



Introduction
The United Nations Convention on the Rights of the Child, in article 24, defines the right to health as the right of the child to the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness1. As a signatory, Australia recognises the right of every child to good health and bears the responsibility to advance this health right through legislative measures, policy development, and strategic planning, thereby incrementally ensuring universal and equitable health coverage. Oral health is a vital component of overall health and wellbeing and should be fully considered in the roadmap towards achieving health equity2. Australia’s key policy for children’s dental health, particularly for disadvantaged families, is the Child Dental Benefits Schedule, a federal means-tested program offering children aged 0–17 years capped benefits for basic dental services including examinations, X-rays, cleaning, fissure sealing, fillings, root canals, extractions, and partial dentures3. The National Oral Health Plan also targets priority groups, including low-income families and those in remote areas, aiming to reduce oral health inequities4.
While the overall oral health of Australian children has improved, certain identifiable groups continue to experience a disproportionate burden of oral disease5,6. Children in rural areas experience poorer oral health-related quality of life and higher caries risk than those in metropolitan areas6. The National Child Oral Health Study (2012–14) reported caries in primary teeth in 53% of children in remote/very remote areas versus 39% in major cities7. Consistent with this, dental visiting in 2023–24 was lower outside metropolitan areas (55.3% in major cities v 46.2% in outer regional, remote and very remote regions)8. Disparities are particularly pronounced for Aboriginal children, who experience dental caries threefold higher than non-Aboriginal children6, and a substantial proportion reside in rural and remote Australia (19.0% in outer regional areas and 15.4% in remote/very remote areas)9.
In Australia, rural and remote settings are commonly defined using the Australian Statistical Geography Standard Remoteness Areas (RAs), which classifies locations into five categories based on the Accessibility/Remoteness Index of Australia Plus (ARIA+). This index fundamentally measures remoteness as a proxy for access to essential services by calculating the road distance from a given location to various population centres. The classification moves from Inner Regional (RA2) and Outer Regional (RA3), which experience moderate service access, to Remote (RA4) and Very Remote (RA5), where the greatest geographic distance is associated with the lowest levels of service availability10.
Poor oral health in rural and remote areas is a complex issue driven by limitations in dental care access4,8. Evidence indicates that improving access to primary care results in better health outcomes and reduces preventable hospitalisation4,11. In health services and policy research, access is commonly conceptualised using the Penchansky and Thomas (1981) framework, which comprises five dimensions12:
- availability – refers to the adequacy of dental service supply in relation to needs
- accessibility – addresses the geographic proximity of services
- accommodation – involves health services organisations and responsiveness to meet the population’s needs and preferences, including appointment flexibility, and culturally appropriate delivery for Indigenous and non-Indigenous populations13
- affordability – considers direct and indirect cost of services, including travel and lost income14
- acceptability – concerns the compatibility between patients' expectations and providers’ attributes, including cultural sensitivity, trust in the healthcare system, and the comfort level experienced during interactions15,16.
In rural and remote Australia, children and their families face compounded barriers across these dimensions, contributing to persistent oral health disparities. Addressing these disparities requires a comprehensive understanding of the influencing factors. This systematic review applied an ecological model, exploring barriers at system, policy, community and individual levels that influence regular dental visits. In public health research, an ecological model is a framework that explores the complex interplay of various factors influencing health and wellbeing at multiple levels. It emphasises that health behaviours are not solely influenced by personal characteristics but are also shaped by community, policy and organisational factors17. We aim to synthesise the existing literature, using a mixed-methods approach, to identify multi-level barriers and propose evidence-based solutions tailored to the unique challenges of these communities.
Methods
We conducted a mixed-methods systematic review, incorporating qualitative, quantitative and mixed-methods studies to yield complementary insights, as studies focus on different aspects of the phenomena of interest: barriers to oral care. Quantitative studies, such as cross-sectional or cohort designs, established patterns and prevalence of dental utilisation within specific populations. Conversely, qualitative data derived from methods like focus groups and interviews offered in-depth explanations for these observations. This convergent, integrated approach facilitated a comprehensive, pooled synthesis of the diverse data types18. Detailed findings were derived through this integrated mixed-methods approach, which specifically addressed the research question by transforming quantitative outcomes into qualitative interpretations. The ultimate synthesis is presented in a narrative format. This review follows the Joanna Briggs Institute (JBI) methodology for mixed-methods systematic review18. A protocol for this review was developed and registered in the PROSPERO systematic review registry (CRD420250625809).
Search strategy
First, we conducted a preliminary search of MEDLINE and Scopus to identify keywords from relevant titles and abstracts. Then, we used these keywords and Medical Subject Headings (MeSH) terms to develop a full search strategy for MEDLINE, which was customised for each database. We conducted the final search across MEDLINE (via Ovid), Scopus and Web of Science between December 2024 and January 2025 using the following MeSH and keywords: [(Austral* or qld or Queensland or new or 'New South Wales' or vic or Victoria or tas or Tasmania or sa or 'South Australia' or wa or 'Western Australia' or nt or 'Northern Territory' or act or 'Australian capital territory') AND ("rural areas" or "rural regions" or "remote areas" or "remote regions" or "rural Australia" or 'geographic perspective') AND (children or child* or adolescent or adolescence or teenager or teenagers or 'paediatric patients' or childhood or 'Aboriginal children' or 'Torres Strait Islander children' or Indigenous) AND ("oral health" or dentistry or dental or "dental care" or "oral care" or "oral health services" or "dental services" or "dental treatment" or "oral treatment" or "emergency care")] (Supplementary figure 1). We complemented the database search with hand-searching in Google Scholar, and on relevant website, including the Australian Institute of Health and Welfare, Australian Bureau of Statistics, and WHO. Additionally, we screened the reference lists of included articles for additional relevant articles. We applied no publication-date restrictions, as barriers to oral health care in rural and remote communities represent a longstanding structural issue rather than a recent phenomenon.
Selection criteria
In accordance with the JBI guidance, we structured our review question using the PICO (population, intervention, comparison, outcome) framework. The population of interest comprised children and their families. The phenomenon of interest focused on the barriers affecting access to oral health service, and the context was rural and remote communities across Australia. The review includes both Indigenous and non-Indigenous Australians. We did not apply any age limits, but we focused on children’s access to dental care. We excluded letters to the editor, conference abstracts, opinion articles, studies conducted outside Australia, and articles that focused on medically compromised individual in rural communities.
Study selection
We exported all retrieved articles that met inclusion criteria into Covidence, and removed duplicate records. Two authors independently screened the titles and abstracts in Covidence for inclusion of relevant studies, followed by a full-text assessment based on the predefined inclusion and exclusion criteria. We documented the reasons for exclusion during full-text screening in the PRISMA diagram. A third author resolved any disagreements through discussion. The results of the full search and the article inclusion process were reported in the PRISMA flow diagram (Fig1)19.
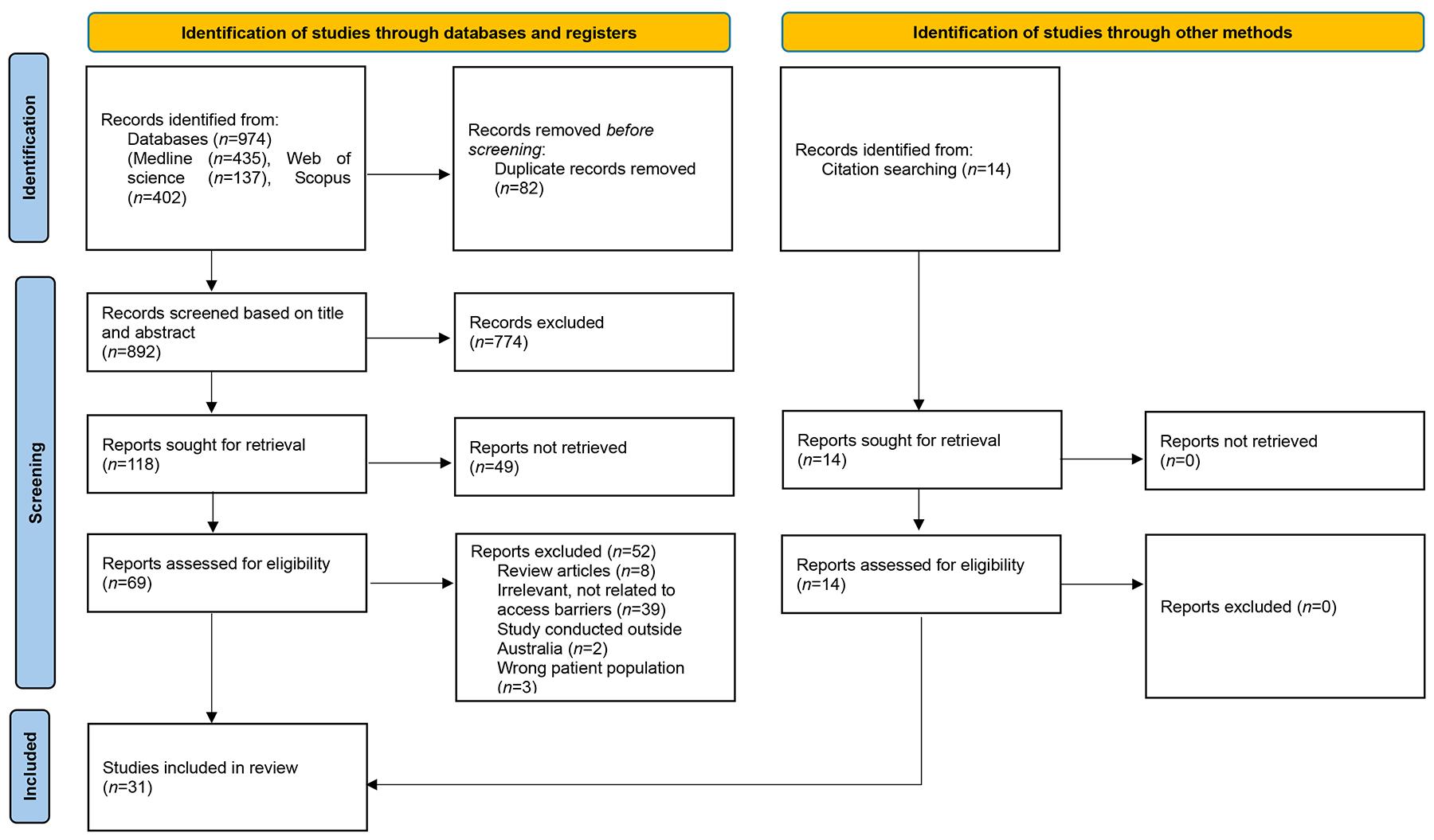 Figure 1: PRISMA flow diagram of full search and article inclusion process.
Figure 1: PRISMA flow diagram of full search and article inclusion process.
Assessment of methodological quality
This systematic review used the JBI critical appraisal tools20. We appraised quantitative studies, including the quantitative component of mixed-methods studies, using the JBI critical appraisal checklist for analytical cross-sectional studies. We evaluated qualitative studies, including the qualitative component of mixed-methods studies, using the JBI critical appraisal checklist for qualitative research. Using the checklist responses ‘yes’, ‘no’, and ‘unclear’, we critically appraised all studies, regardless of methodological quality. Two reviewers independently completed the critical appraisal and a third author resolved any disagreements through discussion.
Data extraction
Two independent reviewers extracted data for all included studies in Covidence, following a convergent integrated approach18. The research team developed a customised data-extraction template to guide the process, track key information efficiently, identify emerging themes relevant to the review question, and organise all extracted data. We extracted study characteristics including first author, year of publication, state/territory, study design, study setting, sampling technique, and participants’ information (age, sample size, Indigeneity, and gender). We also recorded levels of impact at which barriers were reported.
Data transformation
We transformed quantitative data into qualitised data. This involved transformation into narrative interpretations of the quantitative results. We applied this same transformative approach to the quantitative aspects of mixed-methods studies.
Data synthesis and integration
This review used a convergent integrated approach for data synthesis, following the JBI methodology for mixed-methods systematic reviews18. We assembled and pooled the qualitised data from transformed quantitative studies together with the qualitative data. Then, we categorised the synthesised results and linked them based on similarity in meaning to construct a cohesive argument. This synthesis of findings yielded a comprehensive overall analysis.
Ethics approval
We conducted this systematic review in compliance with the guidelines and standards established by the Committee on Publication Ethics. Given the nature of the study, we did not require ethics approval from institutional ethics committee.
Results
Our search identified 974 articles. We removed 82 duplicates and screened the remaining records. Subsequently, we excluded 774 articles based on title and abstracts screening and a further 49 papers after full-text review. This process resulted in 17 studies that met the inclusion criteria. Although we searched Google Scholar, Australian Institute of Health and Welfare, Australian Bureau of Statistics, and WHO resources, none of the records identified through these resources met the inclusion criteria. We identified an additional 14 studies through citation searching of the included articles, bringing the final number of included studies to 31 (Fig1). These studies form the foundation for the systematic assessment of barriers to accessing oral health services in rural and remote Australia.
Study characteristics
Included studies were geographically diverse, spanning multiple Australian states and territories, including New South Wales, South Australia, Western Australia, Victoria, Northern Territory, Queensland (Fig2). Studies used a range of methodologies, involving qualitative interviews/focus groups, cross-sectional surveys, prospective cohort designs, secondary analysis of large administrative datasets, mixed-methods and descriptive case studies. Participants included non-Indigenous and Indigenous children and their carers, community members, and healthcare/dental professionals working in rural and remote communities. Age eligibility varied from paediatric samples (≤15 years) to adult samples of 18–98 years. Sample sizes ranged from small qualitative samples (eg 12 interviewees) to very large population-based datasets (eg 43,937 hospitalised children) (Table 1). Almost all included studies employed appropriate research methodologies. The assessment indicated that only one study had a high risk of bias21. Twelve studies were assessed as having a moderate risk of bias2,5,13,22-30, and 18 studies had a low risk of bias14-16,31-45. Five studies did not report confounding variables2,5,21,24,29, seven qualitative studies failed to locate the researcher culturally or theoretically13,22,23,26-28,31 and seven studies didn’t describe the influence of the researcher on the research13,22,23,26-28,39. The detailed results of the quality assessment are presented in Supplementary table 1 and Supplementary table 2.
Table 1: Descriptive characteristics of included studies
| Authors, year of publication | State/territory | Study design | Setting | Sampling technique | Participants | Age (years) | Total sample size | Indigenous status (Aboriginal or Aboriginal and Torres Strait Islander) | Gender | Barrier level |
|---|---|---|---|---|---|---|---|---|---|---|
| Gardiner et al, 20205 | Victoria NSW, NT, WA | Prospective cohort study | Rural and remote regions with a Royal Flying Doctor Service Dental service within a 60-minute drive time | Royal Flying Doctor Service dataset | All patients who accessed an Royal Flying Doctor Service dental clinic in rural and remote regions | 1–85 or more; mean age 31.5 (standard deviation 24.8) | 3407 patients | 27% Indigenous, 43% non-Indigenous, 30% patients had missing data for ethnicity | 33% men, 38% women, and 29% of unknown sex | System level |
| Barnett et al, 201523 | Queensland | Qualitative semi-structured individual and group interviews | Four remote communities in outback Queensland, Australia in which there was no resident dentist/dental surgery | Purposive and snowball sampling strategies | Primary and oral healthcare providers with experience in oral care in rural and remote communities | 18–40 or more | 35 primary care providers (12 GPs, 6 pharmacists, 4 practice manager, 3 child health nurse or nurses, 3 managers/directors of nursing, 3 receptionists, 3 medical students, 1 speech therapist) 4 dental care providers (3 dentists, 1 dental nurse) | nr | 24 female and 15 male | System, policy, community, individual levels |
| Alsharif et al, 201445 | WA | Cross-sectional study | Records of hospitalised children because of oral-related conditions | Western Australia Hospital Morbidity Dataset | Child under the age of 15 years diagnosed and admitted for an oral health condition in WA for the study period | 0–14 | 43,937 children | 5% (2,119)were Indigenous children, 41,818 non-Indigenous children | nr | System level |
| Jean et al, 20202 | National | Cross-sectional study | Public dental clinics providing services for children | Publicly available information on government health service websites | All residents under 18 were included in the study in line with the UN Convention on the Rights of the Child definition of a child | <18 | nr | nr | nr | System level |
| Barnett et al, 201726 | Queensland, SA, Tasmania | Qualitative semi-structured individual and group interviews | Rural communities across three Australian states. Classified as RA2 (Inner Regional Australia), RA3 (Outer Regional Australia), RA4 (Remote Australia) or RA5 (Very Remote Australia) by the Australian Standard Geographical Classification Remoteness Areas | Purposive and snowball sampling strategies | Primary care providers and dental practitioners in rural and remote areas | Mean age 40 | 14 communities identified in the study. 105 primary care providers (1 speech therapist, 3 allied health workers, 3 Aboriginal Health Workers, 21 child health nurses or nurses, 12 directors of nursing, 30 GPs, 19 pharmacists, 9 practice managers, 7 receptionists) 12 dental providers (8 dentists, 1 dental therapist, 2 dental assistants, 1 practice manager) | nr | 74 (70%) female, 31 (29.5%) male | System, policy, community, individual levels |
| Patel et al, 202140 | WA | Qualitative individual interviews and yarning groups | East Kimberley region of WA | Purposive sampling with the assistance of Aboriginal liaison officers enabled invitation of participants leading to a heterogenic sample | Aboriginal adults over 18 and living in the Kimberley region of WA | >18 | Total of 80 participants 23 individual interviews and 17 yarning groups | Aboriginal | 27 males, 53 females | System, policy, community, individual levels |
| Marino et al, 202142 | Victoria | Cross-sectional study including face-to-face survey and clinical assessment of oral health | Regional centre and three adjacent shire capitals in the Goulburn Valley of regional Victoria | Randomly selected households | Population living in the Goulburn Valley region of Victoria | Mean age 58.6 (standard deviation 16.3), ranging from 18 to 98 | 574 participants | nr | 55.3% female, 44.7% male | System, individual levels |
| Irving et al, 201724 | NSW | Cross-sectional survey | Northern Central Tablelands of NSW | All Aboriginal children attending the new collaborative oral health service in the communities were eligible for participation in the study | Aboriginal children aged 4–14 attending the new collaborative oral health service in the community | 4–14 | 49 children aged 4–14 participated in the study (with parents/guardians) | Aboriginal children | 63% female, 37% male | System, individual levels |
| Barnett et al, 201628 | Queensland, Tasmania, SA | Qualitative face-to-face semi-structured interviews | Rural and remote communities in which oral health care was a significant problem, and where there was no resident dentist | Purposive and snowball sampling strategies | Primary care providers in remote communities, who had experience in advising patients with oral health problems | Mean age 40 | 16 communities were identified by state dental officers for inclusion, and 30 GPs | nr | 22 male, 8 female | System, policy, community, individual levels |
| Gussy et al 200631 | Victoria | Qualitative focus group discussions and semi-structured interviews | Four rural, non-fluoridated local government areas in Victoria | Purposive and snowball sampling strategies | Maternal and child health nurses, GPs, dental practitioners (dentists, dental nurses, and dental practice managers), and paediatricians | nr | A total of 56 participants (18 maternal and child health nurses, 9 GPs, 7 paediatricians, 22 dental professionals) 11 focus groups and 5 semi-structured interviews | nr | nr | System, policy, individual levels |
| Tynan et al, 202236 | Queensland | Qualitative focus group discussions and semi-structured interviews | Rural community in Queensland with a predominantly Aboriginal population | Participants were purposively recruited from established health and community groups. | Community members and community leaders of Aboriginal and Torres Strait Islanders who were engaged in health and community groups | nr | 27 participants. 12 in depth-interviews and 3 focus groups | Aboriginal and Torres Strait Islanders | nr | System, policy, community, individual levels |
| Jamieson et al, 200827 | SA | Qualitative focus group discussions | Rural community of Indigenous Australians in mid-north region of SA | participants were chosen purposively, in a strategic manner, to capture the diversity and breadth of oral health knowledge across different age-groups and cultural backgrounds in the community with relative homogeneity in regard to age and background | Members of a local Indigenous arts and crafts group, a diabetes awareness group that operated through the Aboriginal-owned health centre, a young mothers’ Indigenous childcare group and a group of Indigenous Healthcare Workers | 21–72 (female), 55–65 (male) | 34 participants | Indigenous | 30 female, 4 male | System, community, individual levels |
| Walker et al, 202316 | Queensland | Qualitative semi-structured individual and group interviews | A small, rural Indigenous community in Queensland with 1300 people | Purposive and snowball methods | Rural Indigenous community members | Four participants aged 18–39, with the remaining 23 aged >40 | 27 community members. Three focus groups and 12 in-depth interviews were completed | 95% Aboriginal and 2.5% identifying as both Aboriginal and Torres Strait Islander | 10 male and 17 female | System, policy, community, individual levels |
| Toh et al, 202237 | National | Secondary analysis of data from the Longitudinal Study of Indigenous Children | Data from the Longitudinal Study of Indigenous Children, a longitudinal population-based cross-sectional study in Australia. Covers all of Australia's states and territories, inclusive of urban, regional and remote areas | A cluster sampling technique was used to select geographic sites. Data were collected from primary caregivers | Australian Indigenous children | nr | 1258 children | 87.1% Aboriginal children, 6.8% Torres Strait Islander, 6.1% Aboriginal and Torres Strait Islander | 49.1% male, 50.1% female | System, individual levels |
| Dickson-Swift et al, 202329 | Victoria | descriptive design and case study | Rural Victorian towns with over 1000 population (Barwon Southwest, Loddon Mallee, Hume, Gippsland and Grampians) | nr | Rural Victorian towns with over 1000 population that did not have water fluoridation | N/A | 66 towns | N/A | N/A | Policy level |
| Jones et al, 201639 | SA | Qualitative semi-structured interviews | People referred for oral care through the Aboriginal Liaison Program of the SA Dental Service | Purposive sampling method | Aboriginal population eligible for publicly funded dental care | nr | 49 participants | Aboriginal | 18 males. 26 females | Policy, individual levels |
| Ellershaw, 200521 | National | Cross-sectional survey | National Dental Telephone Interview Survey 2002 | Random sample. Records were stratified by state and region and a random sample of telephone numbers were selected from each stratum | Residents from all states and territories of Australia | ≥5 | 7312 participants | nr | nr | System level |
| Dimitropoulos et al, 201825 | NSW | Quantitative cross-sectional study | Schools and local health centre for Aboriginal communities in three small, rural and remote communities | nr | Aboriginal children aged 5–12 enrolled in local schools, parents/guardians, school staff and community health workers | Children aged 5–12, parents/guardians and school staff and health workers (20) | 88 children were screened and 78 completed the child's oral health questionnaire, 32 parents and/or guardians, and 37 school staff and 2 community health workers | Aboriginal children | Children(39 male, 49 female), parents/guardians (4 male, 28 female), school staff and health workers (12 male, 27 female) | System, individual levels |
| Curtis et al, 200733 | NSW | Cohort study nested within a clinical trial | nr | Self-administered questioner mailed to each study participant within 1 month of recruitment into the clinical trial | Patients recruited for clinical trial study | 43–46 | 823 participants | nr | 57% female in major city, 63% female in regional area, 47% in remote area | System, individual levels |
| Simmons et al, 200632 | Victoria | Cross-sectional study using qualitative and quantitative methods, face-to-face and self-reported household survey | Household in regional (rural) centre and surrounding smaller towns in rural Victoria | Stratified random sampling design | All members of the household were invited to participate | ≥16 | 3172 participants from regional centre; 3144 from shire capitals (small towns) | European descent, Aboriginal, and Iraqi | 56.7% female | System, policy, individual levels |
| Adams et al, 200438 | WA | Quantitative cross-sectional telephone survey | Urban, rural, and remote locations in WA | Random selection of participants' telephone number using the electronic White Pages phone directory | Participants aged 60 or more, had a telephone listing, were on the State Electoral Roll and lived in non-institutionalised accommodation and who were able to speak English sufficiently | ≥60 | 2100 participants | nr | Urban: 415 female and 351 male; rural: 413 female and 345 male; remote: 239 female and 255 male | System, individual levels |
| Jones et al, 201434 | SA | Quantitative cross-sectional survey | Rural-dwelling Indigenous Australians | Convenience sampling | Aboriginal or Torres Strait Islander aged 17 or older living in a regional centre about 230 km north of Adelaide, the capital of SA | ≥17; mean age 38 | 468 participants | Aboriginal and Torres Strait Islander | 83 male, 385 female | System, individual levels |
| Jamieson et al, 200630 | NT | Quantitative cross- sectional survey | Three remote communities in the Top End of the NT | Random sampling approach | Carers of Indigenous children in remote communities in the target age range | 4–12 | 214 carers completed questionnaires for 409 children | Indigenous children | nr | Policy, individual levels |
| John et al, 201744 | NSW | Secondary data analysis of a cross-sectional survey | Rural community of Lithgow, NSW | nr | Primary school children and their parents | Children 6-13 | 667 parents completed the survey | Indigenous and non-Indigenous | 336 male, 329 female | Community, individual levels |
| Nolan-Isles et al, 202115 | NSW | Qualitative semi-structured interviews | Regional and remote communities in NSW | Snowball sampling | Healthcare delivery staff and stakeholders | nr | 31 interviews | Aboriginal and non-Aboriginal | nr | System, policy, community, individual levels |
| Kelly et al, 201413 | SA | Qualitative semi-structured interviews | SA rural and remote health services and tertiary hospitals | nr | Health professionals from urban, rural, and remote regions; patients/carers, Aboriginal Elder women | nr | 88 participants | Aboriginal and non-Aboriginal | nr | System, policy, community, individual levels |
| McBain-Rigg and Veitch 201122 | NSW | Qualitative semi-structured interviews | Mount Isa, Queensland | Interviewees were purposively chosen for their personal experiences, and ability to identify potential barriers for Aboriginal people | Aboriginal and Torres Strait Islanders people, Aboriginal Health Workers and other health professionals | nr | 12 interviews | Aboriginal and Torres Strait Islanders and non-Indigenous health workers | nr | System, policy, community, individual levels |
| Patel et al, 201535 | WA | Quantitative and qualitative cross-sectional study | Remote Kimberley region of WA | An online survey was sent to all volunteers working with the Kimberley Dental Team | Volunteers working with the Kimberley Dental Team including dentist, dental nurse, dental student, dental specialist, and other non-dental practitioner volunteers who held administrative and community liaison positions | 18–68; median age 47.5 | 42 participants | nr | 28 (68%) female, 13 (32%) male | System- policy, individual levels |
| Kruger et al, 200814 | WA | A cross-sectional survey and dental examinations was carried out | Rural and remote communities in the Kimberley region of WA | Random selection of participants through the help of workers in all the communities. Every third adult on the Kimberly Aboriginal Medical Services Council computerised health information system was listed. About 15% of the total participants were not randomly selected but attended the clinic through the publicity in each community | Adult members of four selected communities | 18–88, the mean age 41.2% (standard deviation 18.0) | 208 Aboriginal adults | Indigenous adults | 134 female, 74 male | System level |
| Crocombe et al, 202243 | National | Cross-sectional study | Three regional levels (Major city, Inner regional, Outer regional and Remote/Very remote) were used | Data from the latest National Study of Adult Oral Health (2017–18). Study participants were selected using a multi-stage probability sampling design that began with the sampling of postcodes within states/territories in Australia | Adults in major cities, regional, and remote communities | 15–60 or more | 15,731 people interviewed, 5,022 were examined | Indigenous and non-Indigenous | 50.2% female, 49.7% male | System, policy, individual levels |
| Williams et al, 201041 | SA | Cross-sectional study | Port Augusta Aboriginal community | Convenience sample, included word of mouth, attendance at health promotion sessions and community centres, the waiting room of the health service, interviews on radio, flyers, street stalls, home visits and Indigenous Health Worker contact | Indigenous, lived in the Port Augusta region and aged ≥17 | ≥17, mean age 38 | 468 participants | Indigenous adult | 36.9% female, 31.1% male | System, individual levels |
NSW, New South Wales. N/A, not applicable. nr, not reported. NT, Northern Territory. RA, Remoteness Area. SA, South Australia. WA, Western Australia.
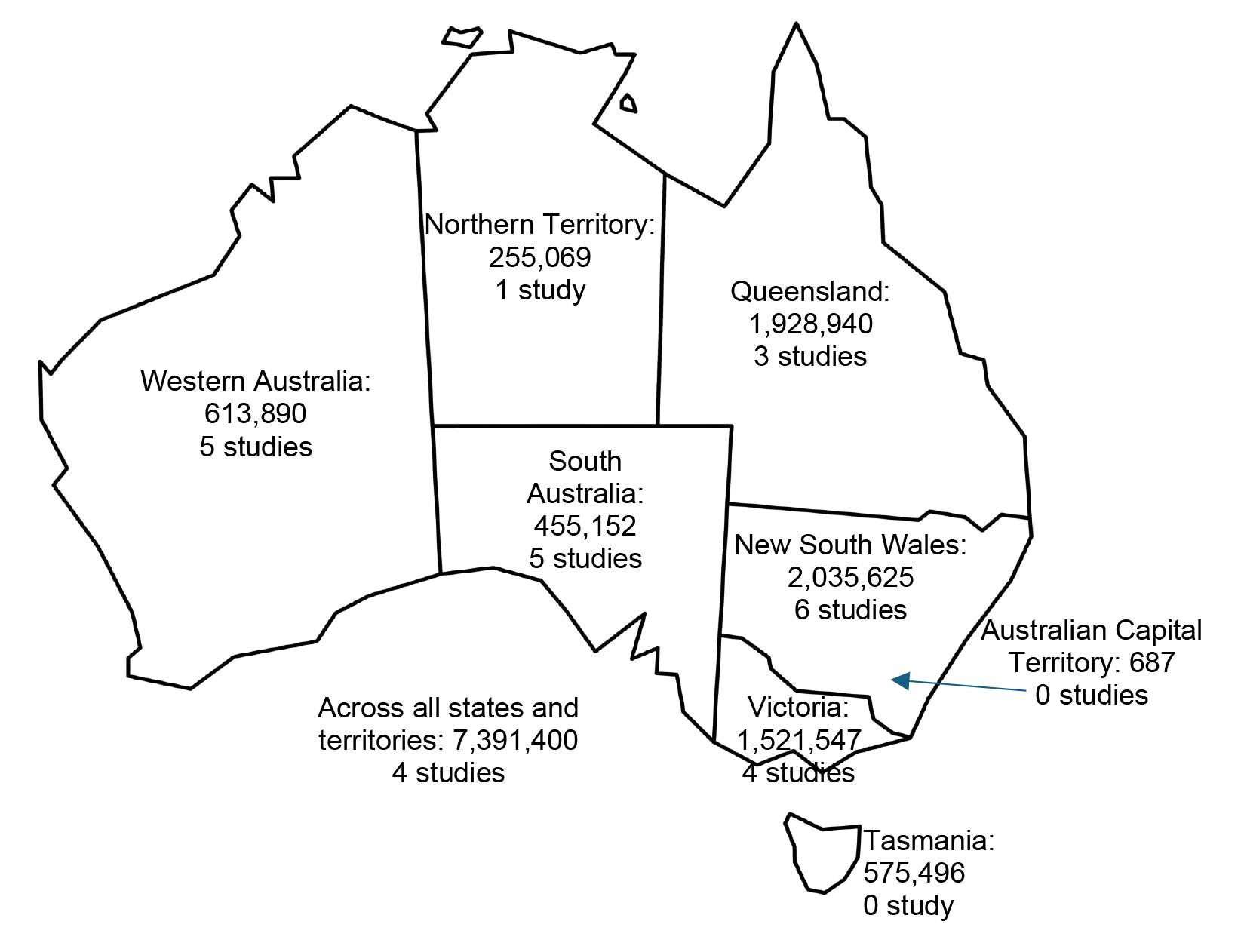 Figure 2: Estimate resident populations of rural and remote areas and number of studies reporting barriers to accessing oral health services. Population counts obtained from Australian Bureau of Statistics46.
Figure 2: Estimate resident populations of rural and remote areas and number of studies reporting barriers to accessing oral health services. Population counts obtained from Australian Bureau of Statistics46.
Synthesis of findings
It is important to highlight that the barriers to access are not independent factors; rather, they often interact with and influence one another, and their impact can vary from person to person. To capture this complexity, we developed an ecological model that illustrates the interplay of barriers across multiple levels, including system, policy, community, and individual levels (Fig3).
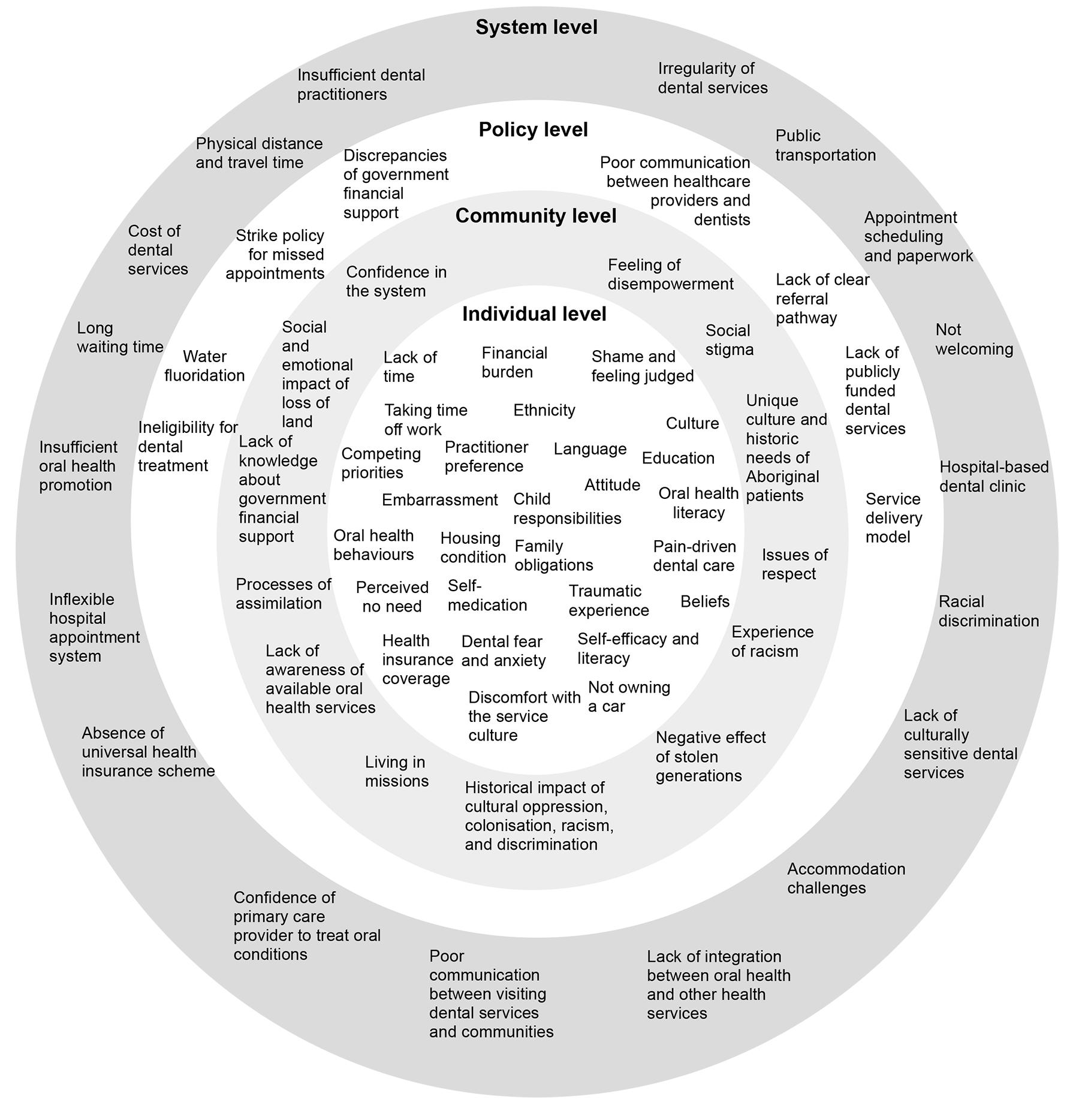 Figure 3: Ecological model of barriers to accessing oral health care in rural and remote areas within Australia.
Figure 3: Ecological model of barriers to accessing oral health care in rural and remote areas within Australia.
Potential barriers at system level
Twenty-seven studies emphasised challenges related to the health system.
Geographic location and transportation
The most frequently identified system-level barrier was the geographic location and physical distance of oral health services. Many communities in rural and remote areas lack dental coverage within a 60-minute drive, with some residents required to drive 2–4 hours to access dental services2,13-16,22-25,31-37. Compounding the challenge of distance is the issue of transportation, where personal vehicle ownership is low and public transport options are often limited or non-existent13,15,16,22-26,34,36-40. Even where community transport service exists, it presented several limitations, such as inflexible schedules, a limited number of seats allocated for dental appointments, and the exclusion of children who required car seats15,36.
Appointment systems and waiting times
Difficulty aligning appointment times with fixed public transport schedules is another challenge for rural and remote individuals accessing health services in a major city, as they must navigate two inflexible systems: healthcare scheduling and public transport timetables13,22. Additionally, administrative requirements, including paperwork and formal appointment processes, often caused patients to lose access to oral care, even when they had already organised travel and accommodation. This barrier was particularly pronounced in remote communities, where unfamiliarity with administrative procedures further impeded timely dental attendance40. Long waiting periods also emerged as significant barriers to accessing dental services24,27,31,32,36-38,40.
Cost of dental services and absence of universal health insurance coverage
Affordability of dental care is another barrier that can prevent individuals in rural and remote areas from accessing dental services14,16,21,22,24,26-28,31,32,34-39,41-43. Compounding direct costs are the substantial indirect expenses associated with accessing oral health services. These include fuel cost, potential accommodation for overnight stays, and lost income for time off work, which disproportionately burdens families13,16,22,23,26,33,36,39. Although the Patient Assistance Transport Scheme offers limited financial reimbursement, it does not cover all out-of-pocket expenses13.
Workforce
The literature extensively reported the challenges associated with the recruitment and retention of dentists in Australia’s rural communities14,23,26,35,37,43. Hence, in the absence of a resident dentist, individuals in rural and remote communities present to local hospitals, GP practices, pharmacies and Aboriginal Health Centres with a range of oral health problems23,26. However, the scope of care provided is limited to oral hygiene instructions, short-term pain relief, antibiotic prescriptions, and advice to patients to see a dentist23,26. Some primary care providers acknowledged a lack of confidence in managing patients presenting with oral health issues23,26,31. Similarly, some dentists working in these communities were reluctant to treat young children, which posed a significant barrier to timely dental care for this vulnerable group31.
Visiting oral health services
The infrequent and inconsistent provision of dental services in rural and remote areas, characterised by the absence of a fixed oral healthcare setting or consistent dental practitioners, was perceived as unsustainable and detrimental to building trust-based relationships between patients and healthcare providers15,16,22,26. Compounding this was the scarcity of community and school-based oral health promotion activities16,28,31. Jamieson et al identified five key reasons for the under-utilisation of visiting school dental services in rural and remote communities: limited community awareness of preventative dental measures, difficulties in obtaining consent for child dental care, high mobility among children, low school attendance limiting opportunities for school dental service delivery, and the short duration of school dental service visits27.
Acceptability of oral health services
A lack of culturally sensitive dental services and providers was consistently identified as a barrier to accessing oral care among Aboriginal and Torres Strait Island communities. Participants reported feeling misunderstood, judged, or disrespected by dental professionals who lacked awareness of their cultural background15,16,24,27,35,39. Furthermore, the integration of dental clinics within main hospital facilities inadvertently introduced stigma, as hospitals are often associated with illness, trauma, or negative past experiences, particularly for Aboriginal and Torres Strait Islander individuals. This can deter attendance for routine dental care35,40.
Potential barriers at the policy level
Eleven studies documented the presence of policy-level barriers to oral health access.
Government funding
The literature highlights significant discrepancies and insufficient government financial support for oral health care, compared to other health conditions, creating a major barrier to accessing dental services. Notably, many dental services also fall outside the scope of subsidised health programs16,23,35.
Ineligibility for dental treatment
The restrictive eligibility criteria for accessing public dental care, with only individuals holding government healthcare cards or concession cards qualifying for subsidised dental treatment, excludes a substantial group of individuals with low income levels who do not meet the strict criteria for these cards but still cannot afford private dental treatment27,28,39,43. In addition, the implementation of strike policies in some regions, whereby individuals are denied further appointments after two missed visits, further acts as a barrier to dental care39.
Professional communication and integration of health services
Poor interprofessional communication both between primary healthcare providers and either visiting or regional dental practitioners, and between visiting dental professionals and the local community, emerged as a significant barrier. This deficit in communication led to reduced community awareness regarding the availability of oral health services, including visiting dental services, school dental services, and the mobile dental van15,22,23,26,28. Furthermore, unclear referral pathways and the absence of structured feedback process limit coordinated patient care23,26,28. A lack of coordination and integration between oral health and other healthcare services also contributes to fragmented care, with many health practitioners not incorporating oral health consideration when diagnosing or managing systemic conditions like diabetes15,16,22.
Lack of access to water fluoridation
Studies identified limited access to water fluoridation in rural and remote communities as a policy-level barrier that contributes to higher caries risk and widens oral health inequalities29.
Potential barriers at the community level
Eleven studies present findings related to community-level barriers.
Racism and discrimination
Several studies reported that fear of racism, discrimination, judgement, disrespect, and negative government intervention act as barriers to Aboriginal and Torres Strait Islander communities when accessing health services15,24,36. Aboriginal parents also expressed concern about potential involvement from the Department of Child Services in New South Wales and about being perceived as a bad parent15.
Cultural practices
Oral health behaviours were not traditionally embedded within the lifestyle of Aboriginal and Torres Strait Islander communities, which may influence present-day practices27. Therefore, there was a lack of understanding at a community level about oral hygiene measures required for good oral health27. Also, social stigma associated with poor oral health discourages individuals from seeking timely treatment, as many avoid disclosing the condition of their mouth36.
Community awareness
Limited awareness of the location of oral healthcare services, how they operate, and what government financial support is available commonly prevents individuals from accessing dental care13,16,22,32,39.
Potential barriers at the individual level
Twenty-five studies highlight individual-level barriers as a major issue.
Parents’ knowledge and attitude
A lack of oral health knowledge and poor hygiene practices among parents22,23,26,39, in particular a limited understanding of the importance of early dental care, can delay or prevent necessary treatment for their children31. Factors such as parents’ educational levels, employment status, ethnic backgrounds, and cultural beliefs further influence their health-seeking behaviours35,44.
Low priority
Rural community members often perceive oral health as a low priority and typically seek dental care only when severe pain arises15,23-25,27-29,31,32,36-40,42-44, or when aesthetic concerns negatively affect their self-esteem and quality of life39. Also, the presence of multiple competing priorities, such as medical conditions, lack of time, family responsibilities, and other personal commitments make it difficult to prioritise or attend dental appointments13,15,32,36,38,39,42. For Aboriginal and Torres Strait Islander Peoples, cultural obligations during times of bereavement Sorry Business can also delay or prevent engagement with oral health services15.
Financial burden
Key challenges in preventing oral diseases among children in rural and remote communities are closely associated with financial constraints and broader socio-environmental factors within households30,36. Limited financial resources often restrict access to basic oral care items, such as toothbrushes and toothpaste, thereby impeding the development of consistent oral hygiene practices16,24,36. Low levels of dental insurance among children in rural and remote areas create substantial barriers to accessing care. A marked inequality in insurance coverage also emerges between Indigenous and non-Indigenous children living in these communities28,32,44,45.
Fear and anxiety
Fear and anxiety related to dental treatment, including the impact of previous traumatic dental experiences, commonly deter individuals in rural and remote communities from seeking care24,27,31,32,36,39-42. Similarly, fear of the unknown is associated with travelling outside the community for care40. Moreover, individuals from these areas expressed concerns about receiving care from inexperienced practitioners, posing an additional barrier32,40.
Shame and embarrassment
Emotional barriers, including shame, embarrassment, and guilt among parents, who feel they have neglected their children's oral health, often hinder engagement with dental care16,22,31,40.
Discussion
The current state of access to oral health services is shaped by a complex interplay of healthcare factors. To address this, our review synthesised the available evidence and categorised recurring themes related to barriers into four interconnected levels. System-level barriers included workforce shortages, limited service availability, geographic inaccessibility, and cost of services. At the policy level, disparities in funding models, fragmented services, lack of integration between oral health and general health services, lack of access to fluoridated water, and inconsistent eligibility criteria impede equitable access to dental services. Community-level barriers encompassed the unique cultural needs of Aboriginal and Torres Strait Islander patients and cultural mismatches between providers and patients, and the general lack of oral health promotions tailored to local contexts, which affected the whole community’s confidence in the health system. Finally, individual-level barriers including low oral health literacy, financial hardship, low prioritisation of dental care, and feelings of shame and fear related to dental treatment directly influence care-seeking behaviour.
Importantly, these barriers are interrelated and reinforce one another. In response to this complexity, we first developed an ecological model to visually map the interconnected nature of these barriers. Building on this, we developed a conceptual model grounded in the ecological framework to present comprehensive, evidence-based solutions at each level (Fig4). Together, these models offer policymakers, service planners, and public health researchers a practical tool that illustrates access challenges and highlighting critical leverage points for intervention across different levels of influence, with the ultimate goal of improving oral health equity for children in rural and remote Australian communities.
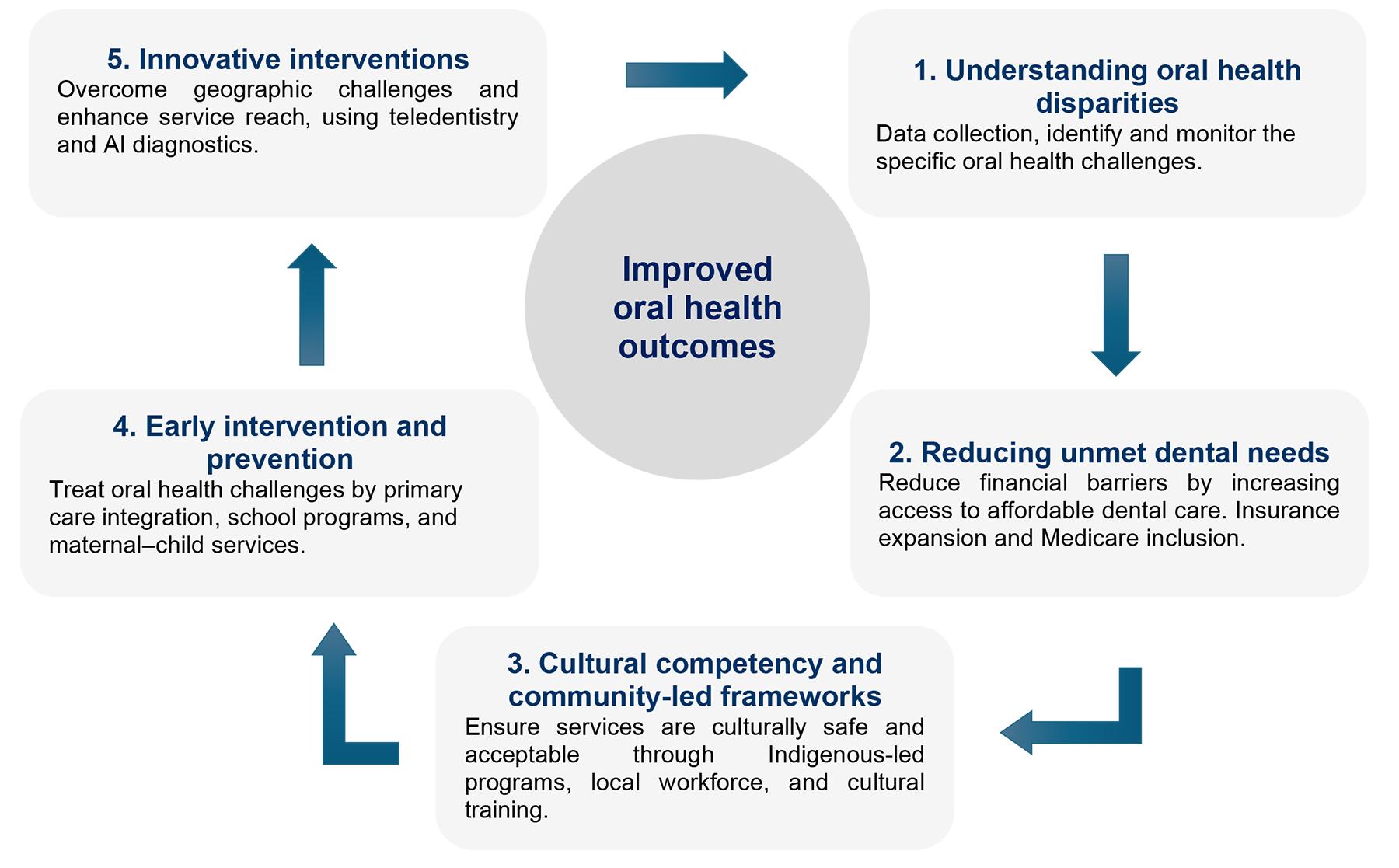 Figure 4: Conceptual model to improve oral health outcomes of children in rural and remote Australia.
Figure 4: Conceptual model to improve oral health outcomes of children in rural and remote Australia.
Conceptual model to improve oral health outcomes for children living in rural Australia
Understanding oral health disparities
Understanding disparities in access to dental care is crucial in addressing gaps in oral health among rural and remote populations, particularly for children. Evidence indicated that paediatric oral health service requirements differ from adult care and therefore warrant specific consideration in service planning44. Children’s oral health is shaped by the developmental stage of dentition and growth. Hence, paediatric models commonly emphasise prevention and early intervention, such as fluoride varnish, fissure sealants, and establishment of toothbrushing and dietary routines in early life to reduce future disease burden44. Studies also report that service delivery requires behaviour guidance and child-friendly approaches, with outcomes influenced by the family/caregiver role, as parents/carers are central to consent, attendance, daily preventive practices, and follow-up27,47,48.
Our review reveals that dental coverage and access in rural and remote Australia remain lower than in major cities, indicating a historical underservicing. Similar barriers are reported internationally, including higher poverty, lower rates of dental insurance coverage, geographic barriers, lack of water fluoridation, and fewer dentists available49. While rural health access issues are a global concern, Australia’s large geographical distances and the sparse populations amplify these barriers. The unique interplay of these factors in the Australian context constitutes a distinct national challenge not consistently emphasised in international literature, requiring coordinated policy reform, innovative service delivery models, and community engagement for addressing rural oral health inequities and improving long-term outcomes for children.
Reduction in unmet dental needs
Reducing the prevalence of unmet dental needs requires policy-level interventions that expand financial access to oral health care. In rural Australia, the high cost of dental services, coupled with limited private dental insurance and restrictive public dental schemes, presents a significant barrier. Consequently, families postponed dental treatment, sometimes for several years43. As a result, minor dental issues inevitably worsen over time, ultimately leading to hospitalisation for more invasive treatment45, resulting in significantly higher public healthcare expenses compared to early intervention11. In 2021–22, approximately 78,761 hospitalisations due to dental conditions could have been prevented. This hospitalisation rate was highest in children aged 5–9 years and among socially vulnerable children6.
Expanding insurance coverage or expansion of existing schemes (eg enhancements to the Child Dental Benefits Schedule and the broader integration of comprehensive dental services into Medicare) could alleviate these financial burdens by reducing direct out-of-pocket costs. International evidence supports this, with Medicaid expansion in the US demonstrating improved dental care access for underserved populations50. However, while initiatives like the Child Dental Benefits Schedule have increased private dental service availability in Australia, eligible children in rural areas still face significant utilisation challenges51. These challenges include geographical isolation, limited awareness of financial support, and insufficient integration of culturally safe practices51.
Culturally competent approaches
Included studies highlight the profound influence of the health profile, historical experiences, and cultural distinctiveness of Aboriginal and Torres Strait Islander populations. The delivery of dental care is frequently reported in the included studies as failing to align with the holistic principles central to Aboriginal and Torres Strait Islander culture, with services typically provided by non-Indigenous professionals who are not part of the communities they serve, leading to cultural disconnects, miscommunication, and a lack of trust22,27,39. Included qualitative and mixed-methods studies further describe how these experiences have shaped healthcare-seeking behaviours and contributed to pronounced disparities in access24,35.
Similarly, culturally minoritised groups in countries such as the US, New Zealand, and Canada, experience a disproportionate burden of dental caries. In these settings, national public health initiatives have sought to reduce disparities through social support and culturally tailored approaches52. For example, evidence from Canada suggests that social support can play an important role in promoting oral health behaviours among culturally minoritised groups53. Across included studies, culturally competent care was emphasised as more than language translation; it requires attention to patients’ lived experience, cultural beliefs, values, and social contexts22,24,35. Moreover, community engagement in the co-design and implementation of oral health programs, particularly for Aboriginal and Torres Strait Islander populations, has been reported as a strategy that may strengthen cultural competency and service acceptability23-25. In this context, oral health services and promotion programs targeting Aboriginal and Torres Strait Islander populations may benefit from collaboratively planned, implemented, and evaluated with the communities they aim to serve23,25.
Early intervention and preventive care
The connection between oral conditions and other health diseases creates opportunities for oral healthcare messages to be part of primary health care16. Integrating oral health into primary health care offers a strategic approach to promoting early intervention and prevention, particularly in rural settings where children often have regular contact with GPs, nurses, and Aboriginal Health Workers26. International evidence supports interprofessional collaboration that expands preventive oral health activities among non-dental providers alongside appropriate reimbursement models. Notably in the US, North Carolina’s reimbursement program for medical professionals providing preventive dental care for children led to a fourfold increase in preventive visits compared to dentist-only visits, and reduced inequalities in access54.
Similarly, community-level paediatric prevention pathways, such as school-based oral health programs and mobile dental clinics, have improved access to preventive services for underserved children and may reduce disparities in dental care access47. To enable effective integration, health systems require supportive policy settings, aligned funding and incentives, workforce training and task shifting, updated clinical guidelines, and interoperable information systems, supported by effective referral and communication pathways between primary and dental care providers26.
Innovative interventions
Innovative service models are crucial for overcoming the geographical barriers and workforce shortage in rural and remote communities15,26,28. Teledentistry can support remote triage, consultations, and follow-up55. Mobile dental units equipped with teledentistry capabilities have been successfully deployed in schools and community settings, reducing the need for long-distance travel and associated costs while improving access to preventive and basic restorative care, with evidence supporting the clinical effectiveness and economic efficiency of teledentistry55. In the US, school-based teledentistry programs in rural areas were able to deliver 97% of necessary treatments, halving the need for in-person dental visits56. High compliance with recommended follow-up care was also observed among paediatric patients in rural locations following teleconsultations57. These findings underscore the potential of teledentistry to extend specialist care into underserved areas, offering a solution to address persistent inequalities in access15,26,28.
Strengths and limitations
This systematic review demonstrates several methodological strengths that enhance the robustness and reliability of its findings. First, the comprehensive literature search strategy ensured the inclusion of all relevant studies. Second, this integrative mixed-methods review, combining quantitative and qualitative evidence, delivers a richer, more nuanced understanding of the barriers. Third, the development of an ecological model to visualise how factors at the system, policy, community, and individual levels interact adds clarity to the complex, multi-level nature of access issues. Moreover, the subsequent construction of a conceptual model translates these insights into actionable, evidence-based strategies tailored to each barrier level.
This review also has important limitations. First, relatively few quantitative studies have specifically explored barriers to oral health service access among paediatric populations, limiting our ability to quantify the prevalence and relative weight of individual obstacles. Second, we found no studies that directly compared rural and urban children’s experiences of accessing dental care, preventing empirical assessment of how geographic setting exacerbates or mitigates barriers. Third, substantial demographic heterogeneity and limited disaggregation across included studies, particularly inconsistent reporting by age group, gender, and Indigeneity, restricted subgroup comparison.
Conclusion
The findings of this systematic review indicate that children in rural and remote communities have historically experienced myriad challenges in accessing oral health services. This synthesis highlights the complex, interrelated nature of multi-level barriers, indicating that isolated interventions targeting individual barriers are unlikely to succeed. Instead, a comprehensive, multi-level and multisectoral approach is essential. Enhancing service availability and accessibility must be accompanied by efforts to address broader social determinants of health, including education, housing, nutrition, and social support. Interdisciplinary collaboration among healthcare providers, policymakers, community leaders, Aboriginal Health Workers, and other stakeholders is critical to developing sustainable, culturally appropriate, and community-driven solutions.
Acknowledgements
The authors acknowledge the University of Western Australia librarians for their assistance with search strategies and King Abdulaziz University for ongoing support.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors have no conflict of interest to declare.
AI disclosure statement
Generative AI was used solely as a language editing aid. ChatGPT (OpenAI, GPT-5.2) was used to paraphrase and refine the wording of a limited number of sentences. No AI tools were used for literature screening, data extraction, risk-of-bias assessment, synthesis, statistical analysis, interpretation of results, or figure/table generation, and no synthetic data or images were produced. All AI-assisted text was reviewed, edited, and verified for accuracy by authors, who take full responsibility for the content.
Data availability
Extracted data are available from the corresponding author on request.