occur in rural and peripheral regions, as well as in selected urban areas3,4.
As primary care is recognized as the key level of care responsible for ensuring equitable access, the skillful management of the workforce entering the medical job market is fundamental to preventing the emergence of these deserts in the long run5,6.
To combat the emergence of medical deserts, high-income countries with large territories have historically implemented strategies ranging from utilizing GPs for specialized tasks to experimenting with telehealth and healthcare facilities providing specialized services7-10.
Determinants of professional attitudes and decisions in the healthcare sector
While professional career models have globally evolved into dynamic, individualized sequences, the healthcare sector remains more stable and predictable because most medical professions are highly regulated and require long periods of professional training11,12.
Such an individualization of a career path is influenced, among other things, by:
- deregulation of a number of professions and emergence of completely new ones
- popularization of alternative forms of employment (employment relationships, as well as business-to-business relations)
- decline in fertility rate, advancement of gender equality and increase in social acceptance for alternative family models
- generational valuing shift and an increasing search for the equilibrium between professional, private, family life and self-fulfillment in non-professional spheres of activity.
In Poland, systemic planning remains insufficient. A recent audit by the Supreme Audit Office covering the years 2018–2022 revealed that the activities of the Ministry of Health are only of an emergency nature and are not based on any long-term strategy13. The audit specifically highlighted a lack of target numbers for medical professionals and a lack of analytical instruments or data necessary for long-term workforce planning. This creates a critical research gap, as the professional decisions taken now by medicine students will have a significant impact on the distribution of medical staff in Poland for decades. As a result, isolating the determinants of professional plans for future doctors and developing mechanisms to influence those choices should be a priority for national healthcare policy.
Aim of the research
The current study aims to determine the preferences of medicine students towards planned specialization and workplace – understood both as a type of institution and a geographical location – as well as to isolate the determinants of choice of the medical profession.
Methods
A computer-assisted web interviewing questionnaire study was conducted anonymously with students in their first, third and sixth years of medicine at the Medical University of Warsaw.
The survey aimed to quantitatively assess motivators for choosing a medical specialization. Prior to the main study, the questionnaire underwent cognitive pretesting with five medical students to verify item clarity and face validity.
Minor revisions were introduced before launching the final survey. An electronic questionnaire link was sent to class representatives from each relevant year with a request to distribute it to all eligible students. Participation was voluntary, and data were collected online via LimeSurvey Professional in January–February 2024. In total, the questionnaire was completed by 434 participants (overall response rate 12%).
Statistical analysis
The research questionnaire, authored by the team, comprised 18 questions concerning motivations for choosing the medical profession, preferred specialization and workplace. The pool of potential determinants was generated based on a literature review and preliminary qualitative research. Three multi-item quantitative scales were employed, with respondents rating statements on a five-point Likert scale (1–5). The reliability of each scale was tested using Cronbach's alpha coefficient (α≥0.70 is considered acceptable and α≥0.80 is considered good). All scales demonstrated acceptable to good reliability, with α values ranging from 0.72 to 0.86. Descriptive statistics, including means, medians and standard deviations, were calculated for each questionnaire item. Group comparisons for continuous variables were performed using student t-test for two groups and one-way analysis of variance (ANOVA) for more than two groups, provided the parametric assumptions were met. When these assumptions were not met, non-parametric tests were applied, including the Mann–Whitney U-test and the Kruskal–Wallis test (H-test). Associations between categorical variables were examined using the χ2 test of independence. Cross-tabulation tables were used to compare initial and final specialization choices between groups distinguished by their characteristics. As completion of all questionnaire items was mandatory, there was no missing data. All statistical analyses were performed using the Statistical Package for the Social Sciences v30.0 (IBM Corp; https://www.ibm.com/products/spss-statistics). The level of statistical significance was set at p<0.05.
Ethics approval
The study was conducted according to the regulations of the World Medical Association Declaration of Helsinki after gaining approval of the Bioethical Commission of the Medical University of Warsaw (no. AKBE/248/2024).
Results
Research sample
The participants of the research can be divided more or less equally into two groups: junior students (first year of studies; 222 participants) and senior students (third or sixth year of studies; 212 participants). The majority of respondents were female (62%) and their percentage was higher in the senior group than in the junior one (67% v 58%). More than half of the respondents (51%) were from cities (more than 100,000 inhabitants), one-third from towns (32%) while few (18%) were from rural areas. At least one parent of 91.6% of the sample had a higher education degree and at least one parent of about a third of the sample (32%) worked in some kind of medical profession. A large majority of respondents (82%) regarded their families’ affluence as high or very high, 16% as moderate and only 2% as low or very low (Fig1).
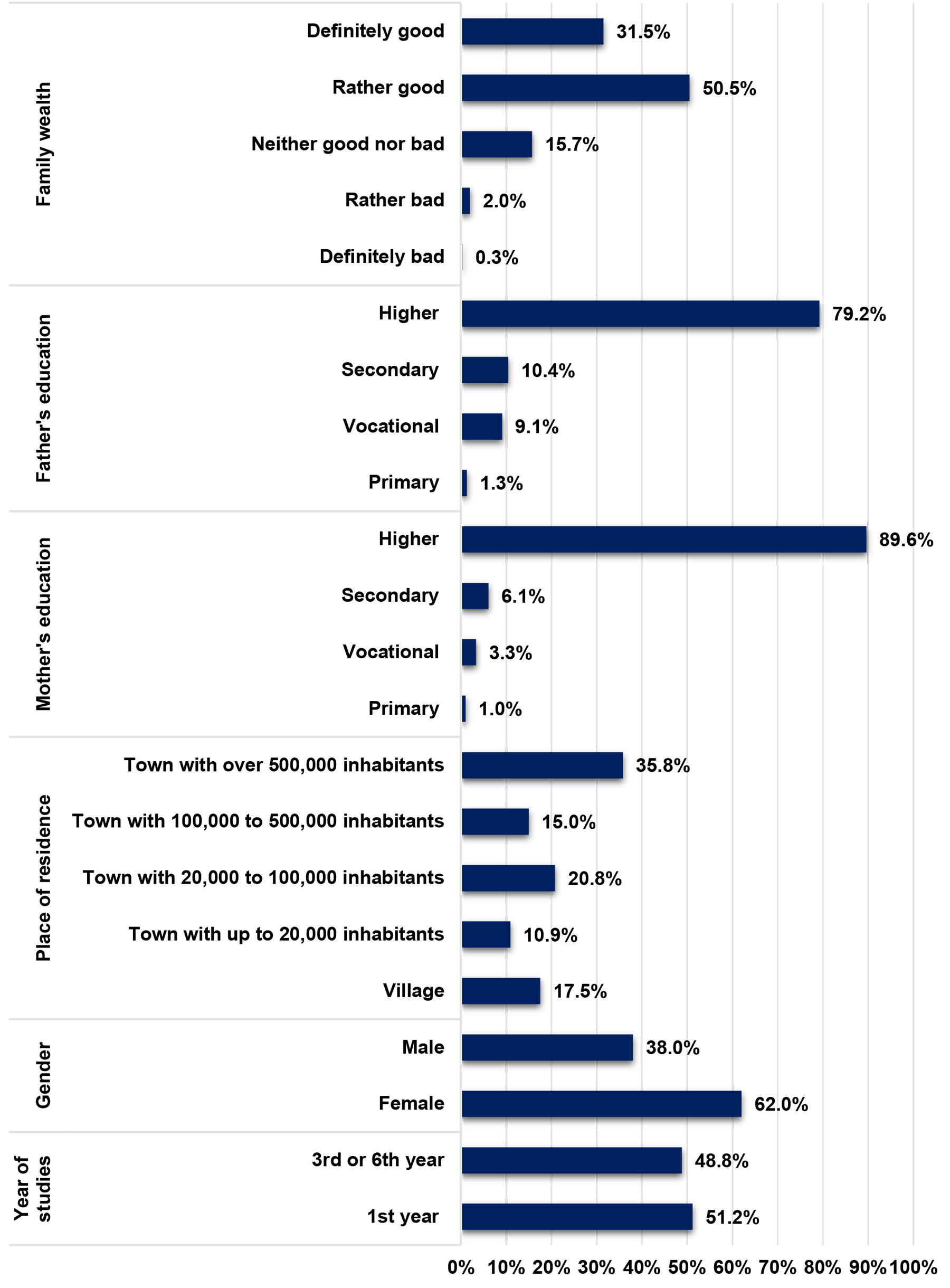 Figure 1: Demographics of study participants.
Figure 1: Demographics of study participants.
Reasons for selection of the medical study program
Out of 16 potential reasons and circumstances influencing the selection of the medical study program, the respondents regarded the following three as the most significant for them (average on a 1–5 scale):
- willingness to have a stable job (4.5)
- desire to have a job that would give something to the world (4.3)
- need for (professional) self-development (4.1).
The least influential factors determining the selection of the medical study program were the influence of mass media, social media and influencers (significance average estimated at 1.3 on a 1–5 scale), encouragement by friends or peers (average 1.4) or by a teacher (average 1.5) (Fig2)
The opportunity for scientific development as a reason for selection of the medical profession was statistically significant for first-year students compared to senior students: 3.04 versus 2.74 (U=20.587, Z=2.25, p=0.02).
Gender had a statistically moderate effect on the perception of the significance of particular determinants of the study program selection. Females found a willingness to help others more significant than males: on average 4.17 versus 3.89 on a five-point scale (H (2, N=395) = 12.97171; p=0.0015). Males found the influence of parents as a slightly more significant factor determining the choice of the future profession: 2.54 versus 2.22 on a five-point scale (H (2, N=395) = 6.86376; p=0.0454), the influence of acquaintances – 1.57 versus 1.31 (H (3, N=396) = 13.23357; p=0.0042), the influence of teachers 1.58 versus 1.39 (H (3, N=396)=7.610963; p=0.0548).
The need for work to be not too difficult and burdensome for the respondents from towns (between 20,000 and 100,000 inhabitants) was statistically more significant compared to those coming from cities (>500,000 inhabitants: 2.18 v 1.73 on a five-point scale (H (5, N=395) = 16.02968; p=0.0068). On the other hand, for the students from cities, chance was a more statistically significant determinant of the selection of the medical profession than for those from towns: on average 1.8 versus 1.3 on a five-point scale (H (5, N=395) = 17.14364; p=0.0042).
It was also observed that the students who assessed their family’s material status as either good or very good were more often driven by ‘the need for their work to mean something – to bring something to the world’ than those who had a worse assessment of their family’s material status: on average 4.4 versus 4.1 (H (2, N=394) = 9.484884; p=0.0087).
Students who assessed their family’s material status as very good were more likely to choose medicine for their career because they desired to ‘earn much’ (statistical significance at the strong tendency level: p=0.08) and ‘have a prestigious job’ (statistical significance at the strong tendency level: p=0.09).
Those who were struggling with a chronic disease and those who did not want to answer that question slightly more frequently suggested that their motivation to choose medicine as the program to study was influenced by trauma, disease or some other difficult situation in life of themselves or their loved ones.
 Figure 2: Perceived significance of particular reasons influencing selection of medical study program. SD, standard deviation.
Figure 2: Perceived significance of particular reasons influencing selection of medical study program. SD, standard deviation.
Choice of medical specialization
As few as 31.1% of the student participants admitted having firm plans for the choice of the medical specialization. It was slightly more frequent for senior students than junior ones (36.3% v 26.1% (χ2=5.26, degrees of freedom=1, p=0.0218). Around 41% of the respondents considered choosing out of a few specializations they had in mind while 27.9% did not have any plans or preferences in that respect.
Out of 77 medical specializations formally registered in Poland, 44 were reported as of interest by the respondents (who were free to choose two). Those most frequently mentioned were general surgery (10.3% out of the whole sample), psychiatry (9.0%), anesthesiology and intensive care (6.1%), pediatrics (5.8%), neurosurgery (4.8%), endocrinology (4.2%), obstetrics and gynecology (4.2%), neurology (4.2%), cardiac surgery (3.8%), cardiology (3.5%), orthopedics and musculoskeletal traumatology (3.5%), and internal diseases/ internal medicine (3.5%).
There was no statistically significant effect of gender, place of residence, family prosperity or other sociodemographic factors on specialization choice.
Half of the respondents (50.5%) mentioned the hospital as the preferred place of work in the medical profession. A quarter (26.5%) preferred to work in a solo medical practice while under 15% opted for a private large medical network. The medicine-supporting industry (including, among others, the pharmaceutical sector, the insurance sector and new technologies) was of interest to a very small number of respondents (about 2.7%).
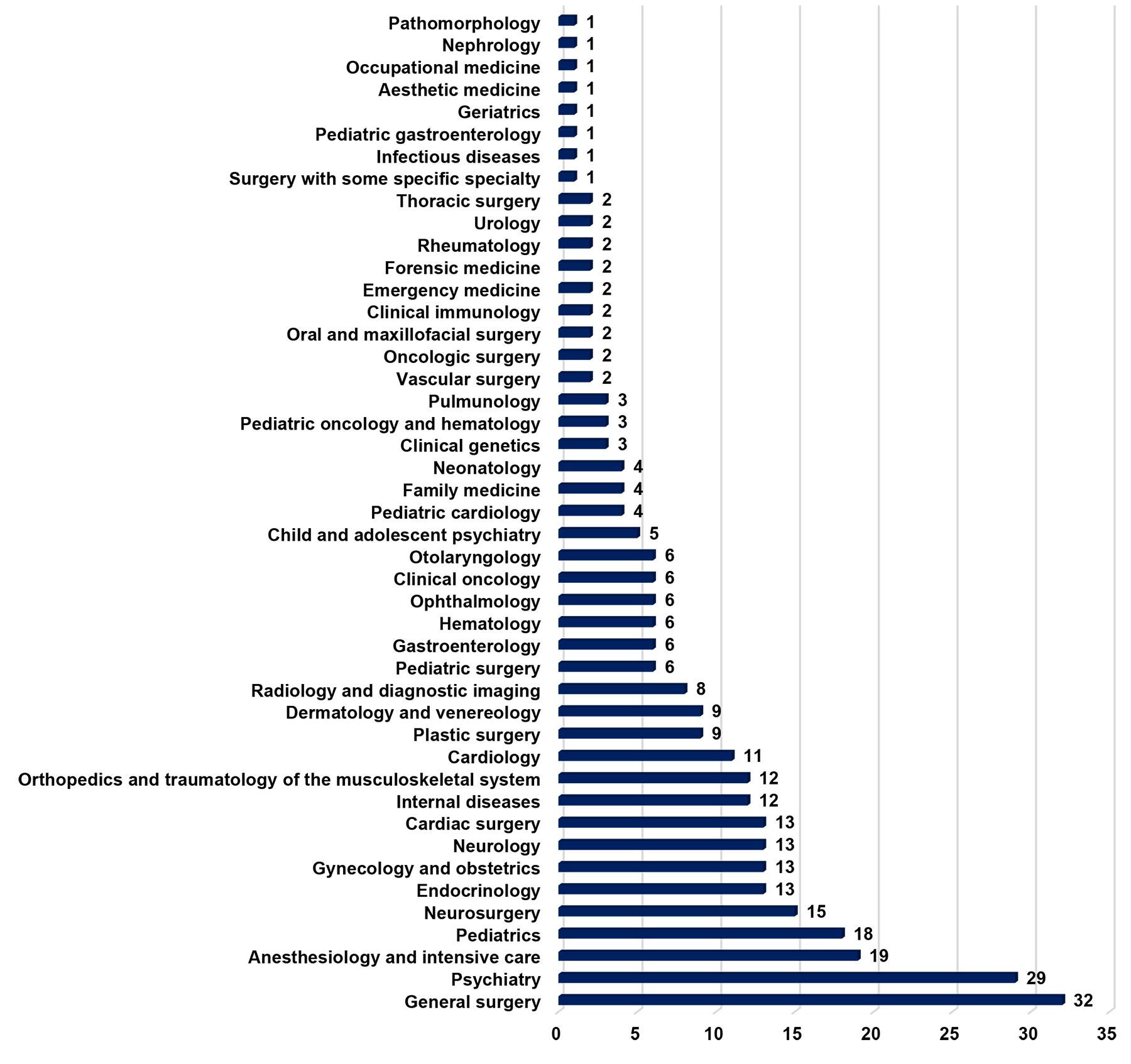 Figure 3: Choice of medical specializations by study participants.
Figure 3: Choice of medical specializations by study participants.
Geography of professional plans
As many as 30.4% of the respondents admitted that they would like to work in the same city in which they studied (Warsaw); 22.5% would preferred to work in the place of their permanent residence (Warsaw in two-thirds of the cases).
Only 9 out of 69 respondents living permanently in rural areas preferred to stay there while only two mentioned their plans to move from the city to the country. Very few participants wished to live in cities other than Warsaw.
One out of eight respondents planned to move abroad; most frequently these were students from Warsaw (42.9% out of these) and from middle-sized towns up to 100,000 inhabitants (26.5%).
ANOVA analysis revealed statistically significant differences in the assessment of selected location factors between groups (Table 1). Significant differences were observed for the following statements: ‘I would have close friends there’ (F=20.694, p<0.001), ‘It would be peaceful there – without an excessive workload’ (F=10.379, p<0.001), ‘It is possible to earn well there’ (F=4.602, p<0.001), ‘It would be a good place to live’ (F=2.830, p=0.007) and ‘People need me there’ (F=2.565, p=0.014).
However, no statistically significant differences were found for factors related to the medical workplace itself, including the presence of a desired medical employer (F=1.754; p=0.096), the medical team (F=1.811; p=0.085), or employment opportunities for a partner (F=1.603; p=0.134).
These results suggest that the migration decisions of medical students are more closely linked to social factors, quality of life and job satisfaction than to the organizational structure of healthcare facilities. This may partly explain the strong preference for staying in Warsaw and the relatively low interest in smaller centers, including rural areas.
Table 1: Preferred future workplace location – analysis of variance of selected determinants
| Statement | Sum of squares | df | Mean square | F | p-value |
|---|---|---|---|---|---|
| It would be a good place to live | 14.799 | 7 | 2.114 | 2.830 | 0.007** |
|
220.350 |
295 | 0.747 | |||
|
235.149 |
302 | ||||
| I would have close friends there | 189.503 | 7 | 27.072 | 20.694 | 0.000*** |
|
385.910 |
295 | 1.308 | |||
|
575.413 |
302 | ||||
| People need my help there | 34.413 | 7 | 4.916 | 2.565 | 0.014* |
|
565.396 |
295 | 1.917 | |||
|
599.809 |
302 | ||||
| It is a good place to earn a good income | 47.243 | 7 | 6.749 | 4.602 | 0.000*** |
|
432.586 |
295 | 1.466 | |||
|
479.828 |
302 | ||||
| It would be peaceful, without excessive workload | 82.639 | 7 | 11.806 | 10.379 | 0.000*** |
|
335.540 |
295 | 1.137 | |||
|
418.178 |
302 | ||||
| There is a medical facility where I would like to work | 24.709 | 7 | 3.530 | 1.754 | 0.096 |
|
593.687 |
295 | 2.012 | |||
|
618.396 |
302 | ||||
| There is a medical team I would like to work with | 27.687 | 7 | 3.955 | 1.811 | 0.085 |
|
644.300 |
295 | 2.184 | |||
|
671.987 |
302 | ||||
| My partner could easily find a job there | 29.689 | 7 | 4.241 | 1.603 | 0.134 |
|
780.568 |
295 | 2.646 | |||
|
810.257 |
302 |
*p<<0.05, **p<0.01, ***p<0.001
df, degrees of freedom.
Discussion
The main finding of our study is that the current students of the medical faculty of the Medical University of Warsaw are encouraged to take up a medical career to the greatest extent by motivations of self-fulfillment: professional stability (most important motivator), self-development (third most important motivator), prosperity (fifth most important motivator) and satisfaction with meeting professional challenges, a sense of agency and belonging to a prestigious group (sixth, seventh and eighth most important motivators, respectively). All this demonstrates some kind of demythologization of the medical profession and at least a partial break-up with the traditional identification of the medical profession with the altruistic mission (an identification shaped, among others, by Polish writers from the Young Poland or social realism periods). One needs to stress, though, that such an actualized motivational scheme contains the willingness to help other people and a conviction that ‘the work should have a deeper meaning – bring something to the world’ as still highly significant motivators (fourth and second most motivating factors, respectively). A slightly similar study conducted among first-year medicine students at the Pomeranian Medical University in Szczecin showed a willingness to help other people as the most important motivator, with an interest in medical sciences in the second place. On the other hand, respondents from the sixth year of the same university listed both motivators in the reverse order. The third and fourth places in the ranking of the motivators most significant for both age groups were occupied by a desire to have a prestigious and well-paid profession, respectively14. It is more than certain that the awareness of those motivators and their hierarchy is a prerequisite to understanding young people’s decisions not only to take up medical studies but also their choice of specialization and workplace. It also enables the development of tools and mechanisms influencing those decisions.
To further interpret these findings, self-determination theory can be used as a useful conceptual framework. According to this theory, motivation and sustained engagement are supported when three basic psychological needs are met: autonomy (eg agency and volition), competence (eg self-development and overcoming challenges) and relatedness (eg belonging)15. From this perspective, the combination of motives observed in the study can be viewed as reflecting the different ways in which students anticipate satisfying these needs. Conversely, overly controlling or purely transactional educational environments may undermine motivation and wellbeing16. This mixed pattern emphasizes the importance of fostering learning environments that nurture autonomy, competence and connection. Training that is purely performance-based and transactional in nature may erode meaning and prosocial motivation, which could affect future workforce engagement and retention.
Beyond individual motivation, students’ career preferences also have implications for workforce planning and equitable access to care, particularly in the context of potential medical deserts in Poland. One positive finding is the relatively high declared popularity of general surgery, anesthesiology and intensive care, and psychiatry – specializations in which workforce shortages are reported not only in peripheral regions. The choice of a future specialty appears to be shaped both by factors operating already at the start of medical education and by the broader motivators that drive the decision to pursue a medical career17. Perhaps at present the greatest impact on the future decisions of young people is exerted by the media, which builds an emblematic (often heroic) image of hospital doctors more frequently than of primary care physicians18. On the other hand, during their university education, young people are influenced by a number of factors that can lead to a change of these early (secondary school) plans for a medical career. As indicated by many studies, the percentage of students declaring their interest in outpatient medicine, including primary care, is rising over the course of consecutive years of studies19.
The dynamics of factors influencing specialization choice are confirmed by the findings from studies conducted with Polish trainee doctors that indicate that contemporary young doctors find such factors (apart from financial motivations) as maintaining a proper balance between professional and private life, having a chance to establish a private practice and flexibility in choosing one’s workplace as crucial for their specialization choice20. It appears that such revaluing takes place not only due to the influence of family and social factors (eg a willingness to return to one’s family members, a search for work–life balance, and parental plans) but also due to the very process of professional training. It has been proven that even minor differences in study curricula at different medical universities might have a significant effect on the percentage of graduates planning (as their first choice) to take up family medicine as their specialization21,22. In this case, both positive reinforcements connected with family medicine training and negative ones (costs and inconveniences of high-profile hospital medicine, especially related to surgery) are at play.
The research yielded noteworthy and disturbing results: interest in rural medicine was minimal among respondents: only 13% of students originally from rural areas intended to return there, and only two respondents from urban backgrounds expressed a willingness to move to the country. Also, family medicine is not among the most popular medical specializations, with only four students declaring their intention to specialize in it. These findings contrast with the WONCA European definition, which describes general practice/family medicine as a primary care specialty that is usually the first point of medical contact. It provides open and unlimited access, managing unselected health problems throughout people's lives23. However, our data indicate very low uptake of family medicine and minimal willingness to work in rural areas. Regardless of the future healthcare model, this specialization remains fundamental to Poland’s health security, particularly in rural communities and regions distant from major cities. Due to the limited health infrastructure and availability of specialist medical services in rural areas compared to urban centers, rural residents tend to rely more heavily on primary care services24. The low uptake of family medicine and limited willingness to work in rural areas observed in this study may hinder equitable access, particularly in areas where staffing shortages are already identified as a key barrier to health care25,26.
The second ‘grand absentee’ among preferred specializations is internal medicine. This absence is partially consistent with previous reports suggesting that internal medicine ranks relatively low in perceived prestige among medical specialties27. Internists provide broadly applicable, integrative competencies and constitute a key workforce group in many non-tertiary and rural hospitals that must address diverse health needs with limited access to narrow subspecialty care. Internal medicine has historically supported holistic, patient-centered practice, which is increasingly important given population ageing, multimorbidity and the growing burden of chronic disease. The global challenge facing healthcare systems today is the increasing prevalence of non-communicable diseases and the growing number of older patients with chronic diseases and multimorbidity. In order to address this new epidemiological paradigm, a holistic approach is required, as well as an increase in the comprehensive care skills of subspecialists – aspects that internal medicine can provide. Gómez-Huelgas et al identified multidisciplinary medical teams as a response to fragmented care, arguing that internists are well placed to coordinate such teams28. This integrative role may be particularly valuable in peripheral areas, where access to narrow subspecialties is limited and a universal, comprehensive skill set can help mitigate the risk of medical deserts. The collected data, especially that related to family medicine and internal diseases, should not only raise concern but also constitute an important argument in favor of expanding research into factors influencing motivation to take up rarely selected specializations as well as into discouraging factors. Only a sufficiently nuanced understanding of these determinants will enable policymakers and educators to better manage early-career workforce flows so that under-resourced areas – understood here as both underserved specialties and rural/peripheral regions at risk of becoming medical deserts – attract well-prepared young physicians, rather than becoming a default option for those unable to obtain training positions in large metropolitan centers.
It appears that the motivators that drive young Poles to take up the medical profession are somewhere between the motivations most often declared by the students from highly developed countries (corresponding to the top of Maslow’s hierarchy of needs – self-development, self-actualization and a need for prestige) and those declared by students from developing countries (usually corresponding to the middle levels of the pyramid, such as job stability and prosperity)29. Moreover, the selection of a future place of work is influenced not only by the individual preferences of particular doctors but also by the state’s health policy, the dynamics of the medical job market as well as (or even most of all) private reasons including partner relationships or plans to have children. These factors change in time and are dependent upon life stage.
Current conditions in the job market such as the so-called ‘employee’s market’ (a situation in which ‘jobs are awaiting the doctors, who will find them anywhere’) may paradoxically lead to a situation in which the doctor will be that partner who will suit his/her workplace to the needs of the other spouse depending on the nature of their profession, for example related to rural or peripheral areas.
At the same time, students may not fully anticipate the practical consequences of workplace selection, such as differences in purchasing power between peripheral and metropolitan areas (eg housing costs), or the fact that some specializations can be easier to complete in smaller urban centers. For example, in the 2024 autumn recruitment, Poland’s capital offered no places in anesthesiology and intensive care, while Ciechanów (6000 inhabitants) offered as many as six30.
Finally, broader structural trends may further weaken the link between residence and workplace. Technological development can delocalize parts of specialist work: cardiologists and radiologists already interpret ECGs and imaging remotely, while telecare and specialist collaboration within coordinated care models are increasingly common. Improved transport infrastructure also brings peripheral areas closer to major urban centers, facilitating both patient mobility and physician commuting by reducing travel time.
The preferences of medical specialties need to be continually investigated to develop a set of incentives that encourage doctors to work in regions where they will be most needed in the future. This is particularly important for mitigating medical deserts. This approach is consistent with the recommendations resulting from European comparative analyses, which emphasise that focusing on undergraduate education and creating dedicated incentives for future doctors is one of the key methods of preventing medical deserts4.
Implications for practice and policy
Our findings offer policymakers valuable insights. From a system perspective, a few issues are particularly important. First, addressing medical deserts requires more targeted workforce planning within undergraduate and postgraduate medical education. Second, key strategies should focus on offering dedicated incentives for family medicine and other specialties experiencing shortages, creating rural and community-based training programs, and arranging clinical placements in underserved areas. In addition, adjusting medical curricula with population health needs and primary care competencies may improve preparedness and retention of medical doctors in rural and remote areas affected by workforce shortages. Concerning health policy, long-term national health workforce planning is needed, as is strengthened collaboration between medical universities and the Ministry of Health. Dedicated structural reforms are also required to make rural medical practice more attractive and sustainable.
Strengths and limitations
The current study had a pilot nature and draws attention to examining and monitoring factors and determinants of medical specialization choice. Its strengths include a relatively large sample size for a pilot investigation, the inclusion of students from three different years of medical study, and the use of an online survey platform that ensured respondent anonymity. However, this study is not free from limitations. First, it was conducted only within one university. The second is a low response rate (12%) and a high proportion of first-year students. Moreover potential non-response bias or characteristics peculiar to the capital city should also be mentioned. Forecasts of growing workforce deficits, particularly in areas at risk of becoming medical deserts, underscore the need for systematic surveillance of these trends and for targeted actions that can inform both undergraduate curricula and policies shaping specialty training pathways. This is why the presented findings should be regarded as preliminary and require further and more in-depth exploration.
Future research direction
Future research should include multicenter studies and comparisons across institutions in both urban and rural settings. A qualitative approach based on in-depth interviews with medical students and young physicians is also recommended to better capture contextual drivers and barriers. Additionally, a longitudinal follow-up study should be conducted to track how preferences evolve over the course of medical education and early postgraduate training.
Conclusion
The study findings indicate that medical students are mainly motivated by the prospect of job stability (average score 4.5), a desire to contribute to the world (average score 4.3) and the need for professional self-development (average score 4.1). The cohort is characterized by a relatively high socioeconomic status, with 82% of respondents describing their family affluence as high or very high and 91.6% having at least one parent with a higher education degree. In terms of geographic career plans, there was a strong preference for remaining in major urban centers, particularly Warsaw, which was selected by over 30% of the sample. In contrast, interest in rural medicine is minimal: only 13% of students originally from rural areas intend to return there, and a mere two respondents from urban backgrounds expressed a willingness to move to the countryside.
To address these disparities, policymakers should consider implementing targeted rural residency positions and financial incentive schemes, such as municipal scholarships or loan repayment programs, specifically for those who commit to working in underserved regions. Furthermore, curricular reforms that introduce mandatory rural clinical rotations could help familiarize students with non-metropolitan practice environments. The current findings reveal a clear preference for medical practice in major metropolitan centers, particularly Warsaw. At the same time, the expansion of telemedicine and professional mobility offers an opportunity to reduce the isolation of rural practice and increase its appeal to new graduates.
It must be noted that these findings are limited to a single university sample in Warsaw and, as such, may not be representative of the entire Polish medical student population. Considering these results, future research should focus on multicenter surveys to compare students from different regional backgrounds and longitudinal tracking to evaluate whether undergraduate intentions align with actual career paths after graduation. Additionally, qualitative studies are needed to explore the specific sociocultural and professional barriers that discourage students from choosing rural careers, providing a more detailed understanding of the factors influencing their geographic distribution.
Funding
This work was not supported by any funding.
Conflicts of interest
The authors report there are no competing interest to declare.
AI disclosure statement
No generative artificial intelligence tools were used in the screening, data extraction, or analysis processes. AI-assisted language tools were used solely for minor language refinement and editing support during manuscript preparation, with all intellectual content, analysis, and final decisions made by the authors.
References
You might also be interested in:
2013 - Advanced rural skills training: are recently qualified GPs using their procedural skills?