


full article:
Introduction
In Australia, people are living through an unprecedented economic crisis generated by an amalgamation of events, including international pandemics, the Ukraine invasion, extreme weather events (flooding and bushfires) and stagnant wages. In the media, cost of living, labour force participation, food and housing security are commonly reported as crunch points where Australian households either have to find additional income to cover these rising expenses, or decide to go without necessities for financial survival1. A commonly reported finance saving technique used by Australian families is to delay or avoid medical care and treatment such as appointments and filling prescriptions1,2. Australian households in outer regional to very remote areas are particularly burdened by well-documented barriers in accessing affordable and equitable health care due to Australia’s largely urban-centred healthcare system1,2.
These burdens include out-of-pocket healthcare expenditure (OOPHE) for gaps in medical costs, and associated additional expenses such as travel, medication, equipment, accommodation and time off work, which are not covered by Medicare, private health insurance or other government initiatives1,2. As a result, OOPHE is a significant risk factor for developing or exacerbating existing chronic and complex conditions2,3. It has been associated with negative health outcomes and even death as a result of delaying or avoiding treatment, with one in four Australians forgoing medical treatment due to OOPHE2-4. From 2019 to 2020, OOPHE created a $30 billion economic burden5, with the most marginalised communities in Australia being inequitably impacted2. The most recent Senate inquiry on out-of-pocket costs identified Aboriginal communities as one of the most vulnerable communities impacted by OOPHE2, with Aboriginal Community Controlled Health Organisations (ACCHOs) reporting patients choosing to defer appointments with GPs due to costs2, and some chronic kidney disease patients forgoing dialysis, resulting in death3. Rural residency and reduced employment capacity are factors associated with increasing OOPHE for Aboriginal families, and are identified as needing targeted support strategies1,2. However, these strategies require co-created health knowledge to provide a comprehensive understanding of risk and protective factors of OOPHE for Aboriginal families. This article explores the experiences and understandings of OOPHE with Aboriginal patients and families residing in the Far West of South Australia.
Methods
Design
Western constructs dominate OOPHE knowledge and experience in Australia. To reorientate this power imbalance and focus on relationality of OOPHE for Aboriginal people in the Far West of SA, knowledge interface methodology was engaged by the research team for the overall project design1. This started with the research team being led by Aboriginal researcher CR, and in ensuring over half of the investigative team were Aboriginal and/or Torres Strait Islander researchers or community leaders (SD, PS, TM, JC, KBB and DC), some of whom are from or have kinship ties to the Far West of SA. Non-Indigenous researchers in the research team (NK, EG, SU and JS) did not have senior research roles and focused on providing research support. These processes were essential in ensuring that Indigenous knowledges (knowing, being and doing) were privileged at the research interface.
In ensuring relationality of OOPHE at the interface the research team employed methods of yarning (a data collection method for rich data collection), no assumptions (an approach to diminish deficit framing) and being on Country (connection as defined by the participant)6,7. This approach was supported by a yarning guide developed by Aboriginal and Torres Strait Islander investigators, and based on previous research by CR, TM and JC1,8. All OOPHE yarns, which included a yarning consent process, were conducted by Kokotha researcher SD with kinship ties to the Far West. Yarns were audio-recorded and transcribed, with freehand notetaking used as an option for participants who did not wish to be recorded.
Recruitment
The Far West in South Australia is identified as a very remote (Monash Model (MM) 7) region9 encompassing Kokatha, Mirning and Wirangu Country. The study was approved by the Far West Community Partnerships (FWCP) Leadership Group, which has Aboriginal representation from across the townships of Ceduna, Koonibba, Scotdesco, Yalata and Oak Valley. Participant recruitment was facilitated by Community Leader PS at the FWCP in Ceduna. This approach, built on pre-existing relationships, ensured correct Far West cultural protocols were followed, and provided diversity of participant recruitment. Inclusion criteria required participants to be aged more than 18 years and have lived experience of OOPHE, defined as being a carer or patient who needed to travel for regular treatment and/or follow-up of an injury, or chronic or complex health condition. Participants who consented to participate were scheduled to have a one-on-one, in-person yarning session with an Aboriginal research assistant. All yarning sessions occurred on Far West Country in a location selected by the participant. Participants received a $30 honorarium for their time to participate in the session.
Analysis
Qualitative analysis software NVivo v12 (Lumivero; https://lumivero.com/products/nvivo) was used to facilitate the thematic coding of de-identified, transcribed (audio-recorded or freehand) sessions by two Aboriginal members of the research team (CR and SD). This process was initiated with deep listening of recordings by SD, with documentation of contextual points that would not be appreciated in transcripts (eg pauses, participant tone, local language). Following this, both researchers thematically coded transcripts individually. Throughout the analysis process both met regularly, undertaking reflective yarning together for theme development in the context of audio-recordings and transcripts. The collaborative process between CR and SD was essential for Far West OOPHE relationality, focused on contextualisation of local language and knowledge to describe OOPHE concepts in the context of family, culture and Country10.
Findings from the early reflective yarns were provided to participants through infographics distributed through Far West Community Partnership networks. Data and outcomes of the OOPHE project were provided back to knowledge custodians, the Far West Community Partnerships, as a process of Indigenous knowledge repatriation.
Ethics approval
Ethics approval was given through the Aboriginal Health Research Ethics Committee in South Australia (reference no. 04-21-920) and Flinders University Human Research Ethics Committee (reference no. 4434).
Results
A total of seven yarning sessions were conducted: four sessions consisted of one participant and the other three sessions had two participants (10 participants in total). All participants were aged more than 18 years, with six female and four male participants. Data were arranged into themes and subthemes, as outlined in Table 1 with illustrative quotes.
Table 1: Themes and subthemes of out-of-pocket healthcare expenditure in Aboriginal families from remote regions accessing health care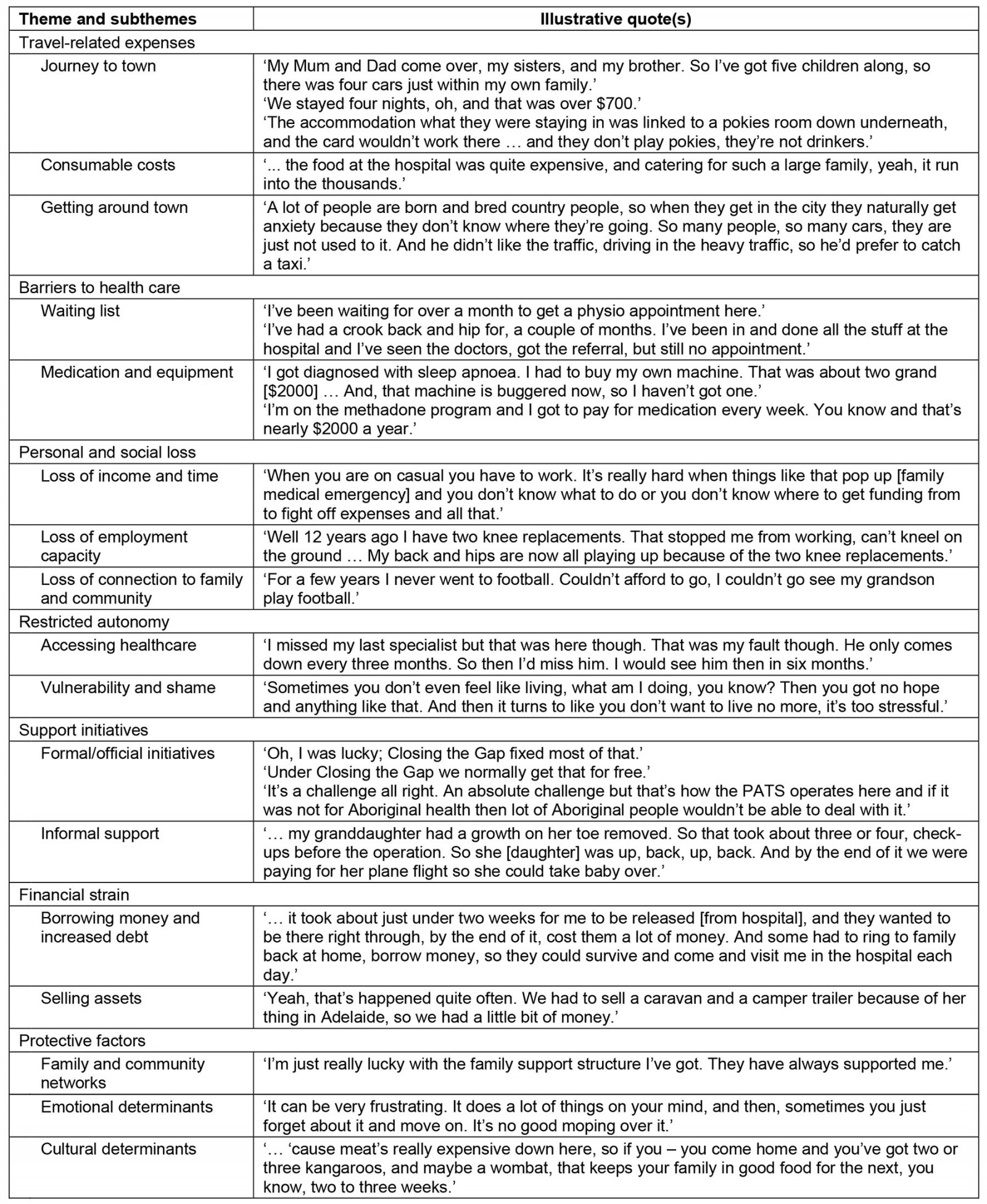
Travel-related expenses
The main theme arising from participant yarns was the various ways in which travelling to access health care incurred travel-related expenses, across a range of healthcare situations – from chronic and complex conditions and paediatric outpatient appointments through to addiction recovery. This theme comprised three subthemes, which related to the costs associated with the journey to a major urban centre to access healthcare appointments, consumable costs while away from home and getting around in an unfamiliar urban location. These subthemes are explored in more detail below.
Journey to town: The journey from the participant’s home to ‘town’ (a term used interchangeably to refer to the South Australian capital city of Adelaide) was identified as a significant cost for participants. Participants who travelled using their own vehicle especially spoke about the costs of fuel and maintenance when using their own vehicles for these journeys:
Our fuel bill was $260 in the Commodore ... I’d come back nearly empty.
The last five years we probably had, oh, a dozen, 15 trips to town … I’ve murdered a set of tyres.
Many participants stated that, when a family member was critically ill, members of the extended family would travel to town to provide additional support, which added to the increased fuel and vehicle costs. In addition to the associated transport costs were accommodation costs. Families who did not have family or friends to stay with in town had to fund the additional accommodation.
For those families who received welfare payments through the Australian Government’s income management systems, such as the Cashless Debit Card (CDC – such as Indue or BasicsCard), travel to town was particularly problematic. The CDC system restricts 50–80% of recipient’s welfare payment to household items11, which was a significant barrier for participants accessing affordable accommodation. For some families, the costs associated with travelling to a major urban area to receive health care could be thousands of dollars for just one trip, as described by one participant:
Normally around the $2000 mark, what it costs to go from here to town and return with meals, accommodation, fuel and that’s not eating in fancy restaurants.
Consumable costs: Purchasing food while in town for healthcare appointments was a significant expense reported by all participants. The cost of purchasing food from hospital kiosks or cafes was a particular concern.
To reduce the need to purchase food, many participants discussed self-catering as a key method to keep expenses down, with one participant providing an example:
… I used to do was put a half a dozen eggs in the eskys … Put the eggs in there and the bread and the butter and the bacon and the vegetables …
Emergency air retrieval (Royal Flying Doctor Service) was identified as being particularly impactful on consumable costs due to luggage restrictions. As reported by one participant traveling with their toddler, they had to contact family members in town to purchase all their consumables (eg nappies, formula, toiletries) while they were in hospital, as these items were not able to be accommodated in the restricted luggage allowance.
Getting around town: Anxiety and fear about city navigation to and from medical appointments was reported by many participants. As a result, participants reported using taxis to decrease the burden of being in unfamiliar surrounds, a solution that created additional out-of-pocket costs:
… He doesn’t know Adelaide, so he automatically gets anxiety because he’s scared he’s going to get lost. So he likes to catch a taxi, so he knows he’s going to the right place, which is another expense.
Barriers to health care
Many barriers were faced by participants when trying to access health care. Most notably, long waiting times were reported, particularly when trying to access general dental and allied health in the region. For some participants the wait time was too long, and sometimes these participants opted to travel and pay extra to access health care more quickly. As one participant expressed:
We’re going to have to pay extra money to go to Streaky Bay and that’s, ah, probably about seven visits to get the whole [dental] job done.
In addition to lengthy waiting times, all participants reported high medication costs as a significant barrier to their health care. These costs were despite medication costs being reduced by Australian Government subsidies and additional medication cost reductions, particularly for low-income earners and people with chronic or complex conditions. Equipment costs were also identified as substantial, with one participant not replacing or repairing a medical device after it broke.
Personal and social loss
Participants reported three ways their health care caused personal and social loss: loss of income and time, loss of employment capacity, and loss of connection to family and community.
Loss of income and time: Participants who were parents or patient carers reported loss of time and income through needing to travel and attend appointments with family. This particularly impacted on participants who owned their own business or worked on a casual basis, as they did not have access to the same leave entitlements as individuals employed full-time. However, one participant who did work full-time estimated a loss of $3500 in income, due to needing to take 5 weeks leave without pay to be in the closest major city (Adelaide, over 780 km away) while their child received treatment.
Loss of employment capacity: Participants also spoke about their loss of employment capacity, with many having to take time away from the labour force to care for family. The additional implication of this loss of employment capacity is the compounding loss of household income, as described by one participant:
I tried ... I couldn't work with my son not well, like that … I became his carer … Full time carer.
Loss of connection to family and community: The loss of connection with family and community caused many participants to experience social isolation. For some participants, this loss was far reaching and impacted their social relationships. One participant explained how the financial impacts of their health care contributed to this loss of connection with family:
You couldn’t afford to go to family barbeques because you didn’t have any excess food to be able to put on the table.
Restricted autonomy
Participants discussed how OOPHE restricted their autonomy in two separate ways: accessing health care, and their ability to maintain relationships, which created vulnerability and shame.
Accessing health care: Participants discussed how needing to travel to access health care restricted their autonomy, particularly their autonomy to make healthcare decisions. Some participants reported that travel to access health care was not always possible. These individuals were left with no choice but to not attend or cancel medical appointments as they could not afford or did not have funds available to travel for health. The effect of being unable to attend appointments is the inability to maintain control over one’s health and health care. As one participant stated:
So sometimes we end up just cancelling it [medical appointments]. And, uh, letting our health get worse, which is not great.
Vulnerability and shame: Restricted autonomy also impacted participants’ ability to maintain interpersonal relationships and participate in the social aspects of their lives. Participants spoke of the embarrassment and shame they felt when having to approach family or friends to borrow money for healthcare expenses. As one participant stated:
I’ve had to borrow money though, just to get by and pay it back, that’s embarrassing.
This embarrassment and shame, as experienced by some participants, has the potential to have lasting impacts on interpersonal relationships with family, friends and community. In addition to these feelings and the effect on their autonomy, the impact of having to travel to access health care also resulted in some participants being socially vulnerable. As an example, one participant spoke of having to place themselves in precarious situations because they did not have accommodation while in the city.
You know, I've done that before and I've stayed in the parklands there … A lot of other people have been doing the same thing … they've got nowhere to stay and they're just wandering around all night and haven't had any sleep.
Support initiatives
Access to support for travel through fuel vouchers, airfares or accommodation from Aboriginal community organisations, such as Land Councils administering Native Title, was reported by some participants. Participants also reported support from Australian Government initiatives such as the Closing the Gap co-payment program for the Pharmaceutical Benefits Scheme (PBS) for Aboriginal individuals with or at risk of a chronic disease, reducing the cost of PBS medication. Additionally in Australia rural and remote patients can also access government initiatives such as the Patient Assistance Transport Scheme (PATS). The PATS program provides travel subsidies for patients who need to travel more than 100 km to seek specialist care that is not available in their region12. The participants in the present study commented on the complex nature of accessing initiatives of this type. Frustration was also evident in how these initiatives function; for instance, PATS provides reimbursement after travel and requires participants to document their travel journey and keep receipts, which for many was a barrier – as described by one participant:
She could get a small reimbursement off, PATS when she got back, but it was actually the money, what she needed, to go in the first place.
Financial strain
Long-term financial strain was discussed, and was particularly evident for participants who were already on very tight budgets, were on government support payments (eg Centrelink carers pension, pension) or were single-income households. Participants spoke of how large or repeated travel-related healthcare costs frequently left them with little or no money to spend on their arrival in the city. As one participant said:
I had to pay that out of my own pocket. That left me with nothing. That left me, when I got to town, that left me with actually nothing at all.
Actions undertaken by participants during these periods included borrowing money from family, taking out loans, reaching credit card limits or delaying bill payments. It was not uncommon for participants to sell assets to get by, especially those who were on government income management, as described by one participant:
So, she sold her vehicle and she used that [money] to assist her to take their baby up and down to town … She’s still recovering [financially] now from that. Like she hasn’t been able to replace the vehicle.
Protective factors
While participants primarily discussed the negative impacts of travelling to access health care, they also resolutely spoke about the social and cultural factors that provided protection. These factors were family and community networks, the cultural determinants of health and wellbeing, and Indigenous knowledges.
Family and community networks: Family for many was a source of strength and support, with some speaking of the resilience of large families; however, for some individuals this type of support was not an option.
We’re a big, strong family, and so we can offer financial assistance as we need it. But some families haven’t got that, and they really struggle.
Additionally, ride sharing with friends and family to town was another way to save on travel costs associated with medical care.
We, ask how much you've got … say if you've got three people. You know, $20 each. That's $60 which is good enough for drinks and food [when travelling to town for medical appointments].
Social, cultural and emotional determinants: Participant reflections included reference to protective factors from social, cultural and emotional determinants of Aboriginal health, even in the wake of significant emotional strain:
Aboriginal people usually manage to get by, but, uh … not easily. And it does cause,%u202Fit causes [a] tremendous amount of emotional pain.
Protective factors of self-efficacy, adaptability and autonomy were evident, with participants reporting on alternative ways to bring in some extra income to their household to cover medical costs, from art (painting, carving, or weaving), through to recycling.
I collect cans and bottles. Yeah, during the football season I walk around a couple of the ovals and pick up cans off the ground. You might get $10 here and $10 there. But in the end it helps a bit.
Cultural determinants through connection and practice were also protective for participants, for example as sources of local food for households to assist in decreasing costs.
If you haven’t got money, we’re lucky enough that we live on the coast, and we’ve got a lot of seafood on tap, so I know a lot of family groups will go down and they’ll fish and they’ll squid … they’ll get enough to last them for a couple of days.
Discussion
This is the first study to demonstrate the extensive impact of OOPHE on Aboriginal families living in the Far West of South Australia. Our findings indicate that remote Aboriginal households experience significant OOPHE when accessing medical care and treatment, especially when travel is required to access services. Accommodation, vehicle maintenance (fuel, tyres), parking fees and consumables were OOPHE reported by all participants, and are similar to the findings of studies with non-Indigenous populations13,14. However, previously unidentified in other studies was the cost of taxis to travel in and around town for appointments due to participants’ fear of becoming lost in an unfamiliar location by using public transport. Our participants reported their OOPHE spending to be well into the thousands of dollars, especially when needing to travel regularly for appointments. Excessive OOPHE has been previously reported by Aboriginal families impacted by burns injuries1, and by non-Aboriginal patients – especially those from rural regions in Australia15,16. However, this study highlights the breadth and depth of OOPHE spending for a range of healthcare requirements by remote Aboriginal families.
While some patients were able to access financial assistance through government initiatives, such as PATS, these supports were only accessible through reimbursement, which covered only a fraction of their total costs, which left many financially out of pocket. Due to increases in the costs of fuel and daily living, in 2022 PATS announced an increase in their fuel subsidy from 16 cent to 32 cents per kilometre starting in 2023, which provides some relief for families17. No other changes to the scheme have been announced, despite it being reported as too complicated for patients12,18,19; government inquiries and reviews have recommended greater clarity, support and ease of access, especially for Aboriginal families12,18,19. This study’s findings add to the call for reforms to alleviate financial strain through partial upfront payments or vouchers for accommodation and fuel. Additionally, extra family members should be considered under PATS across a variety of situations. Our participants reported that several family members were essential for health and healing while in hospital, but this came at a significant cost burden, with PATS only covering one escort for certain health conditions and none for air retrieval or obstetrics, with many Aboriginal women having to birth alone off Country without their partners or children12,18-20.
Financial hardship was evident and comparable to previous research with Australian patients2-4,21-23, with participants cancelling or not attending medical appointments to save money, resulting in worsening of their health condition. Participants were also obliged to place themselves in precarious situations to cut expenses, such as sleeping rough on the streets or parklands, with the increased risk of homelessness24. Vulnerability and trauma are significant risks of sleeping rough, from weather exposure (eg heatwaves and dehydration) and illness impacts (eg medication stolen) to sexual and physical assault, which in turn exacerbate illness for already sick people24. Relocating for medical treatment and limited access to safe and affordable accommodation proximate to healthcare facilities were additional factors identified that place Aboriginal individuals at higher risk of homelessness20,24. In some cases, Aboriginal patients found themselves ‘stuck’ off Country and away from family, with no alternatives; this has resulted in long-term homelessness, negatively impacting the individual as well as their family back home24,25. Radical change is needed to ensure that this is not considered an acceptable alternative for Aboriginal patients. Safe and appropriate accommodation options are required alongside integrated multidisciplinary approaches to care for Aboriginal patients traveling to the city for treatment and home again12,18,19. Examples of these approaches already exist but require greater liaison and oversight by tertiary services beyond patient discharge; the Safer Pathways program is an example of one such program for Aboriginal children with a burns injury.
The CDC system placed unnecessary restrictions and additional burden on participants. The CDC program prohibits purchase of items from businesses that sell alcohol or gambling products, including onsite accommodation or meals11, an extra burden for families already experiencing financial hardship and trying to make ends meet below the poverty line11. It increased the impact of OOPHE to catastrophic levels, evident through alternatives taken by study participants, such as the sale of significant personal assets (vehicle), which – although providing immediate relief – was frequently associated with long-term negative consequences. During this study, CDC was discontinued in South Australia, as long-term evaluations were poor26-28, and key recommendations had not been implemented such as co-designed financial literacy programs to enhance usage of the CDC card at facilities27,29.
Resilience of Aboriginal families and family support were identified as OOPHE protective factors. This theme was similar to past reporting in Aboriginal families who were impacted by burns injuries, with examples including financial assistance and caring roles1. This theme was, however, characteristic of large families, and therefore not available to all individuals. Even with family support, participants experienced feelings of shame and embarrassment associated with needing to borrow money from family to access health care. This is likely to decrease health and wellbeing further, with financial stress being strongly associated with psychological distress and poor physical health29,30. Not previously reported were the additional emotional, social and cultural protective factors that people obtained through connection and cultural practice, such as accessing locally sourced foods – whether traditional (eg kangaroo, seafood, quandong) or from local producers (eg sheep). These were an important and cost-effective way of feeding the family, especially after significant OOPHE from travel to the city reduced household budgets. This option was not necessarily available to all participants, however, as local foods were only seasonally available and often required extensive travel to source.
A strength of this study was the use of Indigenous research methods, which provided new insights and better understanding of OOPHE for Aboriginal households. Outcomes from this work will be communicated back to the Far West community and used to develop an OOPHE survey tool. We note this study focused on examining the OOPHE for Aboriginal people in the Far West of South Australia, therefore some results will be applicable to other Aboriginal and Torres Strait Islander communities in Australia as well as some First Nations communities internationally. It is likely that implications exist between our results at an international level; for example, in British Columbia significant OOPHE inequities exist between rural and urban patients, with a small amount of system-level support for travel being through the British Columbia Travel Assistance Program or the First Nations Health Authority31. In Aotearoa New Zealand, Māori patients in rural regions face significant inequities for treatment of chronic kidney disease, with many having to make the decision to move off Homelands for treatment or go for treatment32. This article adds to the international narrative and examination of OOPHE for First Nations people, and to calls for action for more appropriately designed policy and support programs.
Conclusion
Aboriginal families in the Far West of South Australia are significantly impacted financially when accessing health care through OOPHE, especially when needing to travel to major cities or regional centres for treatment. Government initiatives designed to provide financial assistance to access health care were not always easily available to Aboriginal families, and in some cases increased the financial burden to catastrophic levels, with participants resorting to drastic options such as selling personal assets, not attending medical appointments or sleeping rough. This highlights the need for reform of government initiatives to support remote Aboriginal families accessing health services. Cultural and family connections were protective factors, mitigating OOPHE burden – which in turn decreased anxiety and stress for Aboriginal families. This study provides insights into the level of complexities of OOPHE impacting Aboriginal families and argues for further work to establish appropriate definitions and measurements of OOPHE.
Acknowledgements
We wish to acknowledge all Aboriginal countries that this research was created over: Kaurna, Kokatha, Mirning, Wirangu, Ngarrindjeri, Arrernte and Eora. We pay respect to Elders past present and emerging. Sovereignty was never ceded.
Funding
This research has been supported by an Early Career Research Kick Start Grant through the College of Medicine and Public Health at Flinders University.
Conflicts of interest
There are no other potential conflicts of interest to declare.