


Introduction
Effective management of open fractures focuses on restoring function, preventing complications and minimising long-term disability. The importance of timely interventions in this high-risk cohort stems from the potential for severe consequences including infection, non-union and chronic pain, which can significantly impact a patient’s quality of life1,2.
This study aimed to evaluate and compare the management of patients with open-fracture injuries who presented directly to the major trauma centre in Western Australia (WA), Royal Perth Hospital (RPH), with those transferred to RPH by the Royal Flying Doctor Service Western Operations (RFDSWO) aeromedical retrieval service, representing metropolitan primary presentations versus rural and remote secondary presentations. The goal was to identify areas for improvement in the trauma care pathway, particularly for patients requiring aeromedical retrieval. While previous studies have looked at the aeromedical retrieval of trauma patients within WA3-5, the specific management of open-fracture patients has not been reviewed. This comparison is relevant given the unique geographical and resource challenges faced in WA and the impact of this on delivery of critical interventions such as antibiotic administration and surgical management.
Open-fracture classification
Open fractures are categorised based on the Gustilo–Anderson system, which classifies fractures into three main types based on wound size, contamination and soft tissue damage. Type I fractures have clean wounds up to 1 cm and type II have wounds greater than 1 cm without extensive soft tissue damage. Type III fractures involve extensive soft tissue damage, further subdivided into IIIA, IIIB and IIIC based on tissue coverage and vascular injury. The higher grades are associated with increased risk of both acute and long-term complications1,2.
Prophylactic antibiotic administration
Early prophylactic antibiotic administration is a cornerstone of open-fracture management. Numerous studies have demonstrated that early delivery of antibiotics can significantly reduce postoperative surgical site infections2,6. A landmark study by Patzakis and Wilkins in 1989 showed a significant reduction in infection rates when antibiotics were administered within 3 hours of injury2. This finding has been validated by more recent research, including a study by Lack et al in 2015, which found that immediate antibiotic prophylaxis (within the first hour) was associated with a lower deep infection rate in Gustilo–Anderson type III open tibia fractures6.
Despite some variation on timing in the literature, all major guidelines consistently recommend administering antibiotics as early as possible. The British Orthopaedic Association Standards (BOAST) guidelines recommend antibiotic administration within 1 hour of injury7. In the US, the Eastern Association for the Surgery of Trauma (EAST) practice management guidelines recommend that antibiotics be administered as soon as possible after injury, ideally within 3 hours8. Similarly, the guidelines used in WA, the Australian Electronic Therapeutic Guidelines (ETG) recommend commencing antibiotics immediately after injury for maximum benefit9.
While there is no clear consensus on the exact antibiotic regimen for open fractures, most guidelines recommend a first-generation cephalosporin as the primary antibiotic7-9. Staphylococcus aureus is the most commonly identified pathogen in infected open fractures, and for this reason the ETG recommends IV cefazolin for the initial management of types I and II injuries9. For heavily contaminated wounds or higher grade injuries, additional coverage with metronidazole is recommended9. Other antibiotics are recommended in certain situations, such as cefepime or ciprofloxacin in cases of water exposure9. However, it is important to note that antibiotic choice must consider local antimicrobial resistance patterns, patient factors such as methicillin-resistant S. aureus (MRSA) colonisation and institutional guidelines.
Operative timing
The timing of operative management in open fractures has been a subject of debate in recent years. Historically, the ‘six-hour rule’ for surgical debridement was widely accepted, based on a study by Gustilo and Anderson10. However, this paradigm is currently being challenged. A systematic review by Schenker et al found no significant difference in infection rates between early (less than 6 hours) and late (greater than 6 hours) debridement11. Similarly, a meta-analysis by Prodromidis and Charalambous showed no significant difference in infection or non-union rates between early and delayed debridement12.
Despite these findings, early operative management is still generally recommended, particularly in higher grade or contaminated injuries. The rationale is that early intervention may help to remove contamination, stabilise the fracture and allow for better soft tissue management. However, the emphasis has shifted from rigid time-based rules to prioritising copious low-pressure irrigation and sterile dressing initially, followed by thorough and meticulous surgical debridement as soon as practically possible, regardless of the exact timing13,14. This is mirrored in both the US EAST guidelines and the British BOAST guidelines, which still recommend early operative management, particularly for more severe injuries7,8.
Long-range aeromedical retrieval of open-fracture patients
The RFDSWO provides an aeromedical retrieval service for WA and is responsible for transporting patients from rural and remote locations to the capital city of Perth for higher level care. The service operates 24 hours a day, 365 days a year from five bases (Broome, Port Hedland, Meekatharra, Kalgoorlie, Jandakot (a suburb of Perth)) and utilises both fixed-wing (Pilatus PC-12 and Pilatus PC-24 planes) and rotary-wing (EC-145 helicopters) assets15. RFDSWO faces geographical challenges due to WA’s vast area and low population density outside of the metropolitan area. The state has a land area of over 2,500,000 km2, making up almost 33% of Australia’s total land area, and has a population of approximately 2.9 million, of whom 80% live in the metropolitan area16. All of the state’s tertiary and quaternary health services are concentrated in Perth and minimal services exist in the sparsely populated remote areas of the state. Consequently, RFDSWO handles a significant workload and is one of the only services in the world that routinely transfers trauma patients thousands of kilometres for operative management15.
A study by Fatovich et al highlighted the issues associated with these great distances, showing that rural patients had significantly longer times to definitive care than urban patients, as well as double the risk of major-trauma death3. In a related study, the impact of remoteness on trauma death in WA was examined. The risk of death from major trauma was found to increase with remoteness, with ‘very remote’ areas having a 4.69 times higher risk of death than metropolitan areas4. This increased risk was attributed to longer response times, prolonged total prehospital time and delays in definitive management. An earlier study by Gupta and Rao confirmed the long transfer times for rural patients in WA, with most being transferred to RPH within 24 hours of trauma5, albeit with a mean transfer time of over 9 hours.
In the context of open fractures, these prolonged transfer times can delay both antibiotic administration and operative management, which are critical factors in preventing infection and improving outcomes. Given the inevitability of longer times to operative management in this context, a focus on early and appropriate antibiotic administration is necessary. It is an intervention with good evidence for benefit, minimal risk, and one that can be easily implemented, even in remote settings.
Methods
Study design and setting
This retrospective audit was conducted at Royal Perth Hospital (RPH), the state major trauma centre for WA. Trauma patients with an open fracture who presented for care were included over a 12-month period from January to December 2023. These patients were divided into primary presentations (direct presentation to RPH emergency department (ED) via the metropolitan ambulance service) or secondary presentations (patients retrieved by RFDSWO fixed-wing or rotary-wing services from rural/remote healthcare facilities). Rural and remote healthcare facilities includes any site outside of the greater metropolitan area of Perth, such as country hospitals, nursing posts, remote community clinics and non-facility locations, such as mine sites. These locations are designated on the National Road Trauma Advisory Council framework as level IV or lower trauma centres, meaning they have limited trauma services and patients require transfer to a higher level trauma centre for definitive care.
An additional cohort of secondary presentations were identified and excluded, consisting of patients transferred from metropolitan/outer-metropolitan hospitals to RPH through non-RFDS means such as state ambulance services or private patient transport services.
Data collection
Two methods were used to identify eligible patients. For the primary presentation group, patients who had undergone open-fracture surgery were identified by querying RPH Theatre Management System software data using keyword search. Patient unique medical record numbers (UMRN) were recorded and operation notes accessed via electronic records to confirm their injury and open-fracture surgery.
For the RFDS retrieval secondary presentation group, patients with open fractures were identified by text search and International Classification of Diseases coding in the RFDS electronic medical database. Name, date of birth and UMRN (if available) of patients were collected, along with the date of transfer. These details were then used in the RPH electronic records system to locate the patient UMRN and cross-checked with the list of patients from the primary presentation group. The UMRN was then used to identify and access operation notes via the RPH electronic records system.
A combined list of these patients’ UMRNs were then provided to RPH medical records department and physical files were retrieved for manual review.
Data collected included demographic information (age, sex), injury characteristics (location, Gustilo–Anderson type, wound contamination), presentation type (primary v secondary) and various timings. For both groups, timings included time of injury, time of first healthcare contact, time of arrival in RPH ED, time of first operation and time of first antibiotic dose. For the RFDS group, time of retrieval (defined as the time that the RFDSWO crew took over care of the patient at the referring site) and location retrieved from was also recorded. From these timings, intervals between events such as time from injury to first operation were calculated. Details of antibiotic administration (timing, type, dose, duration and where administered) were also collected.
Inclusion and exclusion criteria
Patient records were included if they met the following inclusion criteria: patient having an open-fracture injury of any Gustilo–Anderson type requiring surgical management; age 12 years or more; presenting to RPH ED directly as their initial healthcare site (primary presentations) or presenting to RPH ED after retrieval from a rural or remote healthcare site by RFDSWO. Exclusion criteria included fractures of the fingers or toes, fractures managed non-operatively or as an outpatient, and incomplete or missing medical records.
Of the final list of patient records collated (n=118), 16 were excluded due to not meeting eligibility or having incomplete documentation. Of the total remaining patients (n=102), 60 were primary presentations and 42 were secondary presentations. Of these 42 patients, 30 were RFDSWO retrievals from rural/remote healthcare sites and 12 were non-RFDS inter-hospital transfers from metropolitan/outer-metropolitan hospitals. The interhospital transfer cohort was excluded from the secondary presentation group analysis, resulting in a final cohort of 90 patients (60 primary presentations and 30 RFDS secondary presentations)(Fig1).
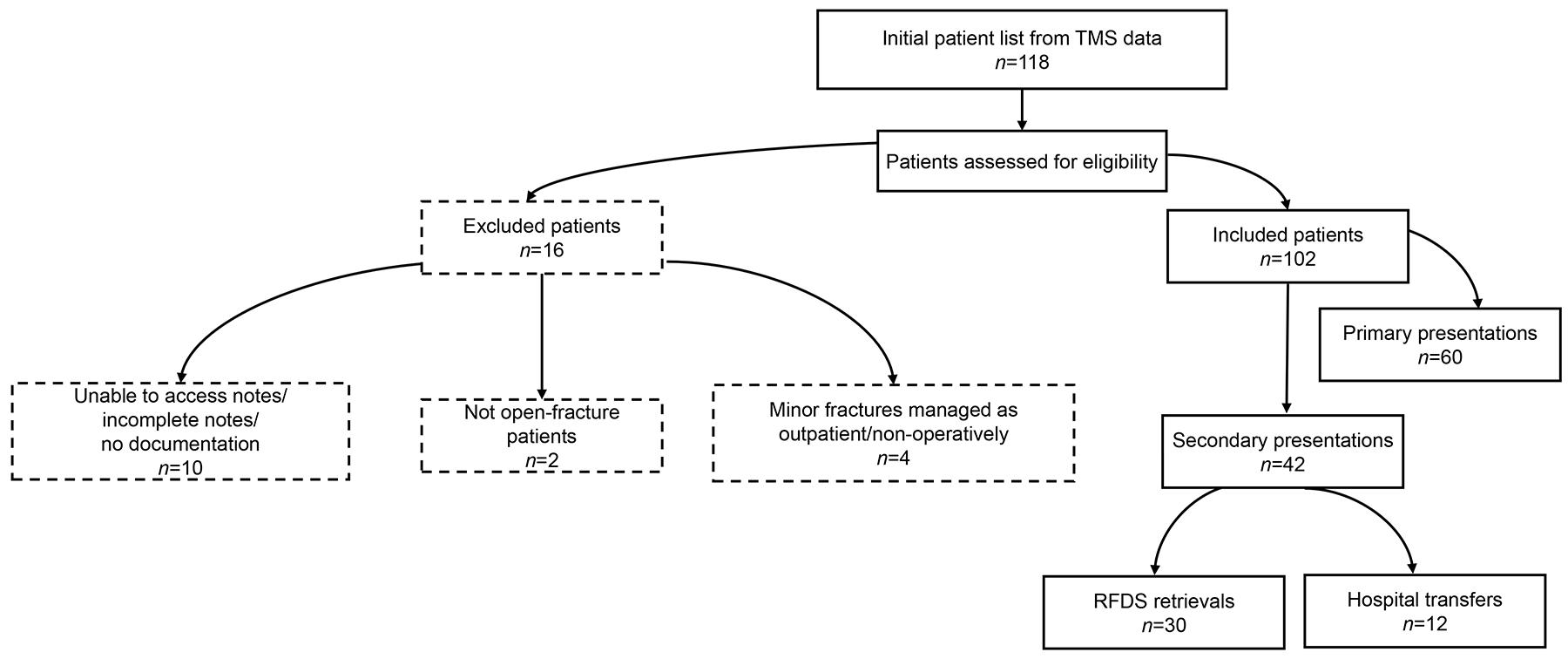 Figure 1: Patient record inclusion and exclusion flowchart. RFDS, Royal Flying Doctor Service. TMS, Theatre Management System.
Figure 1: Patient record inclusion and exclusion flowchart. RFDS, Royal Flying Doctor Service. TMS, Theatre Management System.
Data analysis
Data were extracted from electronic records and inpatient paper notes. This data collection was done on site at RPH, manually entered into Microsoft Excel and securely stored on WA Health computers. Data was de-identified on entry and cleaned to remove duplicate entries, standardise date and time formats and verify group allocation. The cleaned dataset was then imported into Python v3.12.4 (Python Software Foundation, https://www.python.org) for normality testing and inferential analyses using the Pandas and SciPy libraries. All descriptive and basic analyses were conducted in Microsoft Excel. All non-parametric rank–sum tests were performed in Python, with continuous, non-normally distributed variables compared by Mann–Whitney U-test and categorical thresholds compared by Pearson’s χ2 test or Fisher’s exact test.
Ethics approval
Prior to commencing the project, ethics approval was obtained from both RPH and RFDSWO. Following internal governance processes, a research protocol proposal and data release request for the clinical audit were reviewed and approved by the RFDSWO Research Committee and Clinical Governance Committee. Within RPH, ethics approval was gained through the Hospital Surgical Division Committee via the Governance, Evidence, Knowledge, and Outcomes system (quality approval 50956).
Results
Descriptive data
The total group analysed (n=90) was separated into primary presentations (n=60) and RFDS secondary presentations (n=30), as outlined previously.
The mean age of the patients included in the total group (n=90) was 40.2 years, ranging from 14 to 93 years. Males predominated, making up 72% (n=65) of the cases. Injury locations were primarily in the lower limbs (64%, n=58), followed by the upper limbs (34%, n=31). Regarding injury severity, type II injuries were most common (representing 42% (n=38) of cases), followed by type I injuries at 30% (n=27) and type III injuries at 28% (n=25). For wound contamination, fractures were contaminated in 47% (n=42) of the cases, 32% (n=29) were classed as clean/contaminated and 21% (n=19) were clean.
Aeromedical retrieval
Patients were retrieved from all over WA, with a large representation from the northern regions (Fig2). The median distance travelled was 1246 km with a maximum distance of 2216 km for three patients retrieved from Kununurra. (These distances are likely underestimated as direct-line distances from retrieval location to RPH.). The time from injury to arrival and takeover of care by the RFDS retrieval team falls in line with previous studies, with a median time of 14.1 hours (interquartile range (IQR) 10.1–24.3) and 73% (n=22) of patients retrieved within 24 hours (Fig3).
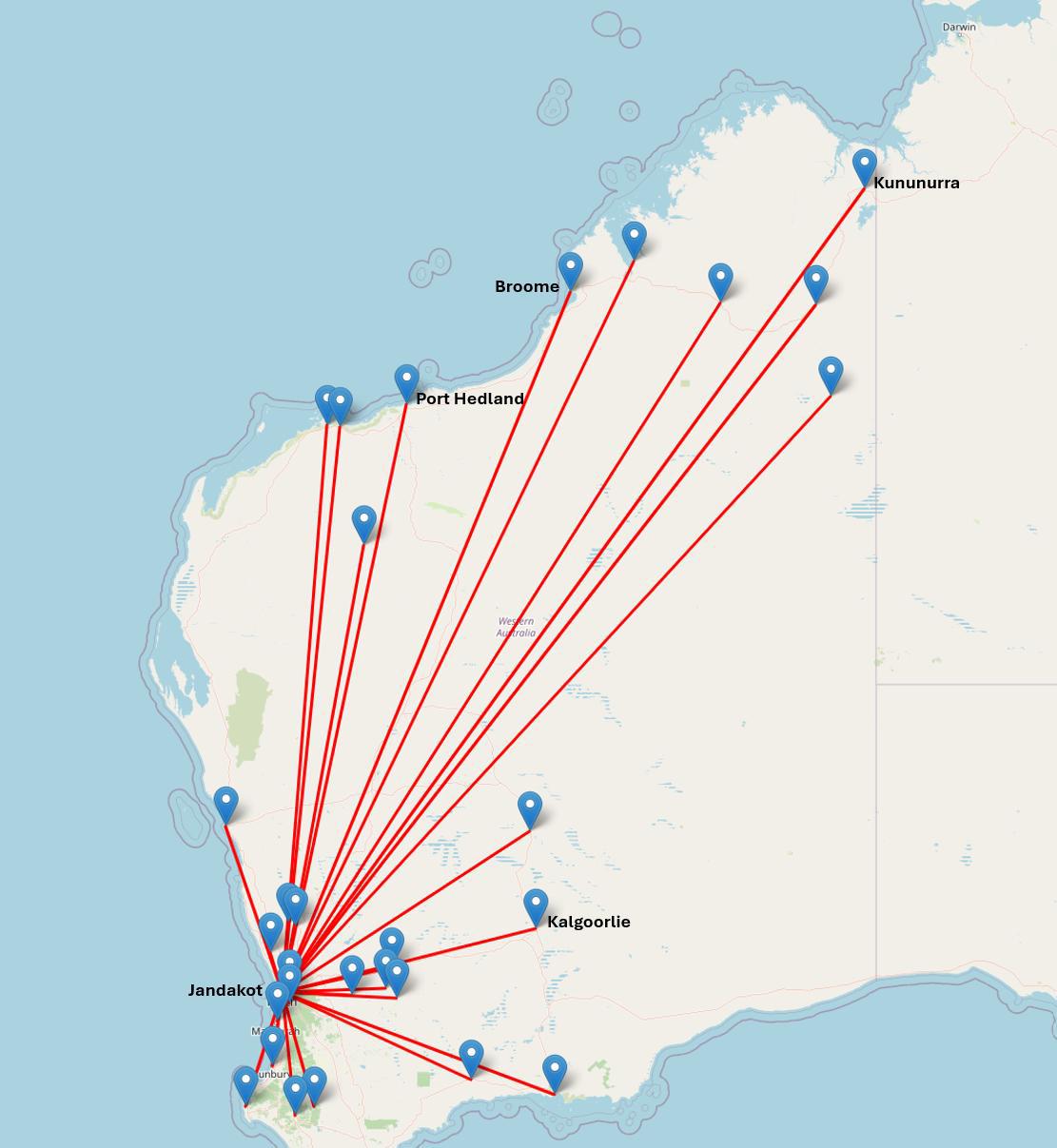 Figure 2: Map of retrieval locations for secondary presentation patients.
Figure 2: Map of retrieval locations for secondary presentation patients.
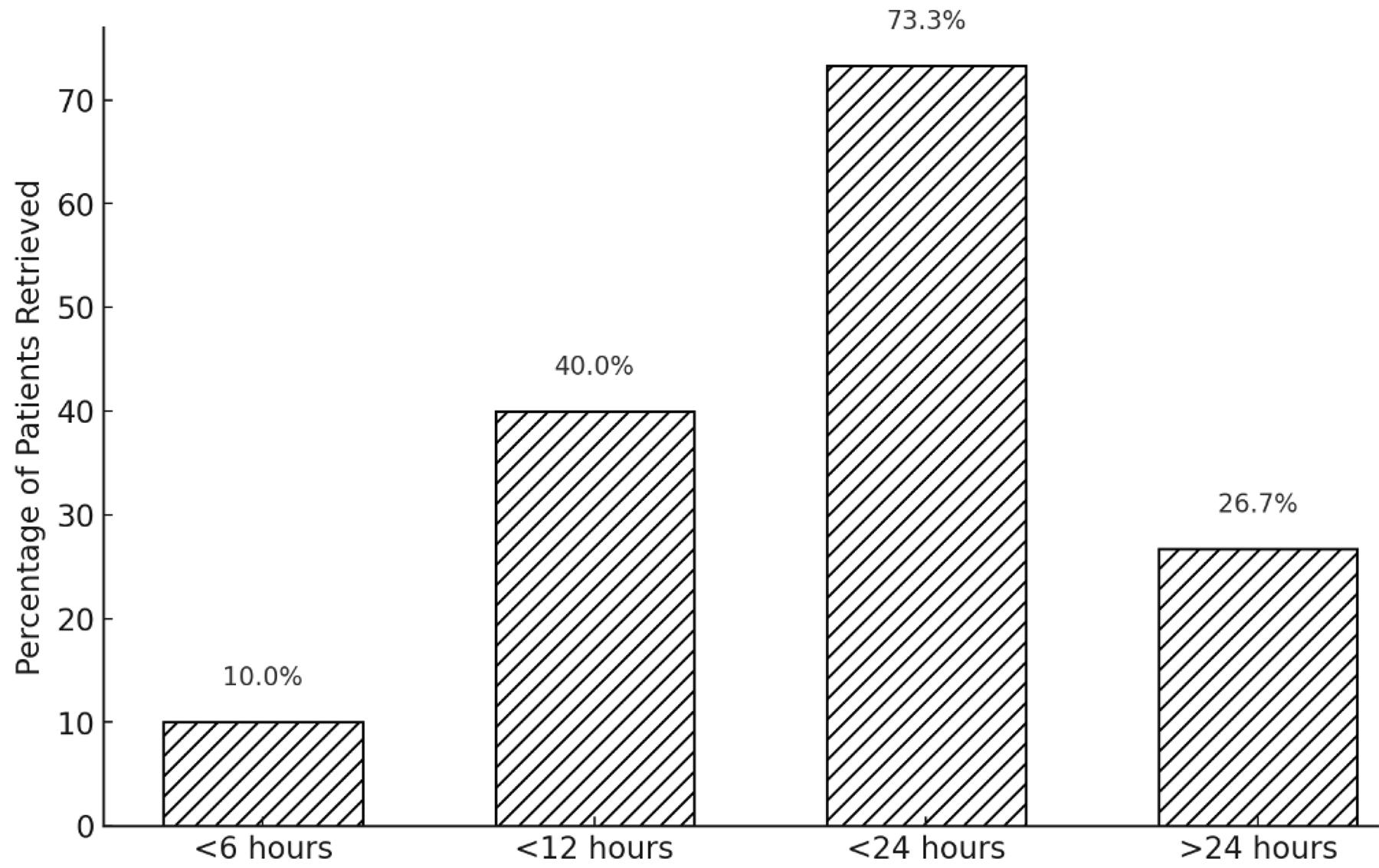 Figure 3: Time from injury to Royal Flying Doctor Service Western Operations retrieval.
Figure 3: Time from injury to Royal Flying Doctor Service Western Operations retrieval.
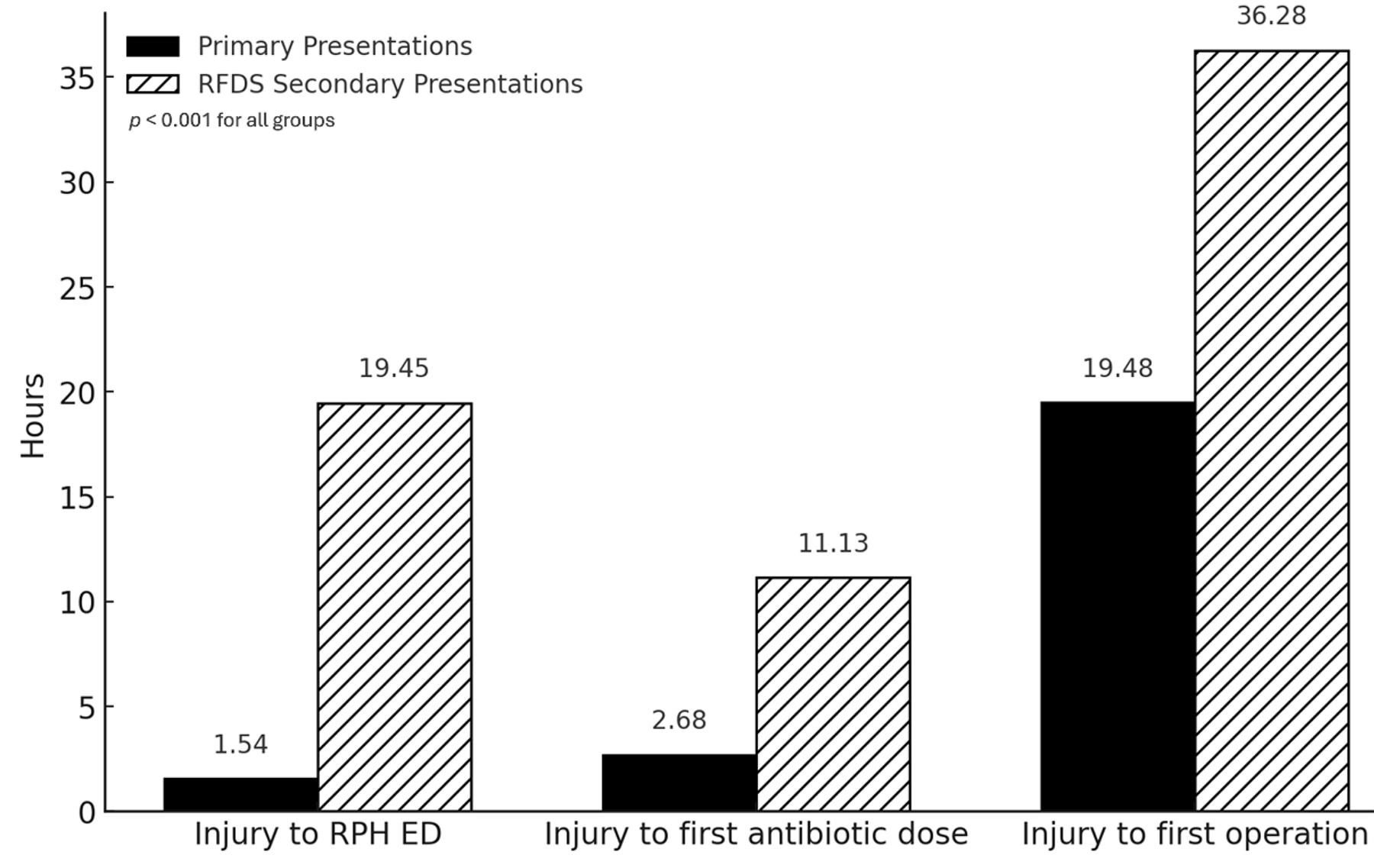 Figure 4: Comparison of median timings, by time since injury. ED, emergency department. RFDS, Royal Flying Doctor Service. RPH, Royal Perth Hospital.
Figure 4: Comparison of median timings, by time since injury. ED, emergency department. RFDS, Royal Flying Doctor Service. RPH, Royal Perth Hospital.
Timings
The time intervals between key events were calculated and compared between the primary presentation and secondary presentation groups, focusing on time to critical interventions such as antibiotic delivery and operative management. The secondary presentations had significantly longer times for all metrics. Most notably, the median time from injury to arrival in RPH ED was 1.5 hours (IQR 1.3–2.2) versus 19.5 hours (IQR 13.8–27.9), median time from injury to first antibiotic dose was 2.7 hours (IQR 1.8–4) versus 11.1 hours (IQR 5.0–19.6) and median time from injury to first operation was 19.5 hours (IQR 15.6–23.8) versus 36.3 hours (IQR 28.1–58.7) (Fig4). p-values were derived, with all comparisons yielding p<0.001, indicating statistical significance.
Another way to visualise this data is to assess the percentage of patients that underwent an intervention within a certain time frame. For antibiotics, approximately 53% (n=32) of primary presentation patients were given antibiotics within 3 hours of injury compared to only 13% (n=4) in the secondary presentation group (p<0.001). This increased to 85% (n=51) versus 33% (n=10) in the first 6 hours (p<0.001) (Fig5).
Time from injury to first healthcare contact was also analysed. For the primary presentation group, the median time was 17 minutes (IQR 10–44) compared to 114 minutes (IQR 53–312) for the secondary presentation group representing rural and remote patients with p<0.001.
For time to operation, approximately 75% (n=45) of the primary presentation patients were operated on within 24 hours of their injury compared to just 17% (n=5) of the secondary presentation patients (p<0.001) (Fig6). This fits with our previous data, given the median time to arrive at RPH ED from time of injury was over 19 hours for the secondary presentation group.
To remove the confounder of prolonged retrieval times for secondary presentation patients, the time from arrival at RPH ED to first operation was also calculated. Once transfer time was removed, the median values were 17.9 hours for the primary group and 16.5 hours for the secondary group with a p-value of 0.94, demonstrating there is no statistically significant difference between the time to surgery for these two groups.
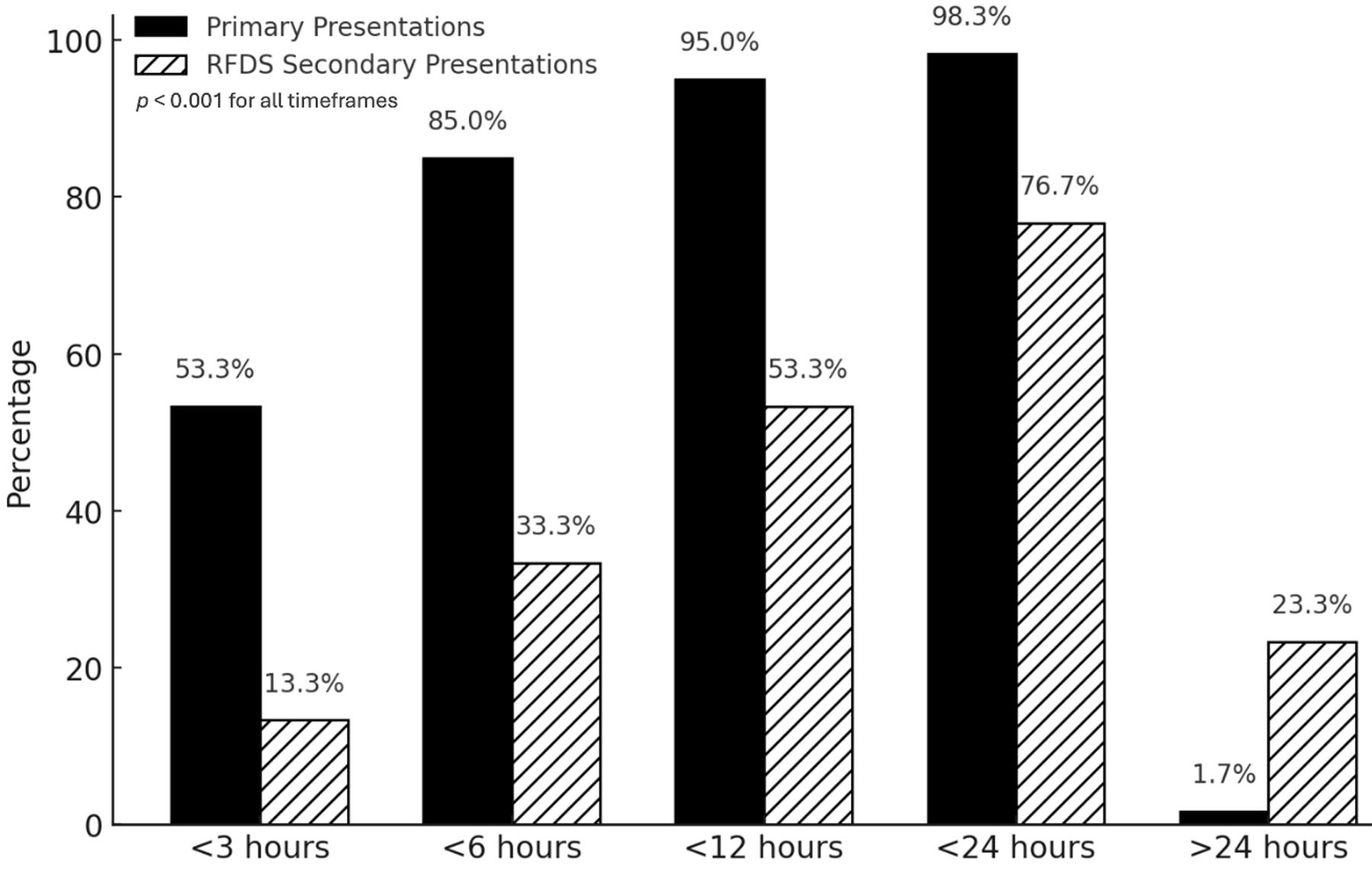 Figure 5: Percentage of patients receiving antibiotics, by time since injury. RFDS, Royal Flying Doctor Service.
Figure 5: Percentage of patients receiving antibiotics, by time since injury. RFDS, Royal Flying Doctor Service.
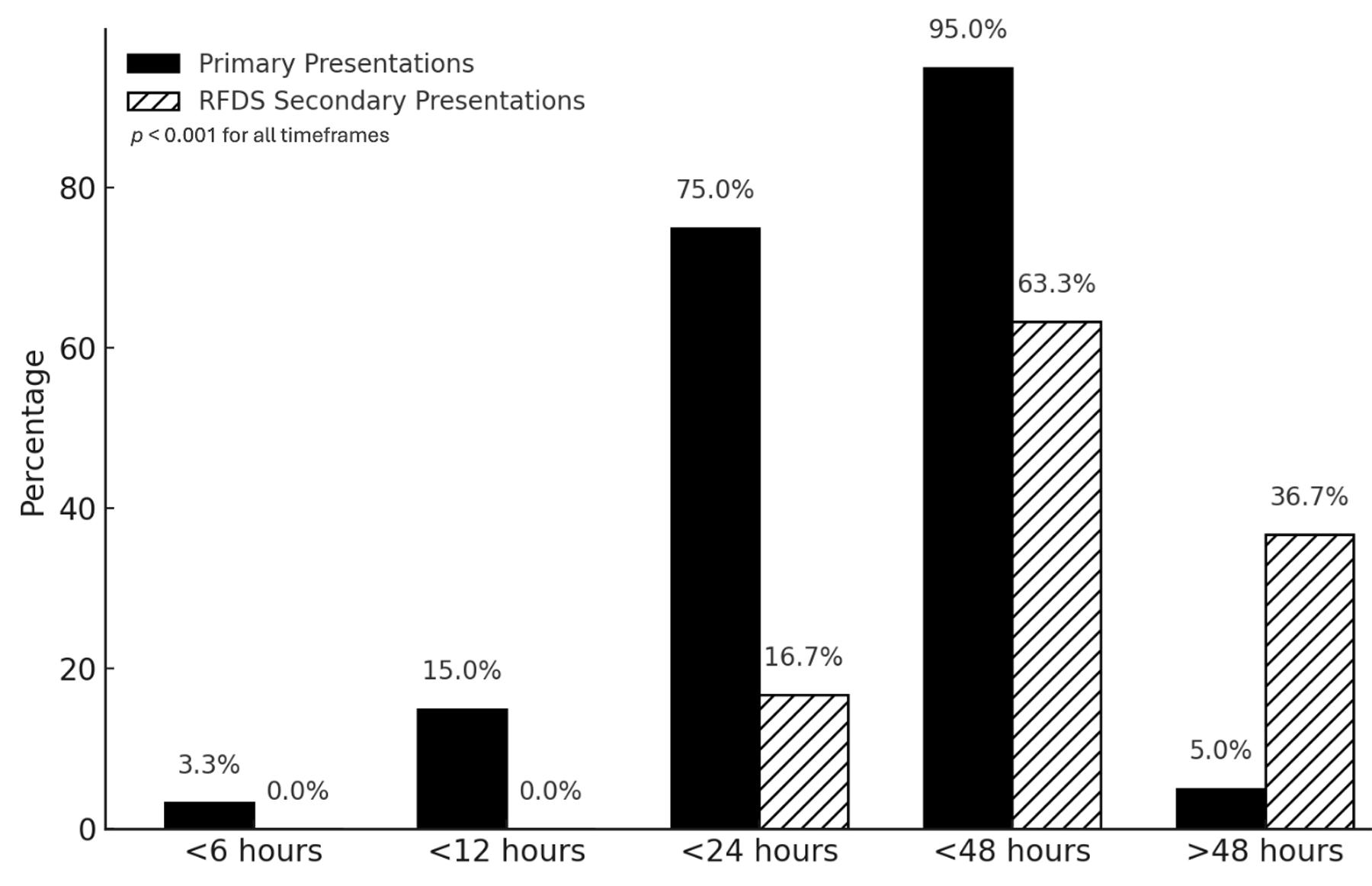 Figure 6: Percentage of patients undergoing surgery, by time since injury. RFDS, Royal Flying Doctor Service.
Figure 6: Percentage of patients undergoing surgery, by time since injury. RFDS, Royal Flying Doctor Service.
Antibiotic administration
The majority of patients in both groups received a dose of 2 g of cefazolin intravenously as suggested by the ETG guidelines. In the primary presentation group, 97% (n=58) of patients received 2 g of cefazolin as an initial antibiotic versus 60% (n=18) in the secondary presentation group (p<0.001). There was substantially more variation in the antibiotics given in the secondary presentation group, including use of broader spectrum antibiotics such as amoxicillin–clavulanic acid and appropriate use of vancomycin for an MRSA-positive patient, and ciprofloxacin for an open fracture contaminated with brackish water.
Limitations
The audit data was extracted through a review of electronic records (including discharge summaries, operation notes and theatre management software) and physical review of paper records (including inpatient progress records, admission notes, trauma proformas, ED notes, medication charts, RFDSWO transfer charts, ambulance transfer charts and discharge summaries/notes from secondary sites). While all effort was made to cross-reference data and calculate accurate times, there was reliance on accurate documentation by the various health professionals involved in patient care. In some cases, documentation was unclear or variations in timings documented; in these cases, an educated guess was made after referencing recorded arrival and departure times at different healthcare locations and any documentation about the timeline of events. In addition, given the complexity, duration and multiple healthcare providers involved in aeromedical retrieval of patients from rural and remote sites, it is likely that missing or inaccurate data disproportionately affects the secondary presentation group.
Discussion
The secondary presentation group had longer median times for all metrics measured – in particular, time to reach RPH ED, time to receive first antibiotics and time to first operation.
The timing and type of antibiotic administration emerged as a critical issue in this audit. As highlighted in the introduction, the importance of early and appropriate antibiotic administration in reducing complications is well established in the literature and current guidelines.
Primary presentations were well managed, with the median time from injury to first antibiotic less than the recommended 3 hours. If we examine the median time to antibiotics after arriving in ED, this number further improves to 59 minutes, suggesting the key delays are prehospital, such as long transport times, inability to handover (ramping of ambulances in ED) or delayed initial calls to health services.
However, for the secondary presentation group, the median time to first antibiotic dose was more than 11 hours, with only 13% and 33% receiving antibiotics in less than 3 and 6 hours from time of injury respectively. It is important to consider contributing factors, such as the median longer time from injury to first healthcare contact (almost 2 hours compared to only 17 minutes for the primary presentation patients) and availability of appropriate antibiotics in remote sites. From a review of patient records, the delay was most frequently due to antibiotics not being given at the initial healthcare contact point and only being administered once the patient had been transferred to another facility, for example from a nursing post to a country hospital. There is great heterogeneity of initial healthcare contacts for rural/remote patients (nursing post, mine-site medic, volunteer ambulance officer, hospital), all with different skills, resources and protocols, which further complicates the situation. This highlights the importance of education and resources directed at all levels of healthcare provider.
When antibiotics were given, the appropriate choice of IV cefazolin was given in the majority of cases, particularly in the primary presentation group, where it was administered to 97% of the patients. Of note, out of the total 90 cases, only one patient was given metronidazole. Metronidazole was not given in any of the higher risk cases, which included 25 injuries classified as type III and 45 classified as having contaminated wounds. This goes against the ETG recommendations of including IV metronidazole 500 mg in adults with heavily contaminated open-fracture wounds9.
The time of the initial antibiotic dose was the data point collected for results analysis. So, although ongoing antibiotic provision was not quantitatively examined, during review of patient records a lack of repeat dosing of antibiotics was noted during long-range retrievals or delayed transfer to tertiary care. The ETG recommends redosing cefazolin 8 hourly to maintain efficacy9. A number of patients in the secondary presentation group received an initial dose but no further dosing until they reached definitive care. Additionally, on multiple RFDSWO transfer documents, the flight doctor noted that the patient should be receiving cefazolin but it was not stocked. This has since been resolved, with RFDSWO now carrying cefazolin in the flight medication box. However, given the long duration retrievals in WA, it is pertinent to ensure adequate repeat doses are stocked, including alternative antibiotics to cover situations such as an MRSA-positive patient or a highly contaminated wound. Further data collection on repeat dosing would be useful to fully assess this observation.
The risks associated with administering IV antibiotics are low and manageable by health professionals, with the most concerning reaction being anaphylaxis. There may be hesitancy to administer prophylactic cefazolin in trauma patients who have not been able to disclose their allergies or have documented allergies to penicillins or cephalosporins. The ETG provides clear guidelines on when it is appropriate to give cephalosporins in patients with documented allergies, and alternative agents to use in those cases9. This should not present a barrier for improving the rates of early antibiotic administration in open-fracture patients.
From the definitive surgery perspective, while there was an increased median time from injury to operative management in the secondary presentation group (36.3 versus 19.5 hours), this difference disappears when the times are analysed from arrival time in ED rather than time of injury. Therefore, the aforementioned challenges of long-range transfer explain the observed increase in time from injury to surgery in this group. This metric is unlikely to be easily improved given the complexity of aeromedical retrieval, competing demands on RFDSWO asset availability and large distances involved. Given the lack of evidence supporting a rigid ‘six-hour rule’ to operative management, the focus of rural and remote sites should remain on comprehensive open-fracture care including low-pressure irrigation of the wound, sterile dressing and prompt antibiotic delivery. Compliance with early wound irrigation and sterile dressing was not assessed in this audit, but these measures remain recommendations in the BOAST and EAST trauma guidelines7,8 and are simple interventions that can and should be performed alongside early antibiotic administration.
Overall, this audit raised a number of points for further review. Given the importance of early antibiotics on reducing morbidity, particularly in patients with delayed transportation to definitive care, there is a need to review and improve protocols for early antibiotic administration at rural and remote sites, as well as during aeromedical transport. Additionally, there is a need for further education and training for healthcare providers at all levels of the trauma care system on the importance of early antibiotic administration in open-fracture management.
Current guidelines are not representative of the austere environments experienced in rural and remote Australia. Consideration of the difficulties and time delays in accessing initial healthcare services, as well as transport to tertiary care, must be addressed. Furthermore, not all sites have access to IV antibiotics, or the scope of practice or knowledge to initiate these.
To address this, a potential solution is the use of the RFDS Medical Chest program, which consists of over 2300 chests across Australia and includes various emergency medications for remote communities to use in conjunction with a telehealth consult from RFDS15. Within this chest are oral antibiotics that could safely be administered early after injury and prior to arrival at a healthcare site that can give IV medications. While the oral versions of these antibiotics (cephalexin, metronidazole and amoxicillin–clavulanic acid) have not been evaluated in prospective open-fracture prophylaxis trials, they are widely used for bone and joint infections and have excellent bioavailability and bone penetration17. In certain guidelines, such as the Children’s Minnesota hospital in the US, oral cephalexin is endorsed as an alternative to IV antibiotics for types I and II open fractures18. In the military context, the US Tactical Combat Casualty Care guidelines recommend oral moxifloxacin as first-line prophylaxis for any open combat wounds, including open fractures19. Intramuscular antibiotics were also considered. Many first-contact providers who lack the scope of practice for commencing IV therapy are likewise not authorised to give intramuscular injections. However, under RFDS telehealth direction, the medical chest does contain a ceftriaxone vial, sterile water, syringe and needle, which could be used to deliver a single dose of antibiotics. The evidence base for intramuscular ceftriaxone prophylaxis in open fractures is lacking and presents a number of issues, namely that these injections are painful, time to peak concentration is slower than the oral antibiotics available in the chest, and ceftriaxone provides limited anaerobic cover so broader cover (such as oral metronidazole or amoxicillin/clavulanic acid) may still be required in contaminated injuries. Despite this, intramuscular ceftriaxone may be a pragmatic option when neither IV access nor an oral route is feasible, such as in patients with maxillofacial injury, depressed consciousness or severe nausea and vomiting.
Based on this, an open-fracture clinical practice guideline has been written, reviewed and published in the latest internal RFDSWO Clinical Manual (version 13.1, March 2025; internal document, cited with permission). This guideline focuses on a pragmatic approach to open-fracture management for retrieval doctors as well as guidelines for the use of oral antibiotics from the RFDS medical chests to treat patients with an open fractures in low-resource settings. In addition, educational material has been developed and distributed to ensure the RFDSWO service is providing the optimal care and advice when undertaking aeromedical retrievals, telehealth consults or advice to rural and remote sites.
Finally, the data collected in this study provide an insight into the importance of the Western Australian aeromedical retrieval service within the state trauma system. It paints a clear picture of the extremely long distances travelled and challenges faced when treating trauma patients in austere and isolated environments. For this reason, it is imperative that the unique demands that are placed on WA Health services are taken into account when developing future protocols or policies and when delivering education to healthcare providers.
Conclusion
Patients with open fractures in rural and remote WA face longer times to antibiotic administration and definitive surgical care due to geographical isolation and to the logistical complexities of long-range aeromedical retrieval. The findings from this audit highlight the uniquely challenging environment faced in these situations, where delays to definitive care are often unavoidable.
In this context, early open-fracture trauma care including wound irrigation, sterile dressings and prompt prophylactic antibiotic administration are low-risk, low-cost and high-yield interventions that may reduce infection risk during prolonged transfer. There is ongoing need for widespread education of all rural and remote healthcare providers on early antibiotic administration, including optimal timing, appropriate dosing and antibiotic selection for open fractures. Achieving this will help standardise care and reduce preventable delays. By tailoring trauma protocols to the realities of rural practice and prioritising timely interventions like antibiotic prophylaxis, healthcare systems can better serve patients across WA.
Acknowledgements
The authors wish to thank Dr James Anderson (RFDSWO) and Dr Nicholas Enzor (RPH) for their support and assistance in planning the audit, Dr Rochelle Menzies (RFDSWO) for her research advice, Helen Bartholomew (RFDSWO) for her assistance in accessing RFDSWO data and Dr Lauren Masi (RPH) for her assistance in data entry.
Funding
The authors received no specific funding for this work.
Conflicts of interest
The authors declare no conflicts of interest. The RFDS Medical Chest scheme is a government-sponsored telepharmacy program. Medical chests and medication are provided free of charge to eligible remote residents, whereas corporate/industrial users may subscribe on a cost-recovery basis. The authors do not receive, and will not receive, any financial benefit, direct or indirect, from the use of the RFDS Medical Chest program.
AI disclosure statement
No generative AI or AI-assisted technologies were used in the preparation of this manuscript.