


Introduction
Risk assessment is a critical component of quality and safety management in any organization, and particularly so in health care1. Defining risk as any event that may jeopardize the achievement of organizational (or individual) objectives provides a structured framework to identify potential threats, analyze them based on the likelihood of occurrence and associated consequences, and determine the need for monitoring or mitigation measures2. Risk-based thinking, applicable across the management system, should extend to all dimensions of an organization, including strategic, operational, financial, and compliance domains, and must actively engage professionals at every level1,3.
Within this framework, healthcare professionals play a key role in identifying situations that may lead to errors, and in recognizing opportunities for prevention. This underscores the importance of leadership in promoting risk-awareness training and ensuring the necessary resources are available4. A professionals’ capacity to assess and judge the severity and acceptability of risks is shaped by a combination of factors, including knowledge, experience, values, attitudes, and emotions5. This highlights the critical role of risk-awareness training in shaping practices and behaviors that enhance the quality of care, while acknowledging the influence of professional role and contextual factors.
Although risk assessment is applicable (and should be applied) to all aspects of healthcare work, current literature reveals that many healthcare professionals tend to underestimate or overlook the various risks they encounter. Among these, biological risks are the most commonly recognized, while physical and psychosocial risks are often underperceived6. There remains a significant gap in the evidence base regarding how healthcare professionals working in emergency services in remote areas perceive and assess risks.
For the purposes of this review, ‘remote locations’ or ‘remote settings’ are defined as geographical areas or localities that, due to their distance from urban centers or from densely populated areas, are characterized by limited, difficult, or slow access to services, infrastructure, and sometimes even communication7-10. Geographic isolation and physical barriers can severely impact healthcare delivery, particularly in emergency situations involving accidents or sudden illness.
Delivering health care in remote emergency contexts is inherently complex and demands timely, effective, and well-coordinated responses to ensure access to appropriate care. In such settings, healthcare professionals’ perceptions of context-specific risks and operational challenges are critical to preventing adverse events and ensuring patient safety. These professionals must be prepared to navigate unpredictable scenarios and take proactive measures to safeguard both patient outcomes and their own wellbeing7,8.
The research questions this study aims to address are:
- What are the risk perceptions among healthcare professionals in remote emergency care concerning patients, themselves, and service delivery?
- How do these professionals manage and mitigate the risks identified in these settings?
Methods
Research design
A scoping review was selected as the appropriate review type, as this approach is effective for mapping knowledge on a topic that is not yet well understood. It is commonly used to identify knowledge gaps, clarify key concepts, and explore the scope or direction of ongoing research. Scoping reviews can also serve as a preliminary step for conducting a systematic review or for confirming the relevance of a particular research focus11,12.
In this study, the approach enables, for the first time, the synthesis of existing scientific evidence on the perception of risks associated with healthcare professionals’ practice in remote emergency settings.
Methodology
This study followed the JBI methodology for scoping reviews13,14, in accordance with the protocol previously published by the authors15. The literature search was conducted across six databases: Scopus, PubMed, LILACS, Cochrane, CINAHL, and Web of Science. These databases were selected to ensure a comprehensive retrieval of indexed literature, including sources from diverse geographical regions. No temporal limits were applied to the search, as, to the best of our knowledge, no prior review on this topic has been published that would justify restricting the time frame of this study.
Eligibility criteria
Following the Population, Concept, and Context (PCC) framework, inclusion criteria were defined for each component16. The population comprises healthcare professionals, the concept pertains to risk perception, and the context involves emergency care in remote locations. A detailed summary of the PCC criteria is available in the published scoping review protocol15.
Additional inclusion criteria were publications in English or Portuguese (enhancing the study's geographical and linguistic breadth) as well as observational studies, quantitative or qualitative research, and systematic reviews. The search was executed in December 2024.
Search strategy
Phase 1: Initial search and identification of best descriptors
The search strategy was initiated with a broad search in PubMed, analyzing titles, abstracts, and keywords to identify relevant terms, including MeSH (Medical Subject Headings). Using combinations like 'nurses and risk perception' in different contexts, the following MeSH terms were identified: 'Nurses*', 'Perception', 'Rural Population', 'Rural Health', 'Nursing*', 'Rural Nursing', 'Social Perception*', 'Community Nurses', 'Rural Areas', 'Rural Health Care', and 'Rural Communities.'
Additionally, several free terms not classified as MeSH were isolated, such as 'risk perception', 'perception of risk factors', 'geographically isolated', 'rurality', and 'rural and remote health-care'. A complementary search in Google Scholar using 'emergency nurses', 'risk assessment', and 'remote areas' also helped identify the term 'emergency preparedness'.
Phase 2: Identifying free terms in Portuguese and corresponding English terms
Next, we identified free terms in Portuguese and searched their equivalents in English in the DeCS (Health Sciences Descriptors) database for adequacy to the databases we intended to search15.
Phase 3: Combining identified expressions
Expression s identified in previous phases were compiled and cross-referenced with English descriptors from the DeCS database. A comprehensive search was then conducted in the MeSH database to determine whether each term or phrase qualified as a MeSH. Relevant definitions and associated entry terms were extracted accordingly. Free-text expressions (quoted and undefined) were also validated during this process15.
This synthesis aimed to streamline each dimension (population, concept, and context) for greater clarity and search efficiency. Common terms across expressions were consolidated using truncations (*). For instance, 'rural health', 'rural areas', and 'rural population' were unified under the keyword 'rural'. Similarly, terms such as 'nurse', 'nurses', and 'nursing' were consolidated using the truncation 'nurs', in line with database-specific search behaviors15.
For the emergency-related terminology, both 'emergency' and 'emergencies' were retained to avoid irrelevant results involving the term 'emergence', which is typically unrelated to the study’s focus. Within the concept dimension, expressions such as 'risk assessment' and 'risk management' were preserved as exact phrases to prevent misclassification with epidemiological or cost–benefit analyses. Quotation marks (' ') were used to maintain the integrity of multi-word s and prevent databases from retrieving orthographically similar but semantically unrelated terms. Additionally, emergency-related descriptors were contextualized to retrieve studies involving any category of healthcare professionals operating in remote emergency settings.
The resulting Boolean search phrase integrating the PCC dimensions was:
(("nurs*" OR "physician*" OR "paramedi*" OR "First responders" OR "First responder" OR "Advanced EMT" OR "Advanced EMTs" OR "EMT-Paramedic" OR "EMT-Paramedics" OR "medical technician*" OR "medicine Technician*") AND ("Risk perception" OR "Risk Assessment" OR "Risk Assessments" OR "Risk Analyses" OR "Risk Analysis" OR "Risk Behavior" OR "Risk Behaviors" OR "Risk Management" OR "Risks Management" OR "Safety Management" OR "Safety culture" OR "Safety Cultures" OR "Hazard Management" OR "Hazards Management" OR "Hazard Control" OR "Hazard Controls" OR "Hazard Surveillance" OR "Program Hazard Surveillance Programs" OR "Operational risk") AND (("rural" OR "remote" OR "isolated" OR "wilderness" OR "offshore") AND ("emergency" OR "emergencies")))
Study selection/source of evidence
As a preliminary step, the search strategy targeted titles, abstracts, and keywords. Minor adjustments were made in the application of truncations to refine the search results, which are summarized in Supplementary table 1.
A total of 410 records were retrieved and imported into the Rayyan bibliographic software. In the first phase, duplicate records (n=94) were identified and removed. The remaining 316 studies underwent a screening process conducted independently by two reviewers. Titles and abstracts were assessed according to the predefined inclusion and exclusion criteria. Studies published as clinical trials, conference proceedings, communications at scientific events, and those without available abstracts were excluded. This screening phase resulted in 76 studies selected for full-text review. In the subsequent phase, 50 studies were excluded due to insufficient methodological focus, irrelevance to the study objectives (eg drug prescription), or lack of emphasis on remote emergency care contexts. As a result, 26 articles were included in the final scoping review.
The study selection process is illustrated in the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews)13 flow diagram presented in Figure 1.
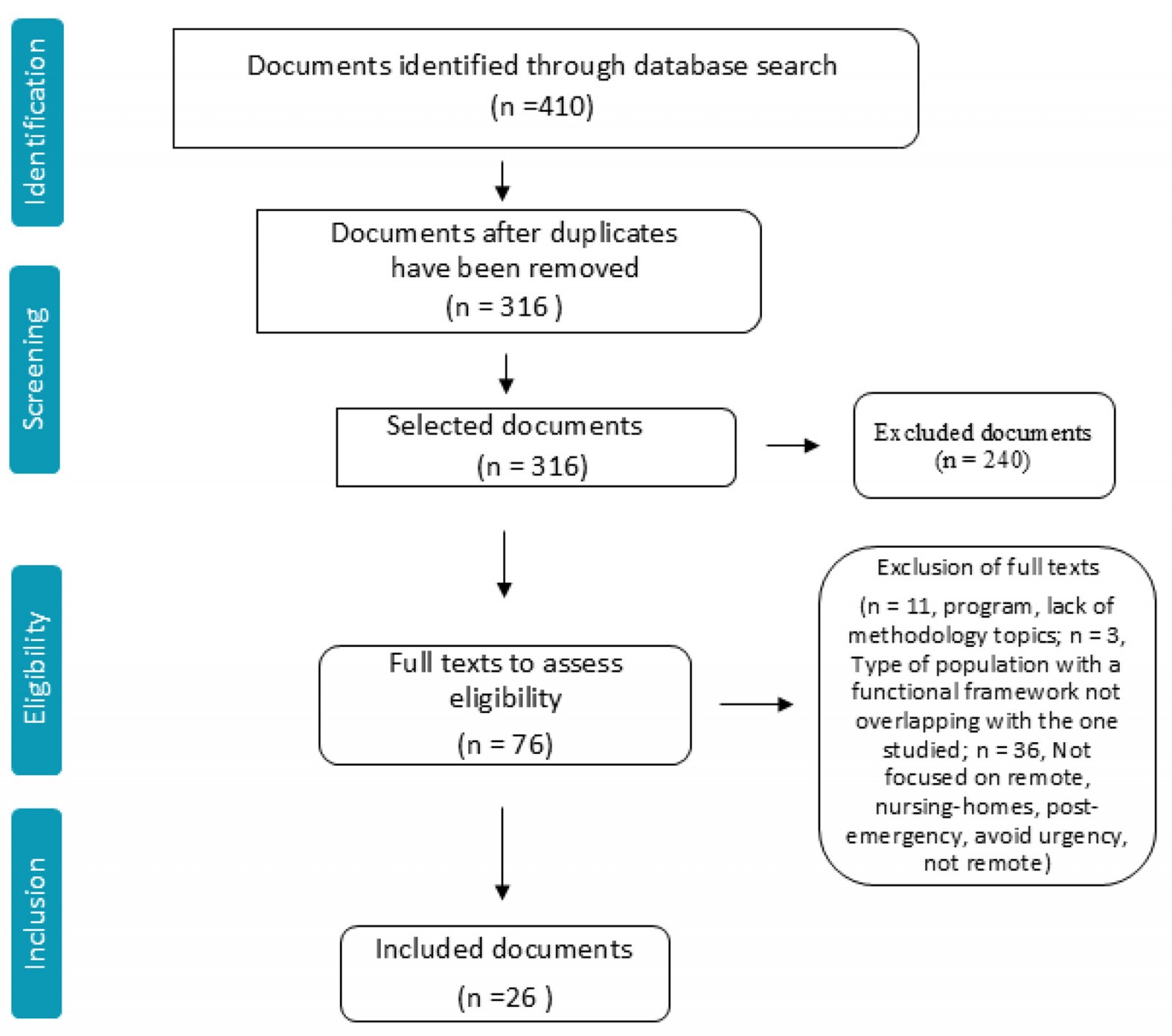 Figure 1: Flowchart of the scoping review process.
Figure 1: Flowchart of the scoping review process.
Ethics approval
Ethics approval was not required for this study, as it is a scoping review based solely on previously published evidence.
Results
A comprehensive analysis of the full-text articles was conducted. Data extraction focused on study objectives, population characteristics, explored concepts, contextual settings, study methods, and key conclusions relevant to the review question(s).
Initially, each reviewer independently read and analyzed the studies, completing the data extraction tool. Discrepancies and uncertainties regarding the inclusion of specific studies were subsequently resolved through discussion among the authors.
Data analysis and presentation
Table 1 summarizes the general characteristics of the 26 articles included and analyzed. The US and Australia emerged as the countries with the highest number of articles, with nine and eight respectively, suggesting a particular concentration of academic attention on emergency care challenges in remote settings within these geographies.
The objectives of these articles reflect a diverse array of concerns within emergency health care in rural and remote contexts. A majority of studies (n=18) addressed risks tied to professional and institutional competence. A smaller number focused on specific issues such as sexual abuse (n=1), safety culture (n=1), prevention of disease or accidents in the elderly (n=2), and occupational health (n=4).
Methodologically, the body of literature encompasses a broad spectrum of study types. Predominant among these are prospective, retrospective, and cross-sectional studies. These are complemented by qualitative inquiries, cohort and case studies, observational research, multimodal approaches, exploratory and descriptive studies, root cause analyses, and even ethnographic accounts, illustrating the methodological heterogeneity in examining risk in remote emergency care. Data collection tools were equally diverse, ranging from record reviews and standardized instruments to custom-developed questionnaires and in-depth interviews.
The temporal span of the studies, from 1994 to 2024, reveals an upward trend in scholarly output over time, with the most productive year being 2011 (n=4). Table 2 offers a synthesized overview of each article, highlighting the specific hazard or issue identified and linking the findings to the core review questions. A cross-cutting theme in the analysis is the ambiguity surrounding the term ‘remote settings’. Definitions fluctuate across studies, with some anchored in population metrics and others hinging on the absence of services and infrastructure. This lack of definitional consistency complicates comparisons and suggests an opportunity for conceptual clarification in future research.
Regarding the risk perceptions of healthcare professionals working in these settings, a complex tapestry emerges. Professionals voiced concerns about the safety of individuals affected by abuse and substance use; the vulnerability of elderly patients, particularly in the context of falls; and systemic risks such as delays in referrals, transportation hurdles, and knowledge gaps in triage and urgent care. Additionally, the emotional and physical toll of managing high-stakes emergencies in isolation was highlighted, including threats of aggression, difficulty standardizing practices, and impacts on their own health and social lives.
Importantly, healthcare professionals perceive themselves as frontline sentinels, a key role to identifying and flagging problems before they escalate. They articulate the crucial role of adequate training, infrastructure, and equitable distribution of resources to enable timely and appropriate responses. The geographic isolation intrinsic to many remote areas is seen not only as a logistical challenge but also as a determinant of clinical outcome.
Risk management strategies, as described across studies, vary markedly. In several instances, risk assessment is either underdeveloped or not explicitly addressed, which is often a reflection of structural limitations or the secondary positioning of risk in the study design. Where approaches do exist, they range from improvisational, context-specific tools to the application of formalized protocols. This variation underscores the absence of a standardized framework for risk identification and mitigation in rural emergency care.
In terms of professional scope, while nurses are the most frequently studied group (n=17), physicians (n=13), paramedics (n=7), and emergency technicians/firefighters (n=5) also feature prominently. Only two studies analyzed all four professions together, with most studies focusing on a single profession (n=13) or two (n=10), suggesting a missed opportunity to examine interprofessional dynamics and team-based risk navigation. Table 3 provides a detailed breakdown of professional focus across the studies.
Table 1: General characterization of articles
| Author(s) | Year | Country | Objective | Study type | Instrument(s) |
|---|---|---|---|---|---|
| Sutherland et al17 | 2013 | US | To describe abuse experiences, substance use patterns, and reproductive health among a sample of women seeking care in the emergency department | Cross-sectional | Questionnaire |
| Shah et al18 | 2006 | US | To assess whether emergency medical services providers could expand their role to include proactive screening for common health risks in older adults, specifically identifying individuals at risk for falls, influenza, and pneumococcal disease | Cohort | Questionnaire; telephone interview |
| Cairns et al19 | 2018 | Australia | To characterize button battery exposures in Australia, focusing on children. The study aimed to describe circumstances surrounding exposure, product details, battery specifics, and hospital management | Prospective observational | Record analysis |
| Flabouris20 | 2001 | Australia | To describe the utilization pattern of a patient transport service with medical team for patients with suspected isolated spinal injuries transported from hospital or incident scene | Retrospective | Record analysis |
| Waymack et al21 | 2015 | US | To compare rates of procedures and critical diagnoses in rural and metropolitan emergency departments | Retrospective | Record analysis |
| Luck et al22 | 2008 | Australia | To identify strategies emergency nurses use to prevent, reduce, and manage violence | Case | Interviews, observation; record analysis |
| Pannifex et al23 | 2013 | Australia | To enhance safety and reduce practice variation in paediatric sedation in emergency departments by implementing a standardized paediatric sedation program | Multimodal | Development of a clinical governance self-assessment checklist; record analysis |
| Cash et al24 | 2019 | US | To compare the distribution of cardiovascular health and its individual components between emergency medical technicians and paramedics. To identify associations between demographic and employment characteristics with ideal cardiovascular health in emergency services professionals | Cross-sectional | Questionnaire |
| Saner et al25 | 2013 | Switzerland | To examine the effects of a first responder-based system working concurrently with local hospital emergency medical services in a mixed urban–rural area | Prospective | Record analysis |
| Tompkins-Dobbs et al26 | 2011 | US | To investigate treatment practices and availability of policies and procedures in emergency departments of rural, suburban, and urban hospitals for patients addicted to methamphetamine | Case | Questionnaire; telephone interview |
| Rice et al27 | 2022 | Uganda | To evaluate the association between emergency medicine physician supervision and 3-day mortality in patients treated by non-physician clinicians in a task-sharing model of emergency care | Retrospective cohort | Record analysis |
| Kaczorowski et al28 | 2020 | Australia | To gain a broader perspective on how emergency nurses understand the term 'safety culture' and how this understanding influences their daily practice | Exploratory; descriptive | Semi-structured interview |
| McCarty et al29 | 2018 | US | To identify and implement an evidence-based fall risk assessment tool for use in Essentia Health emergency departments in a large predominantly rural healthcare delivery system | Prospective | Iowa Model; MEDFRAT Scale |
| Benson et al30 | 1994 | US | To define specific areas needing improvement in air transport | Cross-sectional | Record analysis |
| Husum et al31 | 2003 | Iraq and Cambodia | To explore the effect of low-cost pre-hospital trauma systems on trauma outcomes in landmine victims and study pre-hospital risk indicators for more effective screening of landmine-related injuries | Prospective | Record analysis |
| Fatovich et al32 | 2011 | Australia | To examine the effect of distance and isolation on severely injured patients transferred by the Royal Flying Doctor Service from rural and remote areas | Retrospective cohort | Record analysis |
| Endacott et al33 | 2006 | Australia | To examine strategies used by nurses to manage patients at risk of deterioration in small rural hospitals | Qualitative | Questionnaire adapted from previous research; interviews; observation |
| Kornelsen and Grzybowski34 | 2008 | Canada | To explore potential social effects on physicians arising from an unexpected adverse outcome | Qualitative | Interviews |
| Studnek and Ferketich35 | 2007 | US | To determine factors associated with seatbelt use among emergency medical services professionals | Cross-sectional | Questionnaire: National Registry of Emergency Medical Technicians |
| Turris et al36 | 2017 | Canada | To describe logistical challenges, disease/injury rates, medical attendance rates, and ambulance transport rates at a large-scale annual triathlon event in a remote location | Observational; prospective | Questionnaire; record analysis |
| Bardhan et al37 | 2023 | US | To determine the prevalence of psychosocial work stress among emergency medical services professionals working in rural and urban settings and whether work stress is associated with other risk factors in the population | Cross-sectional | Shortened version of the Effort–Reward Imbalance model in questionnaires |
| Mahmood et al38 | 2018 | Indonesia | To find the root cause of persistently high maternal mortality in a rural district of Indonesia | Root cause analysis | Clinical records |
| MacKinnon39 | 2011 | Canada | To explore the work of nurses in rural acute care hospitals, focusing on their safeguarding practices with patients | Ethnography | Observation; interviews |
| Wright et al40 | 2008 | Australia | To promote evidence-based stroke care practices in rural hospitals | Prospective, observational | Record analysis |
| Harris et al41 | 2011 | Scotland | To outline the skills and competencies needed for maternity care practice in rural areas | Qualitative | Interviews |
| Limprayoon et al42 | 2005 | Thailand | To evaluate and identify challenges encountered in the inter-hospital transport process of critically ill pediatric patients from remote hospitals to the pediatric intensive care unit | Retrospective | Record analysis |
Table 2: Responses to review questions: risk assessment and characterization
| Author(s), year | Identified hazard/issue | What are the risk perceptions among healthcare professionals in remote emergency care regarding patients, professionals themselves, and services? | How do these professionals manage and mitigate identified risks within these settings? |
|---|---|---|---|
| Sutherland et al, 201317 | Women seeking care in emergency services without a history of trauma or acute illness | Potential risks to the wellbeing and safety of individuals affected by abuse and substance use | Risk assessment and management through ad-hoc techniques (eg existing scales/questionnaires) |
| Shah et al, 200618 | Falls, contracting influenza, or pneumococcal disease | Potential risks of falls, influenza, or pneumococcal disease | Risk assessment and management through ad-hoc techniques (eg professionals created a questionnaire to apply to the target population) |
| Cairns et al, 201919 | Failure to identify a situation requiring urgent treatment | Lack of knowledge among professionals in identifying situations requiring urgent treatment | Risk assessment and management through established guidelines and protocols |
| Flabouris, 200120 | Aggravation of pre-existing injury due to choice of transportation | Potential risk of aggravating injury due to choice of transportation | Risk assessment and management through ad-hoc techniques (eg analysis of outcomes resulting from different modes of transportation) |
| Waymack et al, 201521 | Failure to perform a procedure due to lack of experience or no previous experience | Risk of being unable to perform critical procedures due to lack of experience or minimal prior exposure | Risk assessment and management was not performed due to lack of experience |
| Luck et al, 200922 | Being assaulted by patients, their families, or friends in the emergency department | Risk of being assaulted by patients, their families, or friends in the emergency department | Risk assessment or management was not part of the study objectives |
| Pannifex et al, 201323 | Not using the safest and consensus pediatric sedation technique for minor emergency procedures | Risk of pediatric sedation for minor emergency procedures due to lack of uniformity in sedation procedures | Risk assessment and management through ad-hoc techniques (eg nurses and other professionals defined an approach based on best practices, and developed a clinical audit tool to assess compliance with key quality and safety measures) |
| Cash et al, 201924 | Developing cardiovascular disease as an emergency medical professional | Risk of prevalent cardiovascular health risk factors among emergency healthcare professionals | Risk assessment and management was not performed due to limited access to resources |
| Saner et al, 201325 | Delay in applying an automated external defibrillator | Risk of death or severe neurological problems due to delayed intervention with an automated external defibrillator | Risk assessment or management was not part of the study objectives |
| Tompkins-Dobbs and Schiefelbein, 201126 | Lack of policies and procedures for referring methamphetamine-addicted patients | Potential risks associated with inadequate or inconsistent management of methamphetamine-addicted patients | Risk assessment and management was not performed due to lack of knowledge, procedures, and action policies in the institutions |
| Rice et al, 202227 | Mortality within the first 3 days in an emergency service without a specialist emergency physician present | Risk of assuming care for critically ill patients in emergencies without direct supervision from a specialist emergency physician | Risk assessment and management was based on a comprehensive evaluation of patient vital signs, clinical characteristics, disease severity, and statistical modelling techniques |
| Kaczorowski et al, 202028 | Absence of a safety culture | Level of understanding regarding safety culture | Risk assessment and management was not performed due to nurses’ perceived lack of support by managers |
| McCarty et al, 201829 | Falls in elderly patients | Risk of falls in elderly patients in the emergency department | Risk assessment and management was based on the Memorial Emergency Department Fall-Risk Assessment Tool (MEDFRAT) |
| Benson et al, 199430 | Non-location of the aircraft | Risk of not meeting all previously defined communication requirements (the risk of not having regular access to the aircraft's location) | Risk assessment or management was not part of the study objectives |
| Husum et al, 200331 | Lack of systematization in screening for landmine injuries | Risk of high mortality due to lack of a systematic screening tool following anti-personnel mine accidents | Risk assessment and management through ad-hoc techniques (eg professionals monitored the use of life-risk assessment tools tailored to anti-personnel mines and their effects) |
| Fatovich et al, 201132 | Distance and isolation of emergency rescue units | Risk of death from major trauma in remote and isolated areas | Risk assessment and management through ad-hoc techniques (eg nurses and other professionals correlated survival rates with air transport from remote areas to tertiary hospitals, considering trauma classification, remoteness index, time to initial approach, and subsequent transport duration) |
| Endacott and Westley, 200633 | Failure to anticipate deterioration of patients in resource-limited rural hospitals | Risks associated with failing to anticipate patient deterioration in resource-limited rural hospitals | Risk assessment and management through ad-hoc techniques (eg nurses conducted observations, interviews, and questionnaires) |
| Kornelsen and Grzybowski, 200834 | Unfavorable outcomes in emergency care practice in rural or remote settings | Social risk arising from healthcare outcomes | Risk assessment and management through nurses' and other professionals' perceptions |
| Studnek and Ferketich, 200735 | Non-use of seatbelts in emergency services | Risk of moving within the ambulance compartment without wearing seatbelts | Risk assessment and management was not performed due to organizational policies and individual-level variables |
| Turris et al, 201736 | Lack of assistance/resources in emergency care during triathlon events | Risk of injury or illness during mass sports events | Risk assessment and management was based on data from event characteristics, patient presentation rates, percentage of patients transferred by ambulance, hospital transfer rates, ambulance transfer rates, and medical consultation rates were collected |
| Bardhan and Byrd, 202337 | Psychosocial stress among emergency services professionals | Risks related to psychosocial stress among professionals working in emergency services | Risk assessment and management was not performed due to professionals' psychosocial work stress |
| Mahmood et al, 201838 | High maternal mortality | Risks associated with persistently high maternal mortality in rural districts | Risk assessment and management was not performed due to organizational practices, including reduced staff, lack of training and skills |
| MacKinnon, 201139 | Failure to recognize the specificity of nursing work in rural or remote environments | Risks threatening patient safety | Risk assessment and management through ad-hoc techniques (eg combination of practices such as anticipating problems and emergencies, Careful Watching and Surveillance, negotiating safety, mobilizing emergency systems) |
| Wright et al, 200840 | Non-adherence to best-practice recommendations for stroke treatment due to lack of awareness or organizational disorganization | Risk of not following stroke treatment guidelines due to lack of awareness or organizational disorganization | Risk assessment and management through the definition and measurement of key performance indicators, and their positive impact on performance |
| Harris et al, 201141 | Decision-making on the referral of parturients | Risk of referring a parturient to a specialized hospital | Risk assessment and management through ad-hoc techniques (eg nurses and other professionals In uncertain situations assess the risk based on knowledge of ambulance response times, prolonged transport durations, and weather conditions) Continuing multiprofessional professional development courses are effective in bringing teams together for training and updates |
| Limprayoon et al, 200542 | Failure to resolve issues arising from inter-hospital transport of critically ill pediatric patients | Risks of adverse events during the transfer of critically ill patients to the pediatric intensive care unit. | Risk assessment and management was not performed due to lack of experience and knowledge |
Table 3: Identification of studied professions
| Author(s), year | Nursing | Medicine | Paramedics | Emergency technicians/firefighters | Number of professional groups studied |
|---|---|---|---|---|---|
| Sutherland et al, 201317 | X | 1 | |||
| Shah et al, 200618 | X | 1 | |||
| Cairns et al, 201919 | X | 1 | |||
| Flabouris, 200120 | X | X | 2 | ||
| Waymack et al, 201521 | X | 1 | |||
| Luck et al, 200922 | X | 1 | |||
| Pannifex et al, 201323 | X | X | 2 | ||
| Cash et al, 201924 | X | X | 2 | ||
| Saner et al, 201325 | X | X | X | X | 4 |
| Tompkins-Dobbs and Schiefelbein, 201126 | X | 1 | |||
| Rice et al, 202227 | X | X | 2 | ||
| Kaczorowski et al, 202028 | X | 1 | |||
| McCarty et al, 201829 | X | 1 | |||
| Benson et al, 199430 | X | 1 | |||
| Husum et al, 200331 | X | 1 | |||
| Fatovich et al, 201132 | X | X | 2 | ||
| Endacott and Westley, 200633 | X | 1 | |||
| Kornelsen and Grzybowski, 200834 | X | X | 2 | ||
| Studnek and Ferketich, 200735 | X | 1 | |||
| Turris et al, 201736 | X | X | 2 | ||
| Bardhan and Byrd, 202337 | X | X | 2 | ||
| Mahmood et al, 201838 | X | X | 2 | ||
| MacKinnon, 201139 | X | 1 | |||
| Wright et al, 200840 | X | 1 | |||
| Harris et al, 201141 | X | X | X | X | 4 |
| Limprayoon et al, 200542 | X | X | 2 |
Discussion
In terms of approaches to risk, the reviewed literature can be grouped into three main categories. The majority of the 26 articles focus on risks directly associated with professional competence or institutional factors such as limitations in clinical decision-making, inadequate protocols, and systemic shortcomings. A second cluster of studies centers on occupational risks, addressing concerns like work-related stress, fatigue, and exposure to aggression. A smaller subset adopts a broader perspective, framing risk within the context of safety culture, emphasizing organizational attitudes, communication dynamics, and collective responsibility for minimizing harm.
Professional competence and institutional organization
Several articles highlight hazards associated with professional competence and institutional organization, including knowledge level, technical experience, transportation and infrastructure conditions, resource distribution and management, and procedural aspects, among others. Given the specificity of rural or remote settings, most authors suggested that there should be a specific preparatory component for integrating professionals who intend to work in this context33. The quality of initial training in emergency situations is crucial25. Extending training to non-professional groups is recommended as a measure to increase the probability of early and appropriate interventions19,27. Rural or remote areas are also characterized by a lower volume of attendances, reducing the diversity of clinical situations27. Another characteristic of these settings is the lack of specialized emergency professionals or the presence of professionals with little experience in less frequent procedures, as illustrated by the case of resuscitation25,33,38,42. Isolation associated with low-quality care has severe implications for the prognosis, particularly in major traumas32. The authors often argued on the need to mobilize professionals to consolidate practices in more specialized settings21.
The distance from urban centers and lower population density are also critical for situations requiring evacuation of victims17. A successful evacuation requires careful consideration and planning, taking into account the risk of deterioration in victim health and other factors that may influence outcomes, such as sudden weather changes that prevent safe evacuation or the unavailability of ambulances20,41. Also to be taken into account are constraints faced in remote settings, such as the distance to a referral hospital, the time an ambulance takes to arrive, availability of ambulances, prolonged transport durations, and weather conditions. This reality also implies managing criticism from colleagues in urban hospitals who receive the patients41. It is considered essential to invest in training professionals to accompany critically ill patients during potentially long transports. Adverse events can occur, such as extubation or obstruction of the endotracheal tube, among other challenges in maintaining patient stability42.
Rural and remote settings require stronger partnerships. Professionals can and should play the role of agents of change and promote concerted actions involving institutions and communities36. Due to certain events, it is important to align with the industry on ways to prevent accidents, such as ingestion of button batteries by children19.
In cases of war or conflict, rebuilding in remote areas takes a long time, and these areas often have few or no resources. In such contexts, support tools that aid in appropriate triage to save the most victims are essential31.
Emergency services can also represent an avenue for education and health promotion29. For example, elderly people are alerted to and monitored by health professionals about daily risks such as falls18.
Occupational problems
Some articles discussed risks and events related to occupational issues, including the risk of violence (assault by patients, their family members, or acquaintances), exposure to diseases, and social isolation resulting from stress caused by adverse outcomes. Violence issues are associated with various factors such as communication skills, availability of security, and architectural issues of the buildings where emergency care is provided22. Perception of risk in the occupational field relates working and salary conditions to the cardiac health of emergency professionals24. The effort–reward relationship is also pointed out as a source of stress and negative health outcomes when professionals perceive that their efforts significantly outweigh the rewards37. Furthermore, working in demanding isolation conditions, away from other colleagues and support services, can amplify stress due to the underlying belief that if a poor outcome occurs (eg death of a mother or baby), there could be significant social consequences, including the need to leave the community34.
Safety culture
A few of the analyzed articles addressed how safety culture is valued by professionals working in these contexts28. Professionals recognize that safety aspects are a collective effort shared by all team members and working conditions, notwithstanding they claim lack of time to communicate these failures. Even when communicated, proper attention is not always given by those responsible. Studies point to a mismatch between professionals who provide care and those who manage it, regarding priorities and responsibilities28,35.
Enhancing safety can also be achieved by uniformizing procedures, which involves finding an approach based on best practices39. By standardizing procedures, organizations can ensure that safety protocols are consistently followed, reducing variability and minimizing the risk of errors23,26,30,40.
Limitations
The following limitations should be acknowledged. The lack of a standardized definition of ‘remote settings’ across the included studies introduces variability that complicates comparisons and synthesis, as the term is often applied according to local interpretations rather than objective criteria. Additionally, while the inclusion of English and Portuguese publications broadens linguistic and regional representation, relevant studies in other languages or indexed in non-searched regional databases may have been missed. The review also found that most studies examined professional categories in isolation, limiting insight into interprofessional dynamics and team-based approaches to risk perception and mitigation. Finally, consistent with the nature of scoping reviews, no formal quality assessment of the included studies was undertaken, meaning that the findings should be viewed as exploratory and indicative of key gaps rather than as conclusive evidence.
Conclusion
Risk assessment, in the literature analyzed in this review, emerges as a series of processes requiring improvement, encompassing triage potential, initial clinical approach, case referral/transfer, occupational safety, and the quality of procedures and infrastructure. However, this scoping review also underscores the scarcity of studies linking healthcare professionals to risk perception and emergency care in rural/remote contexts. Furthermore, we observe that the analyzed papers tend to focus on isolated aspects identified by researchers, rather than considering the comprehensive context that contributes to their occurrence and resolution. Even those that were analyzed did not follow probability and consequence criteria but rather ad-hoc techniques associated with clinical evaluation and clinical decision-making.
The low number of articles found indicates that there is a need for further studies of risk analysis for emergency services in remote areas. These should include robust measurements of the probability and consequences of risks, alongside with corresponding mitigation strategies. Importantly, future research should also focus on the development of actionable frameworks to guide evidence-based improvements in emergency services. Such frameworks must consider the specific challenges posed by rural and remote settings, including the distribution of healthcare professionals, diagnostic and treatment resources, transportation, training, and referral systems to urban centers.
Future studies should address the limited interprofessional insights identified in this review, which reflect both the dominance of single-profession studies and, in many cases, the siloed way in which emergency care is delivered. Research adopting comprehensive, team-based, and system-level perspectives is needed to better understand the complex interactions and collaborative processes required for effective emergency care in rural and remote contexts.
Funding
The publication is supported by Fundação para a Ciência e a Tecnologia for funds to GHTM – UID/04413/2020 and LA-REAL-LA/P/0117/2020.
Conflicts of interest
There are no conflicts of interest in this study.
References
Supplementary material is available on the live site https://www.rrh.org.au/journal/article/9911/#supplementary