




Introduction
The problem regarding low recruitment and retention of doctors in rural areas is a persistent global issue recognised as a significant barrier to achieving equitable health services1,2. This data aligns with facts in Indonesia: according to the Human Resources for Health Information System (SISDMK – Sistem Informasi Sumber Daya Manusia Kesehatan) in 2023, out of a total of 183,694 doctors, the distribution remains unequal, with 60.8% of doctors centralised in the Java and Bali regions. Conversely, doctor shortages occur in the island regions of Eastern Indonesia, including East Nusa Tenggara. Data indicate that 7.03% of community health centres (puskesmas) in East Nusa Tenggara lack a doctor3. Most areas of East Nusa Tenggara are classified as underdeveloped, border, and island areas (DTPK – Daerah Tertinggal, Perbatasan, dan Kepulauan), characterised by complex welfare challenges and minimal infrastructure development4. This region is described as an archipelago with 1192 islands, of which 44 are inhabited islands. Data from the central statistics agency, BPS-Statistics Indonesia, in 2023 shows that East Nusa Tenggara ranks third among Indonesia's poorest provinces5. Many areas in East Nusa Tenggara experience problems with access to clean water, sanitation, infectious diseases, and stunting, as well as high maternal and infant mortality rates6,7.
Strategies and efforts to increase doctor recruitment and retention in rural areas continue to be vigorously pursued8,9. By examining factors influencing doctor distribution and retention, WHO has formulated global guidelines regarding the development, attraction, recruitment, and retention of health workers in rural and remote areas. These guidelines emphasise four intervention strategy groups, covering education, regulation, incentives, and professional and personal support10. Among these four groups, educational intervention is considered the most promising in the long term11. Numerous systematic reviews and evidence-based studies indicate that selecting students from rural backgrounds, designing curricula responsive to local needs, and providing clinical placements for a sufficient duration in rural areas correlate positively with the intention and realisation of doctor practice in rural areas after graduation8,9,12.
The medical education system in Indonesia generally follows a pattern of an undergraduate medical program and a clerkship program lasting about 5.5–6 years, consisting of 3.5–4 years of campus-based preclinical phases and about 2 years of clinical phases in teaching hospitals and health service facility networks. After graduating, doctors must complete a 1-year internship under supervision before obtaining a licence to practice independently. This national policy is then adapted differently by each medical faculty through the determination of location, duration, and clinical placement models.
One concept suggested in the literature as an intervention effort to increase rural doctor recruitment and retention is decentralised clinical training (DCT)13. This concept developed as a form of restructuring the location and model of clinical education into networks of health service facilities outside the primary teaching hospital14. Various cross-country studies show that long-term clinical placements in rural areas through DCT are proven to increase the probability of practising in rural locations after graduation15.
Universitas Nusa Cendana, or Undana, is one of the higher education institutions attempting to adopt the DCT concept. This medical school was established to address the need for doctors in the East Nusa Tenggara archipelago. In structuring clinical rotations, the Undana Medical School represents a form of DCT implementation in an archipelagic and border province environment. International studies of the effects of DCT generally focus on developed-country contexts such as Australia16 or developing countries in African regions17, with health systems and geographical characteristics different from those of the island provinces of Eastern Indonesia. In Indonesia itself, studies on the determinants of intention and the actualisation of practice in rural areas highlight both external and internal factors18,19. However, to our knowledge, no studies have specifically measured the effect of DCT duration on graduates’ retention in Indonesia, especially in the Eastern Indonesia archipelago region.
This study aims to analyse the influence of DCT duration on rural doctor recruitment and retention, using a case study of Undana graduates from the 2008–2017 classes (graduating between 2014 and 2023). Graduates from this period represent the first decade of the medical faculty's existence in East Nusa Tenggara. Over this decade, several developments in clinical practice locations have increased the number of rotations outside the primary teaching hospital. This study specifically quantitatively tests the influence of DCT duration on rural doctor recruitment and retention. The findings of this study are expected to make an empirical contribution to the development of medical education policy and health human resource planning, specifically by informing the design of more effective DCT strategies to increase doctor recruitment and retention in Indonesia's rural and archipelagic regions.
Methods
Context
Undana Medical School is located in Kupang City, the capital of East Nusa Tenggara Province. The clerkship curriculum includes 13 clinical rotations: five major rotations lasting 10 weeks and eight minor rotations lasting 5 weeks (Table 1 and Fig1). Most clinical rotations are conducted at the Prof. Dr. W.Z. Johannes Hospital in Kupang, comprising the provincial referral hospital and the primary teaching hospital. Additionally, clinical rotations are conducted at partner hospitals in large cities and other provinces, namely Dr. Wahidin Sudirohusodo Hospital in Makassar and Dr. Soeradji Tirtonegoro Hospital in Klaten. Therefore, clinical rotations at these three large referral hospitals are excluded from the DCT duration calculation. Besides these three large hospitals, there are community health centres in Kupang City, Ume Manekan Pratama Clinic in Soe, Naimata Mental Hospital in Kupang, and T.C. Hillers in Maumere, which are classified as DCT locations.
Table 1: Durations and locations of Universitas Nusa Cendana, East Nusa Tenggara, Indonesia for cohorts 2008–2017
| Rotation | Duration | Location |
|---|---|---|
| Community medicine | 10 weeks | Puskesmas (DCT) and/or Ume Manekan Pratama Clinic (DCT) |
| Internal medicine | 10 weeks | Prof. Dr. W.Z. Johannes Hospital or T.C. Hillers Hospital (DCT) |
| Paediatrics | 10 weeks | Prof. Dr. W.Z. Johannes Hospital |
| Surgery | 10 weeks | Prof. Dr. W.Z. Johannes Hospital |
| Obstetrics and gynaecology | 10 weeks | Prof. Dr. W.Z. Johannes Hospital |
| Anaesthesiology | 5 weeks | Prof. Dr. W.Z. Johannes Hospital |
| Ophthalmology | 5 weeks | Prof. Dr. W.Z. Johannes Hospital |
| Dermatology | 5 weeks | Prof. Dr. W.Z. Johannes Hospital |
| ENT (otorhinolaryngology) | 5 weeks | Prof. Dr. W.Z. Johannes Hospital or T.C. Hillers Hospitals (DCT) |
| Psychiatry | 5 weeks | Prof. Dr. W.Z. Johannes Hospital or Naimata Mental Hospitals (DCT) |
| Neurology | 5 weeks | Prof. Dr. W.Z. Johannes Hospital or T.C. Hillers Hospitals (DCT) |
| Forensics and medicolegal | 5 weeks | Dr. Wahidin Sudirohusodo Hospital or Soeradji Tirtonegoro Hospital |
| Radiology | 5 weeks | Prof. Dr. W.Z. Johannes Hospital or T.C. Hillers Hospital (DCT) or Dr. Wahidin Sudirohusodo Hospital |
DCT, decentralised clinical training.
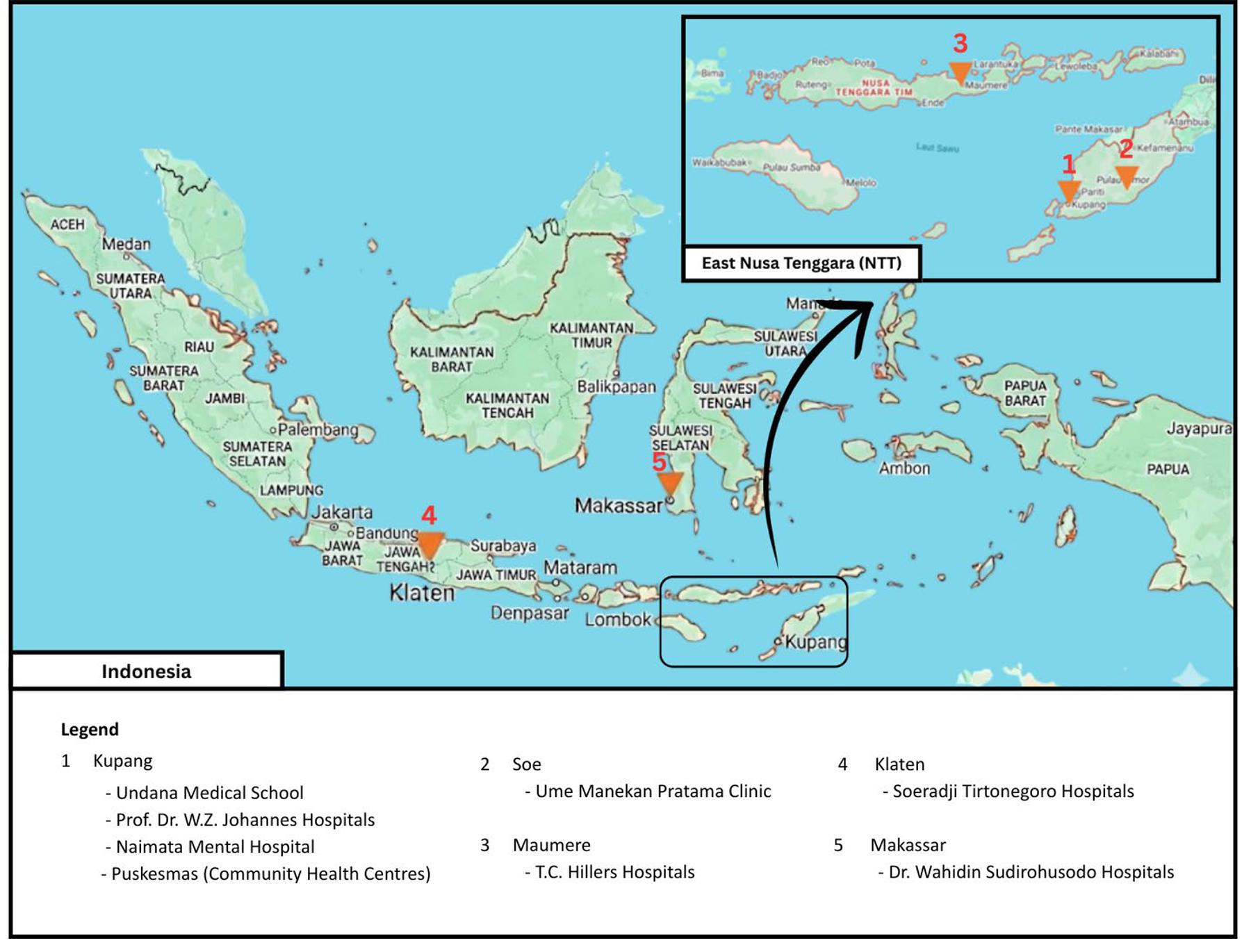 Figure 1: Locations of clinical rotations at Universitas Nusa Cendana, East Nusa Tenggara, Indonesia for cohorts 2008–2017.
Figure 1: Locations of clinical rotations at Universitas Nusa Cendana, East Nusa Tenggara, Indonesia for cohorts 2008–2017.
Design
This study is an observational analytic study with a quantitative approach. A retrospective cohort design was chosen to analyse the influence of past exposure (DCT duration during the clinical clerkship) on the outcome (recruitment and retention of doctors in rural areas) from that exposure to the present.
Population and sample
The population in this study are all alumni of the Undana Medical Profession Program, classes 2008–2017, who graduated in 2014 to present. A total sampling approach was used to select the samples. Inclusion criteria were alumni who had completed the internship program, had their clinical rotation data recorded by the Education Coordination Committee, and were willing to participate in the study. Alumni who had died, whose personal contacts could not be reached or whose rotations were not recorded in the alumni database, and those who did not complete the questionnaire, were excluded from the analysis.
Variables
Decentralised clinical duration (independent variable)
DCT duration was calculated by summing the durations of all clinical rotation stations (in weeks) conducted outside the main teaching hospital, including community health centres, primary clinics, and regional hospitals in the East Nusa Tenggara Province. Referral hospitals located in large cities in other provinces were excluded from the DCT duration calculation. The calculated duration is the standard duration for each rotation, excluding any time spent repeating rotations.
Doctor recruitment into rural areas (dependent variable)
This variable was a measure of whether or not (dichotomous: yes/no) the respondent has worked in a village/subdistrict area classified as rural based on Head of BPS Regulation Number 120 of 2020 since completing the internship until this study period (September 2025).
Duration of doctor retention in rural areas (dependent variable)
The duration of doctor retention in rural areas is calculated in years. Retention duration is calculated by summing the total years of working in village/subdistrict areas classified as rural under Head of BPS Regulation Number 120 of 2020, from the completion of the internship to the start of this study period (September 2025). Respondents who never worked in rural areas were excluded from the retention analysis.
Data sources
This study used secondary data for the independent variable, the DCT duration completed by alumni during their clinical clerkship. This secondary data was taken from the alumni database of the Education Coordination Committee of the Undana Medical Clerkship Program. Primary data on recruitment status and retention duration in rural areas were collected using a questionnaire distributed online by email and each alum's personal WhatsApp. The questionnaire was structured using the site All Counted (https://www.allcounted.com) and included questions exploring respondents’ characteristics, employment history (location and duration) since completing the internship, and reasons for choosing the practice location. Each workplace location was classified as urban or rural according to Regulation of BPS-Statistics Indonesia Number 120 of 2020 concerning Classification of Urban Villages and Rural Villages in Indonesia20.
Statistical analysis
Data were analysed with Jeffreys’s Amazing Statistics Program v0.95.4. (JASP; https://jasp-stats.org). The influence of DCT duration on doctor recruitment was analysed using binary logistic regression, and the impact of DCT duration on doctor retention in rural areas was measured with linear regression. In the analysis, data were grouped into three cohorts: 2008–2010, 2011–2013, and 2014–2017. This cohort-cluster approach was used to meet the minimum data requirements of 30 samples for regression tests (since not all cohorts have 30 samples) and to address potential confounding from the cohort factor (differences in work duration due to different graduation times). Additionally, there were study program policy changes related to DCT duration that differed across clusters – DCT duration increased as more collaborations were established with local health facilities, particularly non-main teaching hospitals. The distribution of DCT duration across cohorts is shown in Table 2.
Table 2: Distribution of decentralised clinical duration by cohort
| DCT duration (weeks) | Cohort | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | ||
| 10 | 25 | 23 | 20 | 20 | 8 | 10 | 1 | 1 | 2 | 3 | 113 |
| 15 | 0 | 2 | 0 | 6 | 2 | 8 | 1 | 3 | 4 | 3 | 29 |
| 20 | 0 | 0 | 0 | 0 | 7 | 4 | 13 | 5 | 2 | 1 | 32 |
| 25 | 0 | 0 | 1 | 2 | 3 | 6 | 14 | 7 | 11 | 6 | 50 |
| 30 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 5 | 2 | 7 | 17 |
| 35 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 5 | 8 | 3 | 21 |
| Total | 25 | 25 | 21 | 28 | 20 | 28 | 37 | 26 | 29 | 23 | 262 |
DCT, decentralised clinical training.
Ethics approval
This study was approved by the Health Research Ethics Committee of the Faculty of Medicine and Veterinary Medicine, Universitas Nusa Cendana (54/UN15.21/KEPK-FKKH/2025).
Results
Respondents
The alumni database shows that 545 alumni from the classes of 2008–2017 completed the Undana Medical Clerkship Program. This study successfully recorded 370 responses (response rate: 67.8%) and analysed 262 responses after excluding those that did not meet the inclusion criteria (Fig2).
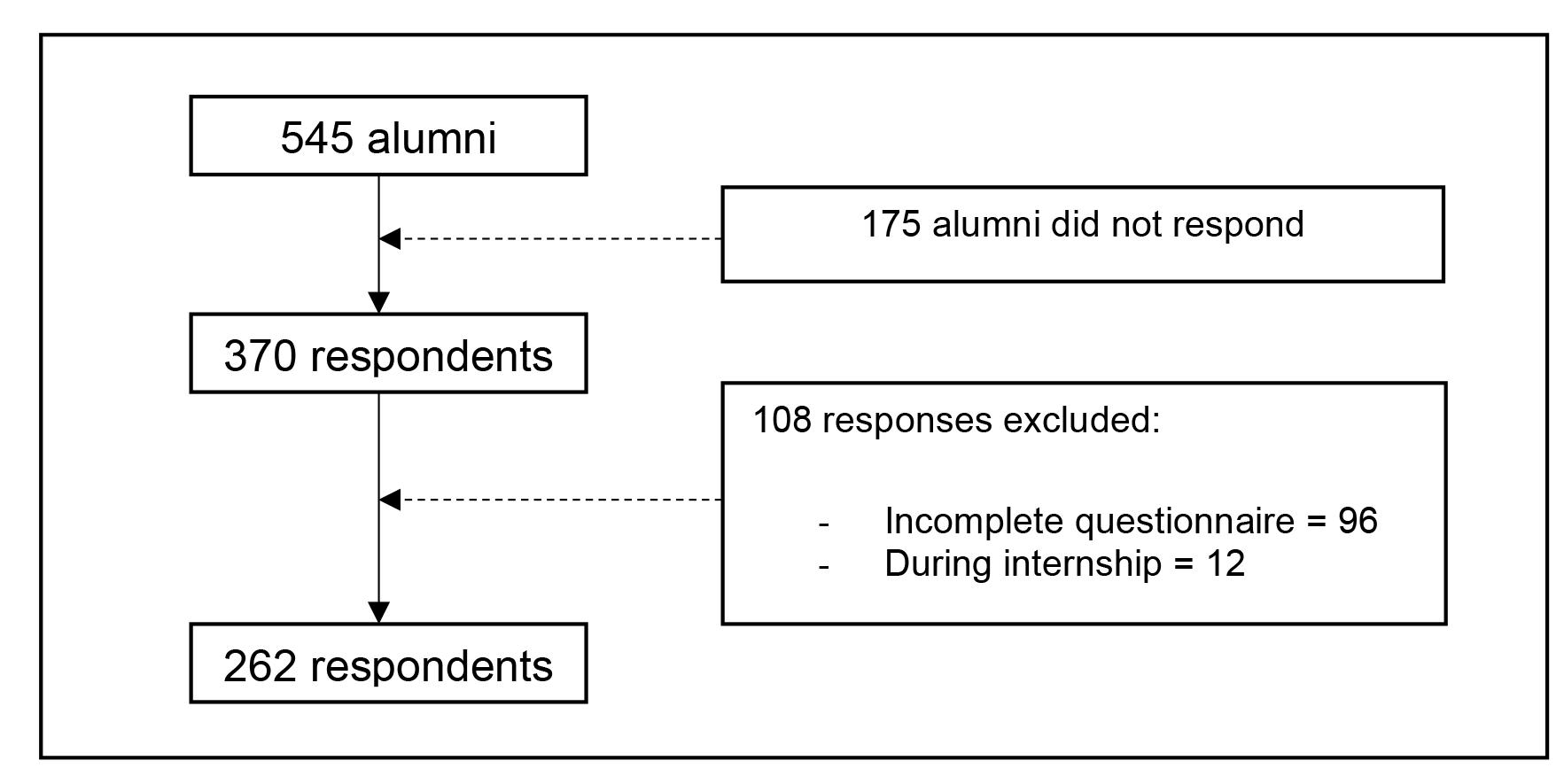 Figure 2: Respondent recruitment process.
Figure 2: Respondent recruitment process.
Demographics
A total of 262 responses were analysed in the study. As shown in Table 3, the majority of respondents were female (67.9%), from the class of 2014 (14.1%), unmarried (60.3%), had no children (71.4%), originated from urban areas (86.3%), and were not pursuing further education (74.4%).
Table 3: Respondent characteristics
| Characteristic | Variables | n (%) or mean±SD |
|---|---|---|
| Gender | Male | 84 (32.1) |
| Female |
178 (67.9) |
|
| Age | 30.12±2.95 | |
| Class | 2008 | 25 (9.5) |
| 2009 |
25 (9.5) |
|
| 2010 |
21 (8.0) |
|
| 2011 |
28 (10.7) |
|
| 2012 |
20 (7.6) |
|
| 2013 |
28 (10.7) |
|
| 2014 |
37 (14.1) |
|
| 2015 |
26 (9.9) |
|
| 2016 |
29 (11.1) |
|
| 2017 |
23 (8.8) |
|
| Marital status | Married | 104 (39.7) |
| Unmarried |
158 (60.3) |
|
| Has children | Yes | 75 (28.6) |
| No |
187 (71.4) |
|
| Region of origin | Urban | 226 (86.3) |
| Rural |
36 (13.7) |
|
| Further education | None | 195 (74.4) |
| Ongoing Master’s degree |
9 (3.4) |
|
| Ongoing specialist training |
46 (17.6) |
|
| Master’s degree |
4 (1.5) |
|
| Doctoral degree |
1 (0.4) |
|
| Specialist |
7 (2.7) |
|
| Current practice location | Urban | 164 (62.6) |
| Rural |
98 (37.4) |
SD, standard deviation.
Effect of decentralised clinical training duration on doctor recruitment in rural areas
Table 4 shows that of the total 262 respondents, 158 respondents had experience practising in rural areas. This percentage indicates that the Undana Medical School contributes to increasing doctor recruitment, with 60.3% of its graduates having worked in rural areas.
The logistic regression results show that the coefficient for the DCT duration variable is negative across all periods, indicating a negative relationship between program duration and the likelihood of recruitment. This means that the longer the DCT duration, the lower the chance of recruitment success tends to be. However, the magnitude of this effect is minimal, as reflected in the odds ratio (OR) values close to 1 (0.750–0.967), meaning the change in duration only provides a minimal decrease in odds (less than 25%). The 95% confidence interval for the odds ratio includes 1 across all periods, indicating that the effect of DCT duration is not meaningful. This is reinforced by the p-values, all of which are greater than 0.05 (0.212–0.277), indicating that the null hypothesis is accepted: DCT duration does not have a statistically significant influence on recruitment across the three observed clusters. Overall, these findings suggest that the duration of the DCT program is not a primary determinant of recruitment success.
Figure 3 shows the reasons participants chose their rural practice location. This indicates that the decision to start practising in rural areas was multifactorial, with three main reasons: government placement (27.8%), returning to the region of origin (10.1%), and serving those in need (9.5%).
Table 4: Binary logistic regression analysis of the effect of decentralised clinical training duration on rural recruitment
| Cohort | Recruitment to rural area | Coefficient | OR | 95%CI | p-value | |
|---|---|---|---|---|---|---|
|
Yes (%) |
No (%) | |||||
| 2008–2010 | 52 (73.2) | 19 (26.8) | –0.266 | 0.750 | 0.505–1.163 | 0.212 |
| 2011–2013 | 42 (55.3) | 34 (44.7) | –0.046 | 0.955 | 0.880–1.037 | 0.277 |
| 2014–2017 | 64 (55.7) | 51 (44.3) | –0.033 | 0.967 | 0.917–1.020 | 0.222 |
| Total | 158 (60.3%) | 104 (39.7%) | ||||
CI, confidence interval. OR, odds ratio.
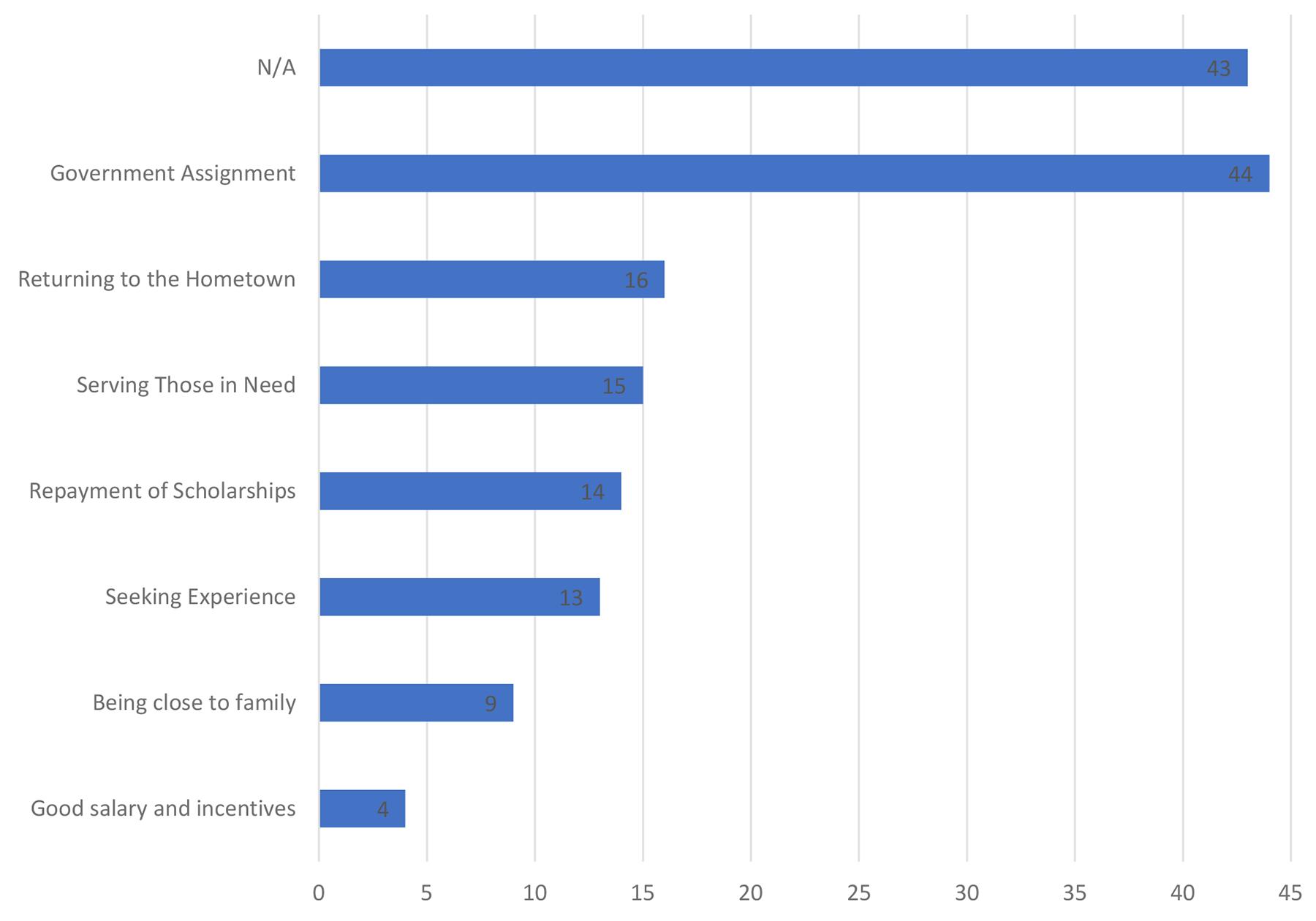 Figure 3. Respondent reasons for recruitment/practice in rural areas. N/A, not answered.
Figure 3. Respondent reasons for recruitment/practice in rural areas. N/A, not answered.
Effect of decentralised clinical training duration on doctor retention in rural areas
Analysis of the influence of DCT duration on doctor retention in rural areas was conducted only among respondents who had ever practised in rural areas (n=158 ). Respondents who did not experience recruitment or had never worked in rural areas (n=104) were excluded from the analysis. Table 5 presents the linear regression analysis results for the independent variable ‘DCT duration’ against the dependent variable ‘retention duration’. Overall, this table shows variations in relationship patterns across groups, with a trend shifting from an insignificant negative in older cohorts to a significant positive in newer cohorts, reflecting cohort-specific retention dynamics.
The linear regression results show a change in the pattern of the relationship between DCT duration and retention duration in different cohort groups. In the 2008–2010 cohort, the unstandardised coefficient was negative (–0.108) and the r value was 0.089, indicating a very weak negative relationship – meaning that longer DCT duration tended to decrease retention duration slightly. However, this relationship was not statistically significant (p=0.530), likely because in the 2008–2010 class, DCT duration was still minimal and nearly homogeneous across all samples (Table 5). Hence, the variation in duration was insufficient to produce a significant pattern. The 95% confidence interval encompassing zero (–0.451–0.235) confirms this insignificance.
In the 2011–2013 cohort, the unstandardised coefficient remained negative (–0.081), with r=0.246, indicating a slightly stronger negative relationship than in the previous period. However, this relationship remained insignificant (p=0.117), suggesting the onset of DCT duration variation, but was not heterogeneous enough to have a detectable impact on retention differences. The confidence interval encompassing zero (–0.183–0.021) confirms this insignificance (Table 5).
A striking pattern change occurred in the 2014–2017 cohort, where the unstandardised coefficient became positive (0.054) with r=0.273, indicating a moderate positive relationship – meaning the longer DCT duration, the longer rural practice duration This relationship was statistically significant (p=0.029), likely because in the 2014–2017 classes, DCT variation began to appear and distribution started to even out, so the program duration could provide a more measurable positive impact on retention. The entirely positive confidence interval (0.006–0.102) confirms the positive effect (Table 5).
Overall, these findings emphasise a trend shift from an insignificant negative relationship in older cohorts to a significant positive one in the newest cohorts, reflecting the evolution of the DCT program over time. Factors of variation and distribution of rural placement duration appear to be key in revealing this pattern. These results indicate that the longer the DCT duration, the longer the doctor retention in rural areas.
Table 5: Linear regression analysis of the effect of decentralised clinical training duration on retention in rural areas
| Cohort | r | Unstandardised coefficient | Standardised coefficient | t | p-value | 95%CI |
|---|---|---|---|---|---|---|
| 2008–2010 | 0.089 | –0.108 | –0.089 | –0.632 | 0.530 | –0.451–0.235 |
| 2011–2013 | 0.246 | –0.081 | –0.246 | –1.603 | 0.117 | –0.183–0.021 |
| 2014–2017 | 0.273 | 0.054 | 0.273 | 2.237 | 0.029 | 0.006–0.102 |
CI, confidence interval
Discussion
This study analysed the influence of DCT duration on doctor recruitment and retention in rural areas in East Nusa Tenggara, Indonesia. Our study's main findings reveal complex dynamics: DCT duration proved insignificantly influential on the initial decision to recruit doctors to rural areas across all cohorts, but showed a progressive, significant shift in its influence on retention duration in the most recent cohort.
The statistical insignificance in the early cohorts (2008–2013) was likely due to the ‘restriction of range’ phenomenon, caused by the homogeneity of DCT duration data. This is evident in Table 2, where DCT duration was minimal, with the majority of students completing only a 10-week rotation. In statistical principles, data homogeneity limits the regression model's ability to detect correlations21.
The analysis of the influence of DCT duration on recruitment showed consistent negative coefficients, but they were not statistically significant across all cohorts (odds ratio=0.750–0.967, p>0.05; Table 4). Our findings indicate that DCT duration is not a strong predictor of graduates' ability to choose initial practice in rural areas. This is because the reasons underlying the decision to work in rural areas are multifactorial and complex22. This interpretation aligns with the findings of Zapata et al (2020), who concluded that health workforce recruitment interventions in rural and remote areas often fail to achieve significance when relying solely on the duration of clinical exposure, because external factors such as government regulations and financial incentives are more influential23.
In our context, ‘government placement’ was the most dominant recruitment reason (27.8%) for doctors to work in rural areas. This shows that most doctors choose rural practice as civil servants, which in Indonesia is associated with income stability, a guaranteed retirement fund, allowances, and a clear career path. Additionally, many government programs, such as Nusantara Sehat or the non-permanent employee program, also play a significant role. These findings align with studies conducted by Strasser et al24 and Wakerman et al25, which state that local health policies have a considerable influence on the decision to practice in rural areas.
The second most common recruitment reason for working in rural areas is ‘returning to the hometown’ (10.1%). Aligning with the findings of Pagaiya et al12 and Ogden et al26, it is stated that DCT needs to be strengthened through recruitment strategies for students from rural origins to maximise long-term recruitment and retention. This implies the need to recruit more medical students with rural backgrounds in the future. The Undana Medical School can play a role in this by providing early health-profession exposure for children in rural East Nusa Tenggara. This concept is known as the ‘inspiration’ stage, and has not been implemented much in medical schools in island regions.
The following most common reason is ‘serving those in need’ (9.5%). These findings align with a study conducted by Handoyo et al, which states that intrinsic factors such as social motivation and personality play an essential role in the decision to work and stay in rural areas27. Besides providing rural exposure to increase this motivation, it is essential to offer training that enhances students' social motivation, for example through social service activities and community service in rural areas. This also aligns with a study by Ngcobo et al, which found that long-duration DCTs to increase recruitment intention need to be combined with qualitative element support, such as meaningful experiences28.
Furthermore, the analysis results of the influence of DCT duration on retention duration revealed a striking pattern change between cohorts. However, the magnitude of this effect is minimal, as reflected in the odds ratio values close to 1 (0.750–0.967), meaning the change in duration only provides a minimal decrease in odds (less than 25%). The 95% confidence interval for the odds ratio includes 1 across all periods, indicating that the effect of DCT duration is not meaningful. This shift indicates that DCT duration is increasingly recognised as positively affecting retention duration as the curriculum evolves. This difference was detected because the DCT duration data were more heterogeneous across respondents. However, our findings underline that retention is not solely a function of duration but also an interaction with the maturation of the education program, where the newest classes may benefit from a more stable curriculum. This stability is evident in achieving a DCT duration of 35 weeks for the class of 2014 and onward. This occurred as more collaborations were established with local health facilities across the East Nusa Tenggara archipelago.
Theoretically, a longer duration facilitates a more mature process of social bonding and professional adaptation, allowing graduates to build the resilience needed to survive in resource-limited areas29,30. These findings support the research of Bally et al, which states that DCTs have a positive impact on long-term retention only if the program has reached a stage of maturity and is well integrated into the local health system31. DCTs are designed to bring medical students closer to the real practice context in the community, increase curriculum relevance to local needs, and build social attachment between students and the placement area. Cross-country studies show that long-term clinical placements in rural areas through DCT increase clinical competence, self-confidence, and learning satisfaction, and are significantly associated with a higher probability of practising in rural locations after graduation32.
Our findings in this study – insignificant recruitment and significant retention – explain the distinct mechanisms between recruitment and retention. The decision to work in rural areas (recruitment) is influenced by initial intent, which is closely related to policy and regulation33. The decision to stay (retention) is closely related to resilience and a person's adaptability in surviving and finding ‘rural comfort’34. These results suggest that DCT may function not as a primary ‘magnet’ to attract doctors, but rather as an ‘anchor’ preparing them to stay. The synergy between regulation and policy (for recruitment) and DCT (for retention) is the key to the sustainability of rural health services in the Indonesian context.
Study implications
Our findings have significant implications for the development of medical education policy and health human resource planning in rural and archipelago regions of Indonesia, specifically in the context of DCT programs. First, the insignificance of DCT duration in doctor recruitment to rural areas indicates that educational strategies alone are insufficient to overcome health worker distribution inequality. This implication encourages integrating DCT with other interventions35. In line with WHO recommendations, a multifactorial approach can increase recruitment effectiveness10,36.
Second, the significant positive trend shift in DCT duration and retention in the 2014–2017 classes suggests that DCT can be a long-term tool for retaining doctors in rural areas. The practical implication is the need to invest in developing rural health facility networks as DCT platforms, including infrastructure improvements and professional support, to strengthen doctors' attachments to the community18,19. This aligns with cohort study findings in South Africa, where DCT with mature and relevant concepts has been shown to increase health worker retention in rural areas28. Theoretically, this research enriches the literature on educational interventions in health worker retention.
Limitations
This study has several limitations. First, the retrospective cohort design relies on primary data via online questionnaires, which are prone to recall bias – where respondents may not accurately remember their work history, especially for longer retention durations. Second, the stratification analysis based on cluster (2008–2010, 2011–2013, 2014–2017) successfully isolated the cohort confounding effect, but did not control for other variables such as age, gender, marital status, or regional origin, which are known to influence practice location preferences based on the literature21. Third, methodologically, linear regression for analysing retention duration has limitations compared to survival analysis, which is better suited for handling censored data37. In this study, retention data may be censored because some doctors might still be working in rural areas at the time of the survey (September 2025), so their retention duration is incomplete. It could result in an underestimation of the DCT duration effect. This limitation suggests the need for prospective research with survival methods to validate findings. Nevertheless, the stratification and simple regression approach still provide valuable initial insights in the context of limited data.
Conclusion
DCT duration did not significantly influence the recruitment of Undana medical graduate doctors to East Nusa Tenggara rural areas. However, DCT duration had a positive and significant effect on doctor retention in rural areas in the most recent classes (2014–2017). These findings emphasise that external factors, such as government placement, regional origin, and intrinsic motivation, are more dominant in recruitment. At the same time, the evolution of DCT programs can support long-term retention. Overall, the results of this case study provide empirical evidence that educational strategies such as DCT need to be integrated with multifactorial interventions – including regulation, policy, and the recruitment of students from rural areas – to address low recruitment and retention of doctors in rural areas. Thus, this study contributes to the development and evaluation of medical education interventions, with recommendations to maintain or increase the quantity, duration, and quality of DCT to support the achievement of equitable health services in rural and archipelagic areas.
Funding
This research received no external funding. The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors disclose that they are affiliated with the medical school under study as staff and a student. To minimise bias, the author followed strict research protocols and objective data analysis. No other conflicts of interest exist.
AI disclosure statement
The authors disclose the use of Grammarly (v6.8.263) and ChatGPT (OpenAI) as AI-assisted tools. Grammarly was used to translate and refine the language of this manuscript. ChatGPT was used to extract data for the literature review. No AI tools were used for data collection, analysis, interpretation, or figure generation. All translated content was reviewed and approved by the authors, who take full responsibility for the manuscript.