







Context
Chronic wounds are wounds that have prolonged healing processes affecting the anatomy and physiology of the skin, with an estimated prevalence of 2.2 per 1000 population1. The most prevalent types of chronic wounds are diabetic foot ulcers, venous ulcers, pressure ulcers, surgical wound dehiscence, and skin tears2,3.
The incidence of chronic wounds is expected to rise alongside non-communicable chronic diseases (NCDs), such as cardiovascular diseases, cancer, chronic respiratory diseases, and diabetes4-6. These NCDs account for 75% of global deaths7, with a higher concentration in the Global South, primarily low- and middle-income countries with often fragmented health systems8.
In this regard, studies have shown that people living with type 2 diabetes mellitus are 25% more likely to develop a foot ulcers and that 85% of lower limb amputations are preceded by a neuropathic ulcer, with a mortality increase of up to 70% at 5 years2,6,9.
The coexistence of NCDs and wounds severely impacts quality of life, affecting physical, psychological, economic and social aspects, and wellbeing. This problem represents a substantial burden on the health system and society, partly due to high costs, especially in populations with a high prevalence of NCDs2,6,9.
Mexico, part of the Global South, faces significant healthcare challenges due to high rates of diabetes (18.0%), hypertension (27.8%), and obesity (37.1%) in adults10. This situation is exacerbated in rural populations, where factors like malnutrition, marginalization, discrimination, lack of access to specialized services, and a shortage of trained personnel favor the emergence of chronic wounds as a complication of NCDs.
The state of Yucatán in south-eastern México exemplifies this challenge. With a 10.7% prevalence of diabetes and 21.7% of hypertension11, the risk for wounds is high, particularly those for diabetic foot. These diseases and their complications give rise to significant healthcare problems, especially in vulnerable and marginalized contexts, such as among the Indigenous communities of Yucatán.
Therefore, this project aimed to co-construct an educational strategy for the prevention and basic care of wounds in Maya-Yucatecan Indigenous communities in the municipality of Chankom.
Issue
Chankom is a municipality located 142 km east of Mérida (state capital of Yucatán), deep in the Mayan jungle and adjacent to Chichén Itzá (Fig1). It has a population of 4981 inhabitants, spread out across eight towns and two ranches (eg Ticimul, Xcopteil, and Xkalakdzonot), each with approximately 800 inhabitants.
The main economic activities are agriculture, beekeeping, and the production of handicrafts. Traditional gender roles are well defined, with men performing physical work outside the home, and women managing domestic tasks, raising children, and performing precision work, such as embroidery. Hammock weaving is another important activity, regardless of gender12.
Chankom is classified as having a very high degree of social lag, with 70% of its population being Indigenous (Maya-Yucatecan), and only 8% having access to health services13. The closest urban center is Valladolid, which is home to a general hospital (Fig1). However, it is not the first option for care due to scarce transportation and subsequent shortages of personnel, materials, and specialists14. This situation forces people to seek private care, incurring high out-of-pocket expenses.
Nationally, wound care in Mexico suffers from a lack of specialists and poor infrastructure, with only 301 public wound clinics in 21 of 32 states15. The only public woundcare clinic in Yucatán is in Mérida, along with most specialized health centers (Fig1) Geographic, economic, and language barriers further restrict access for Indigenous communities14.
Additionally, wound statistics in Mexico are often unreliable due to underreporting, making it challenging to accurately estimate their true prevalence. In Yucatán, the only publicly available data are from annual reports16. In 2021, the state government documented 222 diabetic foot cases treated at a second-level hospital in the capital.
While there exist guidelines for chronic wound care, including for diabetic foot17,18, they are based on urban populations with assumed access to interventions such as specialized footwear, socks, materials, and services. These recommendations do not reflect the reality of marginalized Indigenous cultures, which necessitate culturally appropriate interventions that are responsive to specific community needs.
This project is part of a broader community-based participatory research study on NCDs and rheumatic diseases in the Maya-Yucatecan population19. During the first phase in the communities of Chankom (Ticimul, Xcopteil, Xkalakdzonot), basic wound care was identified as a pressing need. Ethnographic records, and participant and non-participant observations, were carried out at all four stages of the research20, alongside the activities detailed in Table 1.
Table 1: Community-based participatory phases for implementation
| Phase | Objective | Activities | Participants |
|---|---|---|---|
| Situational analysis | To identify the most common health problems and specific health needs of the population. | Informal interviews | Local health professionals. Administrative staff of the health jurisdiction. |
| Focus group | WHLs | ||
| Development |
To identify the types of wounds, traditional practices, and most frequent occurrences in the population. To become informed about the learning interests of the participants. |
Focus group | WHLs |
| To co-construct a culturally appropriate educational strategy for chronic wound prevention and care in the community. | Work meetings | Wound specialist nurse, general nurses, anthropologist, and WHLs. | |
| Implementation |
Theoretical sessions: To provide information on skin care and chronic wound prevention. Practical session: To develop skills for identifying risk factors and implementing basic preventive actions, as well as performing hygiene and basic wound coverage. |
Five virtual theoretical sessions and one face-to-face practical session. | Wound specialist nurse, general nurses, anthropologist, and WHLs. |
| Evaluation | To assess the knowledge acquired during the course-workshop. | Administration of an eight-item questionnaire about chronic wound care before and after the intervention. | General nurse and WHLs. |
WHL, women health leader.
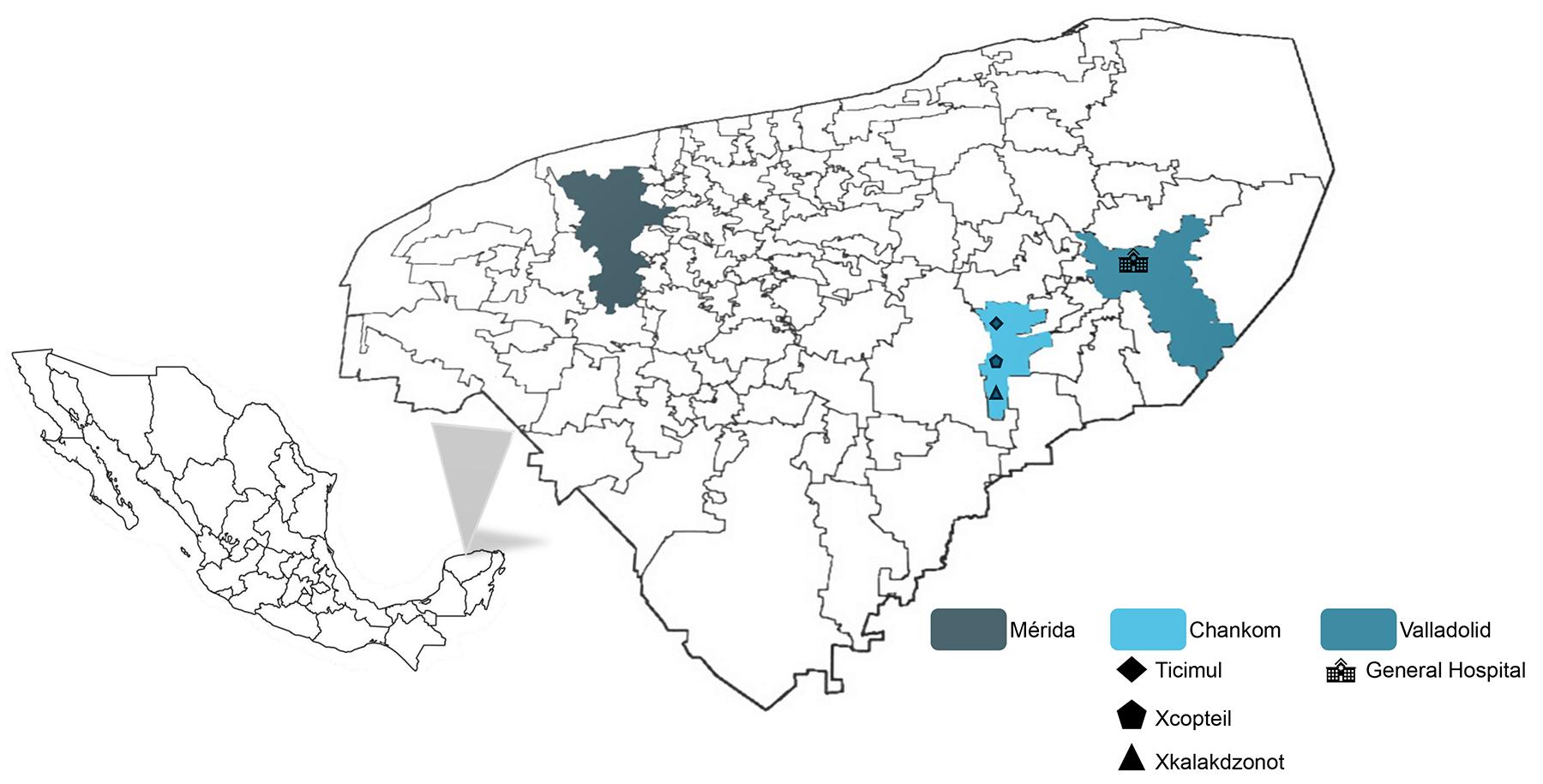 Figure 1: Map of the Yucatán Peninsula, México, highlighting key locations for the study: Mérida (the state capital), the municipality of Chankom (containing the participating communities), and Valladolid (an urban municipality containing the nearest general hospital to Chankom).
Figure 1: Map of the Yucatán Peninsula, México, highlighting key locations for the study: Mérida (the state capital), the municipality of Chankom (containing the participating communities), and Valladolid (an urban municipality containing the nearest general hospital to Chankom).
Situational analysis
Interviews were conducted with three physicians and three nurses (all men, mean age of 38 years) serving the communities. They identified diabetes, hypertension, obesity, and dyslipidemia as the most common NCDs. Wounds were also noted as a prevalent issue, primarily resulting from daily activities (Table 2).
Despite a lack of official data, health authorities similarly identified an increase in diabetic foot ulcer, and potential strategies to address this need were considered (Table 2).
Focus groups with women health leaders (WHLs) also identified diabetic foot ulcer as a problem, with a pressing need to acquire knowledge for home care (Table 2). Consistently, ethnographic records and field diaries documented that the material of commonly worn footwear, combined with uneven and rocky terrain, frequently results in wounds (Table 2).
Table 2: Identified problems and quotes related to non-communicable chronic diseases and injuries in Maya-Yucatecan Indigenous communities
| Problem | Quote |
|---|---|
| High prevalence of non-communicable chronic diseases | ‘... we have a large population that is diabetic and hypertensive, and some with dyslipidemia ... we see between four and five people almost every day. They usually have diabetes, hypertension ... It is very common in the population aged 40 and over, most of them usually have one of these three [diseases].’ (Nurse 1) |
| Footwear and terrain characteristics in Maya-Yucatecan communities | ‘It is common to see injuries caused by footwear that is unsuitable for the terrain, due to the use of sandals, especially plastic ones, by both men and women of all ages ... this habit is closely linked to the high temperatures in the region, which make it impossible to wear closed shoes.’ (Ethnographic record and field diary) |
| Presence of injuries in the communities | ‘... there were many injuries, many cuts, because everyone was carrying wood, using razors, using knives, because in this case, when they cut themselves, they always cut their hands or legs.’ (Nurse 3) |
| Increase in cases of diabetic foot ulcer | ‘... there has been an increase in cases of diabetic foot, we know we must do something ... we are thinking of seeking training for nursing staff, they are responsible for the area of wound care ... so that we can justify the request for more specific wound care supplies ...’ (Official from Jurisdiction II Valladolid) |
| Perceived need | ‘... In the case of complications, for example, we want to know how to clean a wound on a diabetic person, how to detect when that wound has exceeded the limits that require medical attention. Because we are not experts ... we don’t know when they urgently need medication or stronger treatments or deeper cleaning ...’ (Woman health leader) |
Development
Based on identified problems, an educational strategy for wound prevention and basic care was co-developed through meetings with WHLs, three nurses with teaching experience (one with a master’s degree in wound care and two general nurses: one residing in Mexico City and the other living in the community), and an anthropologist.
The educational strategy aimed to include general skin features and wound care, considering the local context and daily activities, though the primary concern was diabetic foot ulcer. It included information on identifying and caring for healthy skin, differentiating between acute wound (traumatic injury) and chronic wound (venous ulcer, arterial ulcer, and diabetic foot ulcer), and recognizing the warning signs.
Five culturally appropriate theoretical sessions were planned on the following topics: characteristics of healthy skin; care for healthy and at-risk skin; types of wounds; factors affecting healing; stigmatization; and specific details on traumatic wounds, venous ulcers, arterial ulcers, and diabetic foot ulcers.
A practical workshop was also designed to develop skills for identifying risk factors, basic preventive actions, hygiene, and basic wound coverage.
Implementation
The educational strategy was delivered as a course-workshop to 13 WHLs aged 25–49 years (Table 3), four of whom had prior formal health training from local health centers. Theoretical sessions were taught virtually by the nurse with a master’s degree in wound care. The WHLs attended sessions in Xkalakdzonot weekly from 5.30 pm to 7.00 pm to avoid high temperatures. The schedule was set by the WHLs, and the general nurse who was living in the community oversaw the logistics.
For each type of wound, sessions addressed: were definition, etiology, illustration of the wound, treatment, self-care, wound prevention, and prevention of wound complications.
These sessions were conducted using language appropriate for the population, incorporating their way of naming things. In addition, the titles of each section were phrased as questions to facilitate understanding, for instance ‘What is it? Why does it occur? What does it look like? How is it treated? What can I do? How can I prevent these wounds and their complications?’
Each session ended with reflections and questions to resolve doubts and explore domestic care practices. This information was incorporated into subsequent sessions to ensure cultural consistency.
The practical session focused on daily care for healthy skin and basic wound care. Using locally available resources (10 cm bandage, non-sterile gloves, gauze, and antiseptic), the participants were instructed to wash a wound with soap and water, apply antiseptic, and cover it with gauze secured by a bandage.
Subsequently, wounds were drawn on participants’ legs/feet to highlight morphological characteristics of each type of wound. In pairs, they assessed the fictitious wounds, asked questions, and described the wound bed.
Two scenarios were practiced:
- patient with an untreated wound with or without coverage: WHLs were instructed to wash the wound with soap and water (due to dirt accumulation from sandals and field work), to apply gauze and bandages, and they pretended to recommend going to the nearest doctor. WHLs were taught to identify signs of infection such as ‘hot skin, red skin, bad smell, severe pain, itching, fever’ or underlying crepitus (‘feeling bubbles under the skin’) as indicators for immediate hospital referral.
- patient with a medically treated wound requiring a gauze change: WHLs were instructed on applying antiseptic, changing gauze, and applying bandages using antiseptic principles.
WHLs were trained to ask key questions, such as ‘How did it happen? How long ago? Are you seeing a professional caregiver? Who is treating you? What have you put on it? Do you have diabetes?’ Finally, they verbalized preventive and skin healthcare recommendations.
Table 3: Characteristics of women health leaders who participated in the educational strategy
| Community | Age (years) | Years of schooling |
|---|---|---|
| Ticimul | 38 | 12 |
|
42 |
6 | |
|
56 |
6 | |
| Xcopteil | 33 | 9 |
|
35 |
9 | |
|
39 |
9 | |
|
48 |
6 | |
|
49 |
9 | |
| Xkalakdzonot | 25 | 12 |
|
27 |
12 | |
|
27 |
12 | |
|
31 |
12 | |
|
41 |
12 |
Evaluation
An eight-item questionnaire based on the course topics was administered to the 13 WHLs at three different times: pre-test (before theory), post-test 1 (after practical sessions), and post-test 2 (1 month later) to assess knowledge retention.
Statistical analysis was applied to the correct answers obtained by the WHLs in each questionnaire administration, reported as a measure of central tendency (mean and median) and dispersion (interquartile range). The Durbin–Conover test was used to compare mean values, with p≤0.05 considered significant. Microsoft Excel was utilized for descriptive analysis and jamovi v2.6 (jamovi project; https://www.jamovi.org) was used for comparative analysis.
Figure 2 shows the results obtained by the time of evaluation. There was significant increase in correct answers between the pre-test and post-test 1, and between the pre-test and post-test 2.
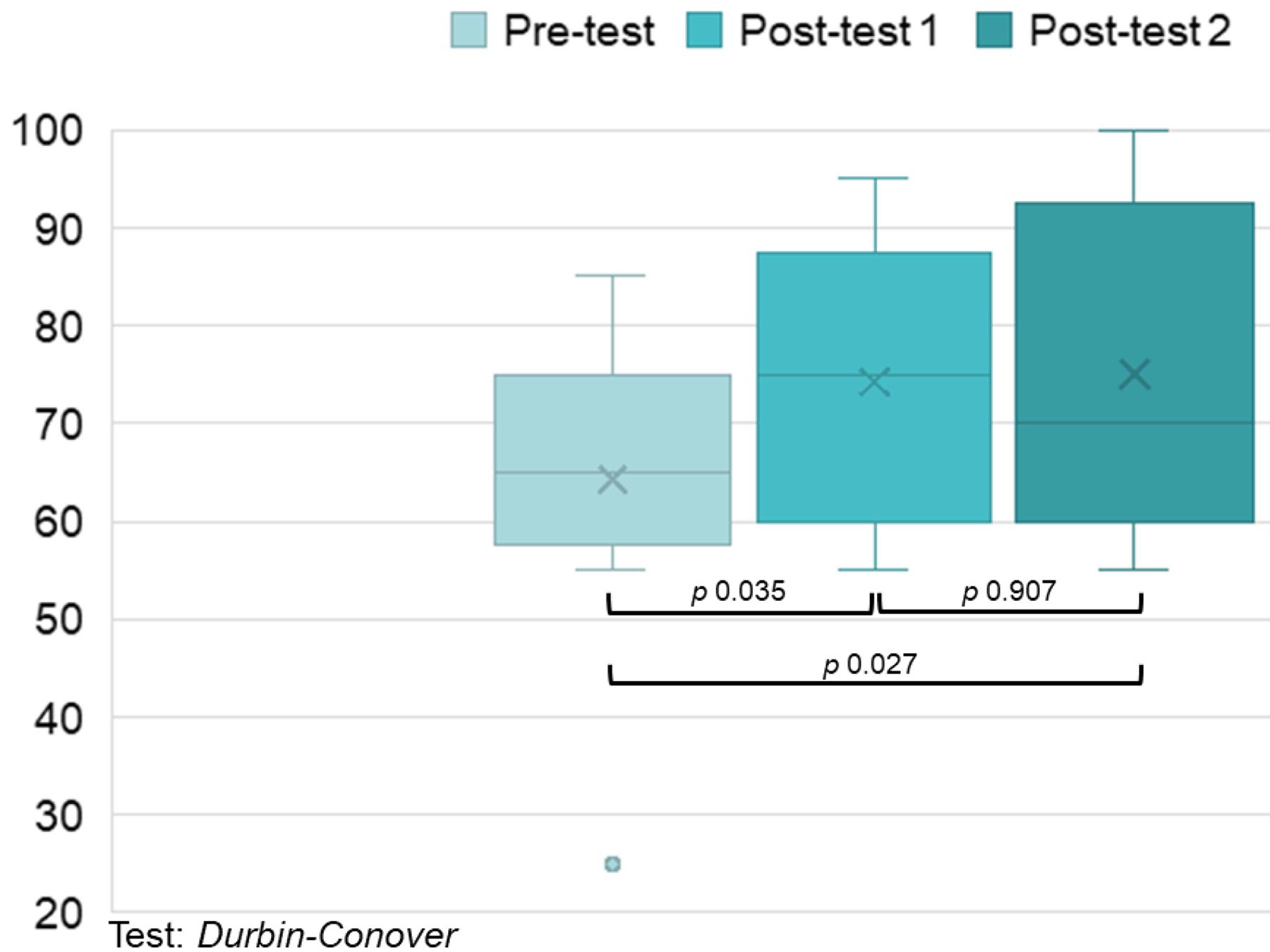 Figure 2: Comparison of evaluation questionnaire scores. Boxplots depict scores from the evaluation questionnaires administered to women health leaders at three time points: pre-test (baseline, before the educational strategy), post-test 1 (immediately following the educational content), and post-test 2 (1-month follow-up after the strategy’s conclusion).
Figure 2: Comparison of evaluation questionnaire scores. Boxplots depict scores from the evaluation questionnaires administered to women health leaders at three time points: pre-test (baseline, before the educational strategy), post-test 1 (immediately following the educational content), and post-test 2 (1-month follow-up after the strategy’s conclusion).
Ethics approval
The broader study was approved by the Ethics and Research Committees of the Hospital General de México ‘Dr. Eduardo Liceaga’ (DI/23/404-B/05/22). Additional approval was obtained from municipal authorities and the general population through community assemblies in each of the participating locations. All participants provided individual informed consent.
Lessons learned
Impact of the intervention
Increased community knowledge was an important outcome of this study, and it was documented that traumatic injuries are the most common wounds in the Maya-Yucatecan communities. When they occur in people with NCDs, especially diabetes, they become chronic and, without adequate care, can lead to limb amputation.
Importantly, interventions that respond to perceived needs and are co-constructed alongside the community are crucial. Such collaborative strategies promote participation, build trust, train community members to share knowledge, and help reduce health complications in marginalized contexts with difficult access to health services.
Opportunities for care
Working with communities enables the identification of cases, since trained community members can provide initial assessments and make referrals to local or specialized services as needed.
This project strengthened collaboration between WHLs (providing preventive/basic care) and health professionals (facilitating specialized care). This ongoing communication lays the foundations for models like telemedicine, bringing expertise to remote areas and reducing inequity. Evidence shows that telemedicine offers similar efficacy and safety to conventional chronic wounds treatment21.
Implications
Considering a community's perspectives and adapting interventions to its available resources enhance their positive impact compared to decontextualized biomedical approaches that do not consider cultural elements.
This aligns with critical health literacy, defined as the ability to reflect on health determinants and apply that reflection in individual or collective actions for health in any context22. Its focus on empowerment and health inequalities, reflection, and action allows for addressing individual and collective agency, contrasting critically with a purely biomedical perspective.
This project showed that standard care guidelines17,18 (eg those for diabetic foot ulcer) are unsuitable for Maya-Yucatecan populations, where shoes are uncommon and podiatry is scarce. Community-based research is essential to generate evidence for clinical guidelines based on the realities of marginalized and vulnerable communities.
Acknowledgements
We acknowledge the women health leaders and health professionals who participated. We thank the Secretaría de Ciencia, Humanidades, Tecnología e Innovación (CVU 671018 and CVU 1145201), and the Latin American Study Group of Rheumatic Diseases in Indigenous Peoples (GLADERPO). We thank Amaranta Manrique de Lara for her critical reading and editing.
Funding
This study received partial financial support from Marista University of Merida.
Conflicts of interest
The authors have no conflicts of interest to disclose.
AI disclosure statement
During the preparation of this work, the authors used DeepSeek-V3.2 in order to improve the structure and readability of the text. After using this tool/service, the authors reviewed and edited the content as needed and they take full responsibility for the published article's content.