


Introduction
Rural and remote communities face ongoing challenges in accessing timely, appropriate, and culturally responsive mental health care. Among these populations are farmers, who are particularly vulnerable due to the wide range of stressors they experience including unpredictable weather, volatile markets, financial strain, physically demanding labor, long work hours, and increasing geographical and social isolation1-3. In Canada, farmers consistently report higher rates of depression, anxiety, stress, as well as suicide, compared to the general population3-6, with similar patterns reported in Australia7, the US8, and the UK9. Yet, farmers tend to be low help-seekers10,11. A common barrier to care is the perception that mental healthcare providers (MHCPs) do not understand their culture, values, or lifestyle12. As a result, even when farmers do seek counselling, their willingness to return may depend on how well the provider is able to build rapport and earn their trust. With growing pressure among policymakers, industry groups and healthcare organizations to improve mental health support for farmers, it is essential that these services are not only accessible but also culturally responsive.
Barriers to help-seeking and accessing care
Seeking early treatment can improve long-term health outcomes13. However, farmers are about half as likely to access mental health support compared to non-farmers, with 9% of farmers reporting that they saw a health professional for mental health reasons in the previous 12 months compared to 16% of non-farmers10. Barriers to help-seeking among farmers are well documented and include stoicism, self-reliance, stigma, limited mental health literacy, and structural constraints such as distance, cost, and long wait times12,14-16. For example, a survey of Australian farmers revealed their concerns about care were that others would view them differently if they sought professional help, wait times for appointments take too long, and they would not get to see their preferred provider15.
Adapting mental health services for rural and farming communities
In response to these barriers, research has explored ways MHCPs have adapted their services and approaches to align with the cultural values and lifestyles of farmers17,18. Therapists have reported adapting service delivery (eg flexible scheduling and modes of contact) to accommodate farmers’ unpredictable schedules and privacy concerns18. MHCPs also emphasized the importance of establishing ‘farm credibility’, defined as understanding the unique needs and challenges associated with the agricultural lifestyle12. Indeed, farm credibility may be an important step in establishing therapeutic alliance among farmers19,20, which is considered a key treatment outcome21. For instance, a study of Canadian farmers reported that therapists who demonstrated knowledge of farm culture, including its values, stressors, and family dynamics, were viewed as credible and empathetic20. While establishing farm credibility is important, there is limited research exploring how trust is developed and maintained within the therapeutic relationship with farmer clients.
Purpose of the study
Therapeutic alliance is recognized as a key factor in treatment engagement and outcomes22. However, despite growing awareness of the mental health challenges faced by farmers and efforts to improve access to care, there remains limited research describing how MHCPs build trust and sustain engagement with this population. Although some community-based services and counselling practices have successfully adapted their approaches to better align with farmers’ unique needs18,23, the processes through which they build trust and foster therapeutic relationships remain unclear. Therefore, the purpose of this study was to explore the perspectives of MHCPs who provide services to farmers to identify the strategies for fostering trust and therapeutic alliance. Our goal is to use this information to inform policy, practice, and training in rural mental health care.
Methods
Research design
We conducted a qualitative study informed by a descriptive phenomenological approach. This approach emphasizes understanding and describing participants’ experiences of a particular phenomenon24. In the present study, this approach guided our focus on how mental health providers experience the process of building therapeutic alliance with farmers. To systematically identify patterns of meaning across participants’ accounts, we used Braun and Clarke’s thematic analytic method25, as described in the data analysis section.
Study sample
Participants needed to be licensed or credentialed MHCPs, including registered psychologists, social workers, and Canadian Certified Counsellors, who provided counselling services and had been practicing for at least 12 months. They were required to have current or recent clients who were farmers and to have a background in farming (eg from a farm family, worked in agriculture, currently live on a farm) or live in a rural area. Detailed professional designations and sample characteristics are presented in Table 1.
Table 1: Study participant characteristics
| Characteristic | Variable | n (%)/mean±SD |
|---|---|---|
| Age | 49.36±11.95 | |
| Years practicing | 11.72±9.37 | |
| Therapy certification | Canadian Certified Counsellor | 12 (48) |
| Registered social worker |
8 (32) |
|
| Registered psychologist |
5 (20) |
|
| Therapeutic approach† | Psychotherapy therapy | 25 (100) |
| Equine-assisted therapy |
3 (12) |
|
| Art therapy |
1 (4) |
|
| Type of practice | Private practice | 19 (76) |
| Healthcare organization |
4 (16) |
|
| Community-based service |
2 (8) |
|
| Background in agriculture | Yes | 20 (80) |
| No, but lives in a rural community |
5 (20) |
† Participants could report more than one therapeutic approach; therefore, percentages may exceed 100%.
Data collection
We used purposive sampling to recruit participants through notices posted to our study website and social media accounts (eg Facebook, Instagram, newsletters) between March and May 2024. Individuals interested in participating contacted the principal investigator by email or telephone to schedule an interview. After participants provided their verbal informed consent, they completed an individual, semi-structured interview with the principal investigator that lasted approximately 45–60 minutes online or by telephone. A semi-structured interview guide was developed based on a review of the literature and prior research conducted by the authors. The guide included five background questions (about age, type of practice, therapeutic modalities, years practicing, background in agriculture) and seven open-ended questions exploring providers’ experiences building trust and therapeutic alliance with farmer clients. The interview guide is provided in Table 2. Participants received a C$25 (A$25.50) gift card to an online retailer. Each interview was audio-recorded and transcribed verbatim.
Table 2: Semi-structured interview guide
| Question | Prompt |
|---|---|
| 1. In your experience, what kind of support are farmers looking for? | What kinds of mental health needs do people in farming communities have? |
| 2. What works for engaging with farmer clients? | What doesn’t work? What recommendations would you give someone starting in a rural/farming area? |
| 3. How do you build trust in a therapeutic setting with a farmer? | What is your approach? How do you encourage them to talk or feel comfortable? |
| 4. How long does it usually take to build trust with a farmer client? | |
| 5. What differences, if any, have you observed between farmer and non-farmer clients that would be important for a therapist who has never worked with them to know? | |
| 6. What challenges do you face practicing in a rural or farming community? | |
| 7. For farmers who have never spoken about mental health, what do you do that might help them through this process? |
Data analysis
Two research assistants screened the transcripts for accuracy and removed identifying information. We uploaded the transcripts to Quirkos v2.5 qualitative software (Quirkos; https://www.quirkos.com/index.html) for data analysis and data management. The three authors independently reviewed and analyzed the transcripts using Braun and Clarke’s six-step thematic analysis approach25, including (1) reading the transcripts to become familiar with the content and participant’s perspectives, (2) identifying words and phrases relevant to the research question to form initial codes, (3) reviewing the initial codes and grouping similar codes to develop possible themes, (4) reviewing and refining themes to ensure they are a coherent description of the data, (5) defining and labelling each theme, and (6) preparing a narrative of the findings that address the research question. For steps 3 and 4, we stopped the coding process when no new ideas emerged26. As part of step 6, we presented the findings both in written form and as a visual summary – the Farmer-Centered Therapy Framework – which was developed after the themes were identified to provide a clear and accessible representation of the participant-derived strategies described in the study without introducing interpretation beyond participants’ accounts.
We used bracketing throughout our analysis, which involved acknowledging and setting aside preconceptions so that participants’ perspectives remained the focus27. To do this, the research team included investigators with varying familiarity with farming and rural mental health, including two members with limited direct exposure to agricultural communities. We recognized that prior assumptions about farm culture and help-seeking could shape interpretation, and therefore we included ongoing reflexive discussion during weekly meetings to examine how our perspectives influenced coding decisions. Multiple team members coded the data to support reflexive discussion, deepen our understanding of the data, and ensure analytic coherence. We invited the participants to review our findings and provide feedback about whether our findings reflected their experiences and observations. No participant requested changes.
Ethics approval
Our study was approved by the University of Alberta’s ethics review board (Pro00138661). Each participant provided verbal consent before their interview.
Results
Participant characteristics
We interviewed 25 MHCPs who provided therapy to farmers. The sample included mostly women (n=18, 72%) and therapists who offered services through a private practice (n=19, 76%). Participants ranged in age from 34 to 75 years (mean=49.36, standard deviation=11.95), and had been practicing for approximately 11.72 years (standard deviation=9.37), ranging from 1 to 35 years. Participants were primarily practicing in Alberta (n=22) reflecting the Alberta-focused recruitment strategy; however, a small number of providers (n=3) from Ontario participated after encountering the study invitation through national professional networks and online groups. While all provided psychotherapy or ‘talk therapy’, three MHCPs provided equine-assisted therapy and one MHCP offered art therapy. While all participants had experience living in rural areas, the majority (n=20, 80%) had a background in agriculture or were part of a farm family (Table 1).
Qualitative analysis
Our analysis revealed five major themes. Each theme and subtheme is described below, with verbatim quotes from the participants.
Understanding unique stressors among farmers
Although the MHCPs described that clients often presented with common symptoms of depression, anxiety, and stress, they emphasized that these concerns were often shaped by a distinct set of occupational and cultural stressors. Participants described that recognizing and demonstrating an understanding of these farm-specific pressures was an early trust-building strategy that helped them establish rapport and engage clients more effectively. We organized these stressors into four subthemes, which providers identified as central to connecting with farmers during therapy.
Intergenerational trauma
Participants described how many of their clients experienced childhood trauma, sexual abuse, religious control, physical abuse, and emotional neglect, which was often compounded with pressure to uphold family legacy and traditional values. The MHCPs observed that their clients acknowledged that trauma and abuse were recurring patterns experienced across generations, and the emotional pain and coping methods were also passed down, normalized, and never discussed within families. One MHCP explained:
There's a lot more people that didn't deal with their trauma. So, if you have grandparents or great grandparents who didn't deal with their trauma and stress then they're passing that along through their children or their children's children. (participant 6)
The deep-rooted culture of self-reliance and mental health stigma made it difficult for earlier generations to seek support. For some clients, therapy only became accessible after those who caused or enabled the trauma had died. One MHCP explained:
My clients are coming for therapy in their 80s now to deal with their trauma … They’re seeking help now because their husband or family have passed, and they feel safe to come forward. (participant 3)
Gendered expectations and isolation
Therapists described how traditional gender roles and rural isolation enhanced stress for their clients. Women clients often felt trapped and unprepared for their roles on the farm, with many having moved to the farm for marriage, managing dual roles and unpaid labor, and being isolated. Male clients felt the pressure of having to take over the farm one day, and were overwhelmed by that process and preferred avoiding the discussion with family. One MHCP explained:
There's still a huge gender difference. So, the typical ‘blue jobs’ versus ‘pink jobs’, right? I have a couple of female clients now who … are starting to resent their partners … You know, they’ll say ‘I got married, I'd never been on a farm before and I'm isolated.’ (participant 4)
These challenges were further intensified by shrinking rural populations, limited social support, and reduced peer networks. One MHCP explained, ‘they don't have as much social support in smaller communities. They're closing community centers because they don't even have enough people to put together hockey teams’ (participant 20).
Substance use
Participants described that substance use, particularly alcohol, was a common and culturally acceptable coping mechanism. Several MHCPs observed a seasonal pattern of substance use, whereby usage increased during the winter months (off-season) and decreased during the spring to fall months (busy season), but the exact reason for these patterns remained unclear. One MHCP explained:
So I have been working with a few people over the years. Their drinking or substance use would increase over the winter months. And, yeah, it's the chicken or the egg situation: Is it seasonal affective type stuff happening? Is it boredom? Is it both? Is it just a lack of purpose felt during the off-season? Or maybe it’s a ‘this is my time, I can drink more because this is my self care.’ (participant 4)
Several MHCPs suspected high-functioning alcoholism, where farmers continued to meet their work responsibilities despite their substance use, making it difficult for them and others to recognize the problem. One MHCP explained:
A number of my [clients] experience substance use to what we would call an unhealthy level. I don't know that the average farmer would consider it an unhealthy level because within our agriculture culture, substance use is a little bit more accepted. (participant 23)
Substance use was a common coping method for stress or other longstanding mental health issues. One therapist explained:
It's about how they're handling the stress, you know, some are drinking more, some are using drugs … they're not handling [the stress] very well. They're bottling it up. And that's overflowing to the rest of the family and their friends. (participant 5)
Uncontrollable factors
Farmers faced a range of external stressors such as extreme weather including droughts and floods, changing government policies, and equipment breakdowns. What made these challenging were their unpredictability and financial strain, contributing to feelings of vulnerability and hopelessness. One MHCP explained:
You can't even fix your own machines in some cases anymore. The equipment has become so specialized that when something breaks down, you can’t go to a neighbor and get a part. And then you need to buy your seed and your chemicals ... All the inputs are outside of your control, and that can deteriorate that sense of independence … [And] you can't make it rain. (participant 7)
Setting the tone
Participants described intentionally designing a ‘familiar’, non-clinical environment for their farmer clients that felt like they were having a conversation with a peer. Common strategies focused on first impressions and creating an environment that limited formality and included comfortable couches and throw pillows, and warm lighting. Several therapists offered counselling from farm-based offices. One therapist explained:
I think the first thing would be accessibility in terms of how you're offering your services and how you are being approachable. Like, is it a warm and welcoming space? Do people want to come there? (participant 12)
Participants also described making deliberate choices about their outward presentation, such as wearing practical, relatable clothing and greeting their clients with a handshake to mimic a typical greeting if they were to engage with this person in any other setting. One therapist mentioned, ‘You know, it might just start with a greeting and a handshake … Lots of farmers still value a good handshake’ (participant 2).
Building trust
Building trust was described as a major milestone that unfolded through ongoing relational interactions after the therapeutic space was established. Participants described the importance of making connections, empowering them, and validating their stressors and experiences. Compared with their non-farmer clients, participants noted that trust often developed more gradually, with farmers taking at least three sessions to feel comfortable and begin ‘opening up’ to them. Whereas setting the tone reflected the intentional changes a MHCP made to the physical environment and their behavior at the outset, building trust reflected the relational work that happened over time. We identified four subthemes MHCPs used to build trust.
Addressing expectations
Participants noted that going to therapy and discussing emotions and personal matters with a stranger was unfamiliar territory for most farmers, with many expecting a quick solution to their problem. One therapist explained ,‘Sometimes people don't seem to know that therapy isn’t going to be the "fix" necessarily’ (participant 1). Participants spent time in the early stages of therapy discussing expectations, including that therapy takes time and issues can unfold slowly. Several participants observed that their clients delayed seeking help until they reached a crisis point. One therapist explained, ‘More often than not, it reaches a fairly major breaking point before they do end up in our office, which is really unfortunate’ (participant 9).
Making connections
Building trust with farmers often required establishing a connection to agriculture or rural life, and a genuine interest in farming. Some used phrases familiar to farmers to subtly signal that they ‘speak the same language’. One MHCP explained, ‘With any group that you're working with, real connection starts with understanding their culture’ (participant 25). Others mirrored language and behavior, acted as a ‘springboard’ for thoughts, attended to body language, used humor, and asked questions about the farm and how the season is going at the beginning of each session. One MHCP explained:
I use humor a lot. I try to meet people where they are. I know lots of those guys don't want to talk about their emotions, so I can make jokes ‘You don't want to talk about your emotions? So let's talk about not talking about your emotions.’ You know, so I think humor is a good door in. And not all of them are accessible, but they're there. By the time they get through my door they're already open enough to recognize that they need to talk to somebody. (participant 19)
Empowering and giving control
Given the number of external stressors farmers face, MHCPs tried to help them regain a sense of control in their lives. Many invited farmers to describe their farm and lifestyle, allowing farmers to teach them something or providing space in their session for sharing information. One therapist mentioned:
You don't have to know everything about farming, but you have to be genuinely curious without judgment. I used to think they were just all called cows. That's how little I knew about cattle farming before my client explained what he was dealing with. (participant 24)
Others encouraged their clients to take an active role in treatment decisions. One therapist explained:
I think one of the things is letting them know they are in full control over how quick or how slow we go. And a lot of times farmers don't want to waste a lot of time, but they also don't want to be opening up and spilling out everything either. So it's having that balance and letting them know, if you don't want to answer that's okay. (participant 5)
Validating stress
Participants emphasized the importance of reassuring farmers that they are not alone in their experiences, acknowledging the difficulties of seeking therapy, and validating their specific stressors and challenges in farming life. One MHCP explained:
I can't be like, ‘I just talked to a farmer two hours ago about the same problem’ but rather I’d say ‘this is something I hear commonly’. I just try to normalize their issues because everybody feels like they're alone. (participant 15)
Participants mentioned their clients valued having someone acknowledge that there are a lot of moving pieces in farming, and many wanted to feel seen. One therapist mentioned, ‘Generally speaking, almost all of my clients are looking for a level of respect, care, and understanding with their difficulty’ (participant 14).
Providing psychoeducation
Most participants described that their clients lacked emotional awareness and the language to express their feelings even though ‘their emotions weren’t buried deep’ (participant 7). As a result, many tried to equip farmers with emotional literacy skills and tools. Several MHCPs used analogies to relate emotions to familiar farming concepts, such as explaining anxiety by how a horse might display its anxiety. Others recommended brief online videos or podcasts that explained emotions, which farmers could listen to further understand their emotional experiences. One participant explained:
I find that even just explaining to people how the brain works, and, … how our body reacts when you've had something traumatic happen to us normalizes the kind of the stuff that they're feeling and thinking and then all of a sudden, they don't feel like they're going crazy anymore. (participant 8)
Other common farm-based analogies compared chronic stress to running a tractor without enough oil, so just as equipment wears down without proper maintenance, the body and mind can also break down if stress is not managed. This reinforced that addressing stress is a form of responsible upkeep rather than a weakness. Other therapists used tools such as emotion wheels or rating scales to help farmers identify and describe their emotions. One participant explained:
I tried to get [the husband] to understand that for his wife, it's important to hear his emotions, and because he's devoted to his wife, he tries really hard. So on each end table is an emotion sheet. Sometimes I will say ‘Just pick up the sheet and see if you can figure out what [the emotion] is.’ That can sometimes be a long process. (participant 19)
Tailoring therapy and sustaining connections
After trust was established, therapy needed to be tailored for farmers in ways that were practical, action-oriented, and grounded in their everyday lives. Many MHCPs used barns as therapeutic spaces, integrated horses or cattle into sessions, and went for walks instead of sitting in an office. Several MHCPs explained that tailored approaches facilitated deeper emotional exploration and healing. One explained:
I'm going into private practice and I am doing therapy in a barn. We're building it. And it's all made out of wood from the farm. So it's history, and generations. So when they come to therapy, they come to a ‘farm’. (participant 3)
Therapists also tailored their questions to discuss mental health issues in ways that were comfortable for farmers and used non-stigmatizing language. For example, one participant explained, ‘I avoid certain words, like "self-care". So, I’d ask ‘With everything that needs to be done on the farm, what do you do to take care of you?’’ (participant 5). Others mentioned that knowledge of farm culture helped to structure questions in ways that resonated with farmers. For example, one participant mentioned, ‘I might ask a farmer "What do you do when it rains?" I think it's a good question’ (participant 7). This question acknowledges the importance of rain in farmers’ lives, but as rain often signals that outdoor work slows down, this question can provide a way to explore how a farmer copes.
Because farming involves seasonal work, participants mentioned their clients rarely maintained a regular therapy schedule. As such, many participants developed actionable post-therapy plans with their clients so that therapeutic activities could be integrated into daily farm routines (eg listening to podcasts or music while driving the tractor) or keeping a journal in the tractor to write ideas and thoughts. One participant explained:
I find practical strategies work well … I recommend that if they have a spot, even in the tractor, if they're the only person that uses that tractor, they can keep a notepad and jot things down when those thoughts are going around their heads. And especially if you're seeding for quite a few hours, which means it's just you alone with your thoughts. (participant 20)
Generating a visual framework
We translated the themes into a conceptual framework, called the Farmer-Centered Therapy Framework, to illustrate the strategies MHCPs use to foster therapeutic alliance with their clients. As shown in Figure 1, this process involved five consecutive steps, with each building upon the next. The framework represents a descriptive, participant-grounded visual summary of the themes. We refined the step labels to emphasize the specific therapeutic actions described by participants rather than serving as direct one-to-one reproductions of the original theme titles. While all of the steps are depicted as the same height, it is possible that certain steps are more challenging than others and would be visually depicted as a taller step. For example, building trust was considered a major milestone. The potential barriers associated with each step, and therefore the issues that could thwart the therapeutic process, are presented on the diagonal in the darker shaded areas.
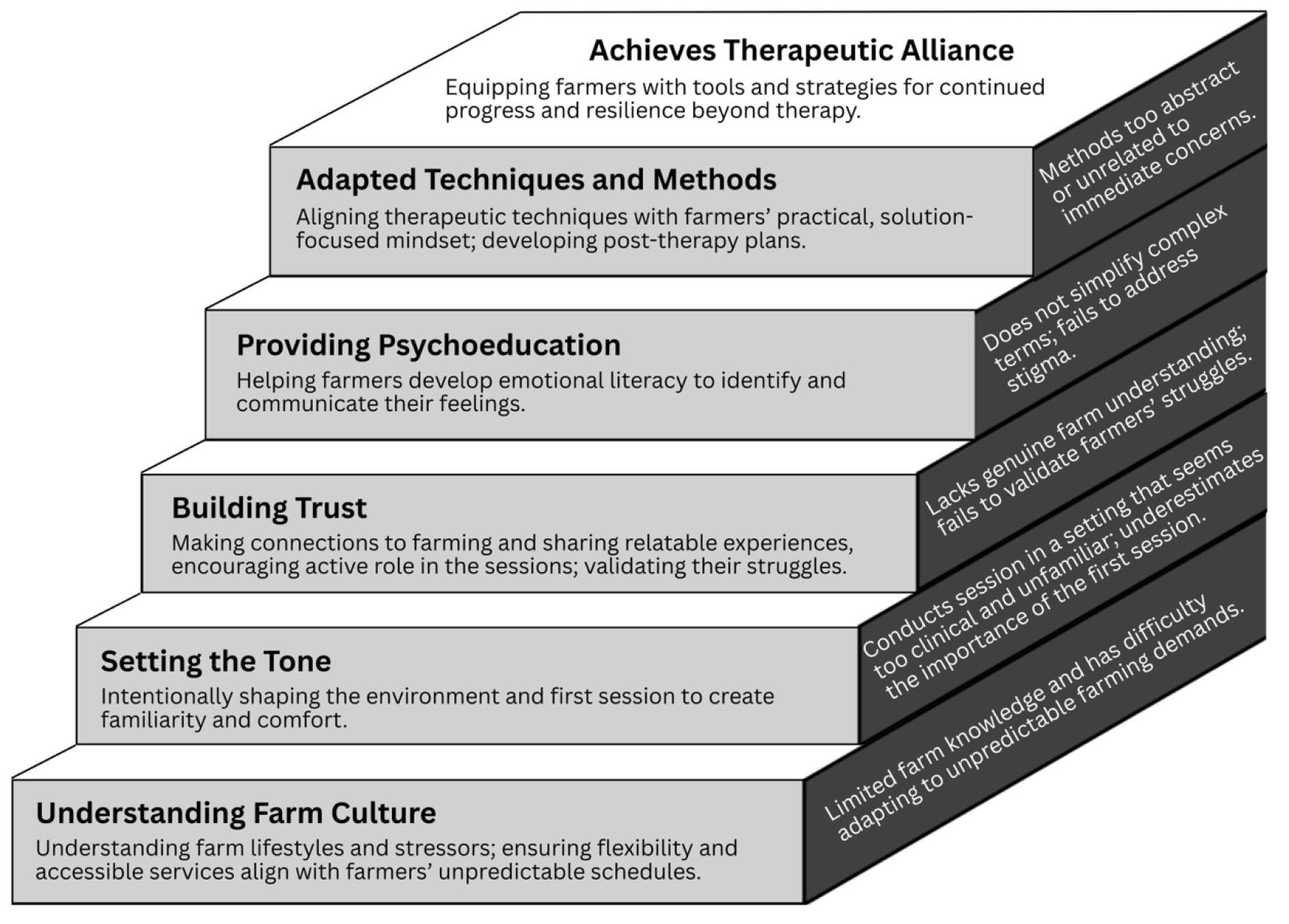 Figure 1: Farmer-Centered Therapy Framework, showing the steps for fostering therapeutic alliance with farmer clients as well as potential barriers at each step.
Figure 1: Farmer-Centered Therapy Framework, showing the steps for fostering therapeutic alliance with farmer clients as well as potential barriers at each step.
Discussion
Providing mental health care to rural and remote communities, particularly farming populations, is challenging due to cultural norms of self-reliance and privacy, mental health stigma, and isolation. By exploring the perspectives of MHCPs who work with farmer clients, our findings highlighted the importance of providing care that aligns with the rhythms and values of farm life. Our findings build upon research on rural mental health that emphasizes the need for flexible, culturally sensitive models of care to effectively engage hard-to-reach populations.
A foundational understanding of farm culture, such as understanding the unique stressors, appreciating the values, and acknowledging mental health stigma, enabled MHCPs to use relatable language and validate farmers’ experiences. This supports previous research that farm culture knowledge is essential for building rapport12,19,20,28,29. For example, Canadian farmers in two studies expressed hesitation to work with providers who lacked any knowledge of farming12,20. Likewise, a mixed-methods study of Australian farmers reported that the farmers preferred MHCPs who had some understanding of the agricultural industry7. Our findings emphasize that access is not only geographic, but that cultural access matters just as much. Therefore, improving rural mental health access for farmers requires attention to relational and cultural aspects of care, as well as the geographical distribution of services.
A crucial part of forming trust with farmer clients was considering the environment, as reflected in the theme of setting the tone. Participants described designing a welcoming and relatable environment for their farmer clients, including farm-based offices, going for walks, adjusting their level of formality, and greeting clients with a handshake. Our findings align with previous research that showed therapeutic spaces can impact clients’ perceptions of the therapist and treatment engagement30,31, and even whether the client continues therapy32. For example, a study of therapy clients described a preference for spaces that felt like traditional living room settings with lived-in furniture, personal items, and dim lighting31. These spaces also provided impressions about the character and expertise of the therapist, especially whether the therapist would understand them31.
Although future research should examine the extent to which modifying the therapeutic space helps farmers feel more relaxed, return for another session, and engage more during therapy, the idea of using the physical environment to set the tone for therapy is supported by several theories33,34. For instance, a client who experiences their home as a safe place may have a positive association, and feel at home, in an office space that is designed in a similar manner. For farmers who are low help-seekers and unfamiliar with sharing emotions, adjusting the physical space to enhance their comfort level may be a critical component to building trust. However, trust-building takes time and flexibility, and standard service models that provide short-term treatment (eg four to six sessions) or highly standardized care may be poorly aligned with the time and relational investment required for MHCPs to engage farmers effectively. Clinical practices may need to explore alternative service design and delivery models that support low help-seeking populations, such as farmers.
Many MHCPs noted their clients had limited emotional and mental health literacy, which required adapting standard counselling approaches, using structured tools, and farm-related analogies to help clients recognize and articulate what they were feeling. The use of metaphors in therapy is well documented35-37. Moreover, this approach aligns with broader research on the need for mental health literacy programs tailored for agricultural communities. For example, programs such as In the Know have reported significant improvements in participants’ knowledge about mental health, confidence in recognizing distress, and willingness to talk about mental health with others38. Another skills-based mental health literacy program in New Zealand, called GoodYarn, has shown significant similar improvements in participants’ awareness, confidence and knowledge39. While psychoeducation may be a valuable tool to incorporate into therapy with farmers, future research needs to examine how it impacts clients’ treatment outcomes.
Implications for practice
Our findings highlight the need for rural mental health policy to improve access, cultural responsiveness, and service delivery of mental health initiatives in rural farming communities. For example, policy changes could support developing and funding training programs that equip rural MHCPs with a better understanding of farm culture, values, and stressors40. This could include integrating farm-specific case examples into existing curricula, ensuring continuing education is available for those working in rural settings, and requiring that MHCPs who respond to crisis calls from farmers receive farm culture training first. The National Farmer Wellness Program in Canada provides free crisis counselling to farmers and requires all MHCPs to be trained in farm culture41.
Policy implications include the need for extended therapy support to address financial barriers and account for the time it takes for farmers to build trust with their MHCP. Participants noted it took approximately three sessions for their clients to feel comfortable opening up. A review of services across Canada showed that free counselling for farmers was offered in only five (38%) provinces or territories, ranging from six free sessions to unlimited counselling hours. Given that a single 50-minute session from a certified counsellor, registered social worker, or registered psychologist can range from C$125 (A$127.50) to C$225 (A$229.50)42, accessing ongoing mental health support on their own may be out of reach for many farmers. Policy initiatives aimed at supporting farmer mental health need to account for the longer engagement period often required to establish therapeutic alliance.
MHCPs who want to support farmers should educate themselves about farm culture to enhance their credibility with their clients and step outside their own worldviews to understand diverse perspectives for culturally responsive care40,43. Organizations such as the Canadian Centre for Agricultural Wellbeing and the Australian National Centre for Farmer Health provide training opportunities for MHCPs seeking to improve their understanding of farm life and learn ways to adapt their clinical approaches.
A useful point of comparison is Gardner’s levels of engagement22, which depict therapeutic relationships as progressing through increasing levels of connection, from initial friendliness and engagement to a deeper therapeutic alliance. While these levels outline the broad stages through which alliance may develop, they offer limited guidance on the specific strategies MHCPs use to move through these stages or the barriers that may cause engagement to stall, especially in farming contexts. Our Farmer-Centered Therapy Framework builds upon Gardner’s work by offering a practical, evidence-based guide for MHCPs working with farmer clients. Our framework emphasizes how key components work together to support culturally responsive care, which is necessary for establishing therapeutic alliance21. Moreover, the stepwise nature of our framework highlights that reaching therapeutic alliance with farmers is an ongoing process rather than a single adjustment. While the framework can serve as a training tool for rural MHCPs, it can also guide future research to understand the treatment outcomes of culturally adapted interventions for the agricultural community. Also, the framework may be transferable beyond farming. Our findings may inform engagement approaches with other rural and remote populations for whom privacy, stigma, self-reliance, and identity shape help-seeking.
Limitations
We used convenience sampling, which affects the generalizability of our findings. Most participants had a background in farming, but the extent of their involvement varied and was not systematically assessed, which potentially influenced their perspectives on farmer clients. Also, the sample consisted mainly of women (72%). Although this gender breakdown reflects the demographics of the counselling profession, we were limited in examining potential gender differences among therapists. Future research should validate the Farmer-Centered Therapy Framework with more diverse samples. While many of our participants had a background in agriculture, future research should validate this framework with farmers. Also, the coding process was conducted by researchers with varying familiarity with farming culture. Incorporating analysts without farming backgrounds could offer other perspectives and reduce potential biases introduced by familiarity with the topic.
Conclusion
Beyond ensuring access, mental health care to farmers requires cultural understanding, trust, and tailoring. From using relatable language to designing familiar spaces and offering practical tools, MHCPs used a range of strategies to reach therapeutic alliance with a population that has historically been hesitant to seek help. For rural and remote communities, where mental health services may be limited and stigma remains present, our findings offer insights for encouraging the uptake and retention of therapy. Policies, training programs, and services must be tailored to the cultural context of farming to improve the mental health outcomes.
Funding
This study was funded by a Sustainable Canadian Agricultural Partnership grant awarded to the Agricultural Research and Extension Council of Alberta through the Alberta Minister of Agriculture and Irrigation (RES0061171).
Conflicts of interest
The authors declare that they have no affiliations with or involvement in any organization with any financial interest (eg honoraria, awards or grants) and have no personal or professional relationships related to the subject matter discussed in this manuscript.
AI disclosure statement
No generative AI or AI-assisted artificial tools were used in the conduct of this research or the preparation of this manuscript.
References
You might also be interested in:
2014 - Acute diarrhea demanding hospitalization in rural India