



Introduction
The majority of qualified health professionals live and work in cities, resulting in a global phenomenon of rural health workforce shortages1. Compared to people living in urban areas, people living rurally have reduced access to health services, which negatively affects healthcare equity and health outcomes. Since the early 2000s, successive Australian federal and state governments have tried to address rural health workforce shortages through the implementation of a range of policy and program initiatives targeting both the health and education sectors and through a range of initiatives aimed at encouraging health students to consider ‘going rural’2. Until recently, these ‘going rural’ initiatives have mostly focused on medical students and involved selecting students from a rural background, requiring a significant proportion of the student cohort to complete an extended rural training year or to undertake all their medical training rurally. These initiatives have more than doubled the number of Australia’s medical, nursing and allied health graduates and increased the overall size of Australia’s rural health workforce, especially among doctors working in rural primary care settings. However, while there have been improvements in rural allied health and nursing workforces, ongoing shortages persist2,3. This article focuses specifically on nursing and allied health workforces, while acknowledging that there are also similar and different issues and incentives for medical practitioners. The incentives for attracting medical practitioners to work in rural areas are considerably different, resulting in medicine-specific workforce retention and turnover challenges that are outside the scope of the present article. Furthermore, nursing and allied health make up the bulk of the community-based mental health workforce in rural and remote Australia, on which this research focuses.
One of the greatest challenges currently facing Australia’s rural and remote public health services is being able to attract and retain ‘experienced’ allied health professionals. Compared to doctors and nurses, allied health professionals are twice as likely to leave their rural or remote position4. The average allied health professional’s rural stay is 3 years and this reduces further in remote areas5. In addition, allied health professionals who commence rural employment as new graduates are more likely to leave than those recruited at more senior levels5. This high rural turnover of new graduate allied health professionals has been linked to the use of Australia’s rural public health services as ‘professional nurseries’ by graduates from cities6. While historically Australia’s rural nursing workforce has been more evenly distributed and more stable, it is increasingly experiencing the negative effects from being an older workforce, with 40% of Australia’s nurses currently aged over 50 years7. In addition, it is negatively impacted by a general decline in interest in nursing as a career8. Recent Australian workforce planning projections forecast that, in the medium- to long-term, demand for nurses will significantly exceed supply, with a projected shortfall of 85 000 by 2025, and 123 000 by 20308. This will likely be more keenly felt in Australia’s more difficult-to-staff rural and remote areas.
In health workforce literature, retention and turnover are terms commonly used when discussing the average length of time between commencement and termination of employment of staff and for discussing the extent of workplace or workforce flux9,10. Because turnover is difficult to research qualitatively given the challenges of recruiting ex-staff, turnover intention – an individual’s thoughts about leaving and intention to quit – among current staff is often used as a proxy measure of turnover, given it is a very strong predictor of an individual’s decision to actually leave a health position11. In this study, turnover intention and reasons for staying/leaving are used interchangeably, as are turnover and retention.
Previous research investigating rural recruitment and retention of nursing and allied health professionals, both in Australia and other developed countries, identifies three main influences: workplace conditions, career advancement opportunities (including access to continuing professional development (CPD)), and social and personal factors1,12,13. These influences have been found to either have a pull effect (to take up a rural position or in deciding to stay) or a push effect (to leave a rural health position)14,15. How, and at what point, these aspects influence the retention of allied health and nursing professionals working in rural Australia has not been well researched16. To date, most retention studies on Australia’s rural nursing and allied health workforces have focused on single professions and on the influence of workplace conditions and/or career advancement factors. Social and personal factors have generally been much less researched. Moreover, the research has usually focused on the experiences of new graduates in their first year of work, with much less attention given to the next few years of early-career development. Overall, there is a dearth of qualitative understanding of the factors affecting retention, particularly how workplace conditions, career advancement opportunities and social and personal factors collectively impact retention.
Some of the most severe and protracted rural health workforce shortages can be found in public sector mental health services17. Australia’s public mental health service system includes both hospital-based acute inpatient services and community-based services. In rural areas, inpatient mental health services are generally only available in regional secondary hospitals, and these operate in large rural towns, while community mental health (CMH) services are more widespread, operating in both small and large rural towns. Public sector CMH is a multidisciplinary nursing and allied health workforce17. Health professionals working in public sector CMH services usually work in case-management positions and they provide generic rather than discipline-specific client services18. Despite severe staffing shortages and high staff turnover in rural and remote CMH services, research on factors affecting retention of this workforce has been very limited17,19. Drawing on this small body of literature and supplementing it with findings from retention studies undertaken with other closely related health workforces (such as Australian health professionals working in mental health inpatient services and/or in metropolitan areas or other rural public health services), CMH professionals’ decisions to stay or leave their rural position are influenced by a complex interaction of organisational, role and personal factors.
The findings from the literature review were considered insufficient to frame the research question and a research design. To supplement the extant literature, a pilot study was conducted for the purpose of strengthening understanding of the rural-based CMH workforce and for identifying any staffing issues. This pilot study was undertaken with public sector service managers responsible for staffing and running rural-based CMH services located in the Australian state of New South Wales (NSW). In NSW, public health care is administered by NSW Health through a network of Local Health Districts (LHDs), which are based on geographically contiguous regions, defined by population size. The pilot study confirmed that staff turnover was a major issue and high turnover among early-career health professionals was of particular concern20. 'Early-career' is a term commonly used in Australia’s health sector to refer to the first 5 years of working in a professional role after completing tertiary level qualifications. In addition, the pilot study found that service managers knew little about the reasons for early-career staff leaving20. Based on the pilot study findings and the literature, and seeking to understand the full range of personal and work factors contributing to turnover intention, the research question formulated for this study was How do employment and rural-living factors impact turnover intention among early-career, rural-based CMH professionals in their first few years of working in non-metropolitan NSW? Because this study was particularly focused on experiences in the ‘first few years of working’, early career was further classified into two levels of experience: beginner (0–3 years) and intermediate (3–5 years).
Methods
Theory underpinning the methodology
The constructivist grounded theory methodological approach of Charmaz21 was selected for the study. Charmaz argued that the roots of constructivist grounded theory lie in social constructionism22 where constructivism is shorthand for social constructivism and is commonly combined with interpretivism23,24. Both constructivists and interpretivists aim to make sense of the process by which meanings are created, negotiated, sustained or modified25. Two key assumptions underpin a constructivist-interpretivist perspective: that individuals seek understanding of the world they live in and make meaning of their experience through their interactions with others (ie reality is socially constructed26) and that the meanings developed by individuals are always subjective and so are varied and multiple. Individuals make meaning within the social, cultural, historical and temporal contextualities. For this study, an in-depth interview approach27 was used to support the building of rapport and mutual understanding between researcher and participant and for the full-telling of the participant’s personal story and rural-living and current work experience.
Because the study sought to understand the full range of factors affecting individuals’ turnover intentions, a symbolic interactionist framework underpinned the methodological grounded theory approach. This meant that the research question would be answered through the development of a substantive theory (which concerns the particular situational context of a specific group of people at a certain time and place and is built on participants’ data). Also, given that turnover intention is a process occurring over time for the purpose of supporting theory development, identification of a basic social process (a theoretical code amenable to modelling that accounts for variation in time, context and behaviour of the phenomenon under investigation) was another research objective. In a grounded theory approach, theory generation results from a bottom-up, inductive reasoning process and involves the continual intermeshing of data collection and data analysis (constant comparative analysis)28. Thus, sampling occurred in stages and was always aimed at theory generation28. Each sampling stage was driven by findings or issues emerging from the constant comparative analysis of the data collected to date28. This conceptualisation, coding and categorisation of data (all included in the term coding) was an ‘essential aspect of transforming raw data into theoretical constructions of social processes’(p. 746)29.
Sampling
For this study, a criterion sampling strategy was developed for participant selection. Participants were required to:
- currently work, or have recently worked, for NSW Health in a CMH service situated in rural NSW
- meet the eligibility criteria set by NSW Health to work as a ‘mental health professional’
- have between 1 and 10 years work experience in public sector CMH services.
Drawing from position descriptions for CMH roles, eligible professions included registered nurse, psychologist, occupational therapist, social worker and Aboriginal mental health worker (AMHW). The study aimed to recruit participants from all eligible health profession groups. While the study’s focus was on the experiences of ‘early-career’ CMH professionals, the work duration was set at 10 years because of anticipated difficulties in finding sufficient participants who would meet the accepted definition of ‘early-career’, given the extent of staffing issues identified in the pilot study20. Anyone recruited for the study who had more than 5 years of CMH work experience was asked to particularly reflect on their work experiences in their first 5 years of working as well as to discuss their current experiences. To differentiate these more experienced participants from those meeting the more accepted definition of ‘early-career’ (first 1–5 years of working), this group were termed ‘experienced’. Definitions of these and other key terms and concepts used in this article are included in Table 1.
The pilot study also found that staffing challenges increased with service remoteness20. As a result, recruitment of participants for the study targeted CMH services operating in different sized towns of varying degrees of remoteness. A town classification system was developed to support this. The classification system drew on population data from Australia’s 2011 census and the Australian Bureau of Statistics (ABS) geographic stratification system, the Australian Standard Geographical Classification – Remoteness Area (ASGC-RA). The ASGC-RA typology is based on the nearest road distance to an urban centre and includes five categories: major cities (RA1), inner regional (RA2), outer regional (RA3), remote (RA4) and very remote (RA5)25. Drawing on ABS 2011 community profiles census data, small towns were classified as having populations of less than 20 000; medium towns 20 000–30 000 and large towns 30 0000–50 000 people.
Twenty-six CMH professionals were recruited for this study. Recruitment occurred by the first author making presentations at CMH meetings. Participants included the full range of eligible profession groups: registered nurses (n=6), social workers (n=6), psychologists (n=4), occupational therapists (n=3), AMHWs (n=5) and others (n=2). With regard to career stage, 16 people were early-career, eight were beginners and eight intermediate. The other 10 participants were experienced. With regard to background, 12 people were working in their hometowns (defined as the town in which they had lived during the majority of their secondary school years), one was from another rural town and 14 were from elsewhere (either Australian major cities or from overseas). The participants were working in CMH services operating in nine rural towns operating in two LHDs in rural NSW. These CMH services were situated in towns of differing size: large (n=2), medium (n=1) and small (n=6). The nine towns covered three of the five ABS remoteness area (RA) categories: three inner regional (RA2), four outer regional (RA3) and two remote (RA4). Participant characteristics are detailed in Table 2.
The two services situated in remote areas (RA4) had teams of fewer than five staff and both had chronic staffing shortages and were heavily reliant on agency staff to backfill unfilled positions. Recruitment of participants in these two remote sites occurred towards the end of data collection for the purpose of expanding remoteness, but to do so required the inclusion criteria to be relaxed to accommodate the impossibility of meeting the inclusion criteria in these remote locations. This resulted in three participants not meeting all the inclusion criteria: participant (P) 24, an Aboriginal support worker who did not meet the health profession eligibility criteria; and P25 and P26, who each had more than 10 years of CMH work experience and therefore did not meet the work duration criteria.
Table 1: Definition of key study terms and concepts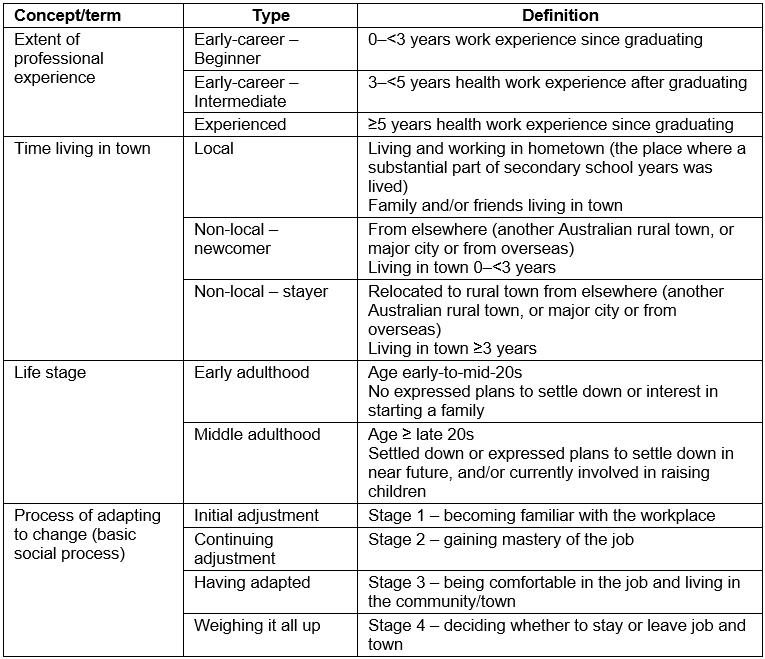
Table 2: Study participant characteristics and town descriptors 
Data collection and analysis
Participant interviews were conducted by the first author over an 11-month period (July 2013–June 2014). The interviews were conducted in four batches, with each batch taking a particular sampling focus, such as town type or a particular professional group. The interviews were semi-structured and conducted face-to-face and, on average, took 1¼ hours. Each interview followed a linear time approach. Participants were first asked to focus on the past and their reasons for taking the job, then the interview moved to discussing initial and current experiences of the job and, where relevant, their experience of relocating and living in the town, and concluded by asking whether they were intending to stay or leave. Through the joint analytic discussions of all three authors, latter participants were asked additional questions to interrogate emerging categories; for example, What was your experience in finding your place in the CMH team and the broader workplace? Who do you rely on for social support in the town? After each batch, the interviews were immediately transcribed verbatim by the first author, participant pseudonyms applied and other identifying information removed. NVivo v10 software (QSR International; http://www.qsr.com) was used throughout the study to support management of all data and analysis. The three authors designed the study and the co-authors validated the coding and analysis, leading to the development of the substantive theory.
Data analysis relied on Charmaz’s21 coding approach, which involves three-stages: initial, focused and advanced. Initial coding of the transcripts concerned applying open codes using an incident-by-incident approach, focused coding involved grouping the open codes into categories until a core category was identified, and advanced coding concerned theory building and relied on the identification of the basic social process. The review of the first batch of transcripts (P1–6) resulted in the creation of 129 open codes, and focused coding immediately followed. To make the open codes more meaningful, they were typed into a Word document and sorted manually by cutting and pasting until groups of like codes were clustered. As well as supporting refinement of the codes, this process assisted with the development of a preliminary descriptive account of the process leading early career CMH professionals to stay or leave their jobs.
This identified process was used to develop 10 preliminary categories, and each category was given a descriptor. These were (1) making career plans, (2) job seeking, (3) weighing up the costs and benefits, (4) arriving and finding one’s feet, (5) adjusting to rural-living – outsiders, (6) making connections, (7) doing a big job, long-term, (8) working in a bureaucracy, (9) finding your place in the team and (10) deciding to stay or leave. These 10 categories were preliminary only and considered to be weak in terms of their explanatory power and the linkages between them. After completing interview batches 2 and 3, some more open codes were created, and refinement and subsuming of the open code list continued. This resulted in the categories being subsumed to eight: (1) job seeking, (2) taking the job – motivations, expectations and promises made, (3) finding one’s feet, (4) the importance of social connection, (5) handling team dynamics and work relationships, (6) working in an environment of change and uncertainty, (7) doing a hard job, long term and (8) deciding to stay or leave.
After conducting coding of the batch 3 interviews, the eight categories were further reviewed, at this point focusing on process issues and identifying sequential stages. The stages identified were (1) seeking, (2) landing, (3) adjusting, (4) connecting, (5) adapting, (6) managing and (7) deciding. These were matched against the eight preliminary categories to reflect the processual nature of the phenomenon. At this point of categorisation, categories 5 (handling team dynamics and work relationships) and 6 (working in an environment of change and uncertainty) were subsumed into one category and renamed as category 5: adapting – finding your place in the team and workplace. This reduced the categories to seven. At this point of the coding process, the properties (characteristics) of the categories began to be defined. Strauss and Corbin30 described properties as defining and giving categories their meaning. Birks and Mills31 explained that properties need to be defined either in terms of their dimensions or their range of variance. In this study, the properties covered such things as time in the job, prior CMH work experience, prior rural Australia exposure, staffing levels and remoteness of town.
At the coding stage of the fourth and final batch of interviews (P14–26), properties (characteristics) had been applied to the seven categories. The final part of focused coding concerned identifying the core category. This involved reviewing all transcripts, extensive memo-writing and use of storyline to investigate the robustness of the core category proposed. As a result of this work, several analytical breakthroughs occurred, resulting in increasing conceptual abstraction and the categories being further reduced to three: (1) sense of belonging to the town, (2) feeling valued and supported in the workplace and (3) managing the workload. These three categories were all assessed as concerning life aspirations and the extent to which participants’ professional and personal expectations were being met by their job and living in the town. This resulted in the identification of the core category: professional and personal expectations being met.
Advanced coding then followed, commencing with a second literature review for the purpose of situating the identified categories and key concepts within the existing research literature. These concepts included transition to practice, adaptation to rural living, health teams and organisational dynamics, social dynamics of rural communities, and life stage. Literature on the link between turnover intention and meeting expectations was also investigated. The latter identified that burnout and job (dis)satisfaction were the major factors affecting turnover intention and this was determined by the work role, workplace situation and career opportunities. Given this broad range of job satisfaction determinants, it was selected to measure participants’ employment satisfaction, but the broader term professional satisfaction was adopted. As a corollary to this, personal satisfaction was selected to measure participants’ personal expectations. In the latter stage of advanced coding, Glaser’s theoretical coding families32,33 were drawn on to assist in the identification of the basic social process, which was identified as adjusting to change and is explored below.
Ethics approval
University ethics approval for this research was gained from the University of New England’s Human Research Ethics Committee (HE13-022), as well as from the two NSW Health Research Ethics Committees operating in the LHD from which the participants were recruited.
Results
Turnover intention theory
The turnover intention theory presents a whole-of-person explanation of turnover. It was developed based on the identified core category of professional and personal expectations being met and the identified basic social process, adjusting to change. The theory posits that individuals’ decision to stay or leave their job is determined by the meeting of life aspirations, and this relates to the extent of the gap between individuals’ professional and personal expectations and the reality of their current employment and rural-living experience. The extent of individuals’ professional and personal expectations was measured by satisfaction levels. Figure 1 sets out the concepts and causal relationships of the turnover intention theory, which are explained in detail below and relevant literature discussed.
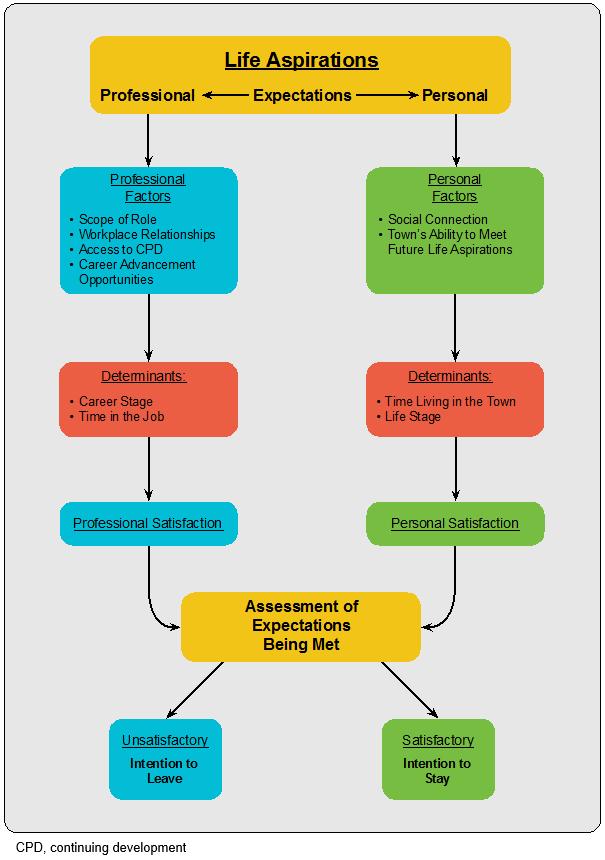 Figure 1: Causal relationships – turnover intention theory.
Figure 1: Causal relationships – turnover intention theory.
Professional satisfaction: Participants’ professional satisfaction was found to be positively or negatively affected by the scope of the CMH position, relationships in the workplace, and the extent of access to CPD and career advancement opportunities. The size of the gap between individuals’ professional expectations and their actual experience was found to decrease with time in the job and the extent of prior work experience in health, as P6 discusses:
The first couple of years was really just establishing my sea legs and finally I felt like I had some sense of what I needed to be doing. Years 2–4 … was not so much chasing my tail all the time. I could start to put some things in place that made things better.
In terms of workplace relationships, feeling valued by the service-level manager was an important contributor to job satisfaction. Participants explained that ‘feeling valued’ concerned believing their manager understood the challenges and demands of their job and appreciated their efforts. Team dynamics were frequently mentioned as strongly influencing professional satisfaction. Team dynamics were discussed as being affected by various team factors including mix of experience levels and professions, age range and gender balance. The degree to which an individual felt they worked in a supportive team environment was mentioned by several participants as being highly sensitive to staffing changes, as P15 explains:
I think it’s really good now [the team dynamic], even maybe a year or so ago it wasn’t. We had a couple of older ladies who had been there for a long time, from when I was there before. People who are just stale, just don’t want to be there, who are negative. You’d suggest something new and they say: ‘Oh, oh, that could never work, oh, no’.
High staff turnover was discussed by participants in all but one of the nine CMH services and commonly viewed as negatively affecting workloads and team dynamics, as P16 discusses:
People are leaving because they are overworked. But if we had a full team I think it would be different. Before we were understaffed people left because they were moving from town not because of the job. … But that’s what happens [now] when you are dealing with 30 or 40 … [clients] because you don't have enough staff and that number is getting bigger whilst our staff is getting smaller.
These findings strongly accord with the CMH literature. Onyett et al’s UK study on the rewards of a CMH job found that the highest rated factors were working in a team, interdisciplinary work, feeling effective clinically and clinical work generally34. Positive teamwork was also found to be a protective factor against burnout35,36. In Wilson and Crowe’s qualitative study of 12 New Zealand public sector CMH nurses, nurses’ therapeutic relationships with their clients were found to be the major source of job satisfaction37. The study identified that this therapeutic relationship could be positively or negatively affected by work or personal factors including the team dynamic, relationship with the line manager and work–life balance issues. In an Australian study of occupational therapists working in mental health roles, Scanlan et al identified the importance of feeling supported and valued by management as contributing to the job satisfaction38.
Personal satisfaction: For the study, personal satisfaction was defined as being the extent of an individual’s sense of belonging towards the town, as well as the assessment of the town’s ability to meet their future life aspirations. Among the participants who were living and working in their hometown (defined as locals – see Table 1), not surprisingly all expressed a strong sense of belonging to the town and to the local community. In comparison, almost all of the participants from elsewhere (non-locals) discussed feelings of alienation and social disconnection, especially in the first year of living in the town. The extent of social isolation was found to be more intense among the non-locals who were also new to CMH work (early-career – beginners) and for people who were single and/or who had had limited or no prior experience of rural ‘Aussie’ (Australian) culture, as P12 explains:
You know in a town like [X] … it’s very difficult if you’re not from here or brought up here or you don’t know much about country Australia when you arrive. I was shocked when I arrived here and there was dogs on the back of utes and cowboy hats, it was like Texas to me. It was just so: ‘Oh my god, where am I?’ type of thing.
Non-locals said that their feelings of alienation significantly reduced after 12 months of living in the town and that feelings of belonging increased incrementally the longer they lived in the town. Most locals and non-locals who had been living in the town for more than 3 years were intending to stay living in the town for the foreseeable future (stayers). This decision involved varying degrees of attachment to the town and feelings of belonging to the community. For the non-local stayers, it had usually involved having made a conscious positive decision about the town’s ability to meet their (and any significant other’s) future life aspirations. These non-local stayers were usually involved in raising families or were planning to start one soon (a life stage termed middle adulthood), as P21’s experience highlights:
Well, we only intended to move out here for two-years … After the two-years had gone past, we didn’t really realise that it had been two-years already … [And] just in the last 12 months we’ve really made the decision [to stay]. We are ready to have kids now, that’s why we got married last year – to settle down and have kids.
Among all these stayers, most thought their public sector CMH position offered the best employment available in the town – in terms of remuneration and parental leave entitlements, as P10 explains:
There is a lack of equally remunerated positions available outside of Health … and that is the thing that makes you stay.
The participants who had no stated plans for settling down or expressed little or no interest in raising a family were the early-career beginners. These participants were all in their early-to-mid-20s (a life stage defined as early adulthood) and included both locals and non-locals. All had assessed the town as not being able to meet their future life aspirations. Among the non-local leavers, they had generally taken their public health position for career advancement reasons and had always intended returning home after gaining sufficient clinical experience to obtain a more senior health position. This contrasts with the leaving plans of locals, who were generally less concerned with career advancement and more focused on personal development, and this group all discussed having plans to travel or to live and work elsewhere.
The literature investigating social dynamics of communities distinguishes between the experiences of local and non-locals and discusses the latter groups’ process of ‘fitting in’ as involving both acceptance by others and self-identification39. Relph posited that there were seven degrees of outsidedness and insidedness: at one end, strangeness and alienation from living in an unfamiliar place and, at the other, deep un-selfconscious immersion from living somewhere very familiar40. This ‘fitting in’ spectrum strongly accords with the range of experiences described by this study’s participants. Gillespie and Redivo’s study investigating the factors affecting retention of mental health professionals working in rural Canada found that those who worked in small remote towns were the least satisfied with their job and the rural lifestyle41. They found that the most dissatisfied workers were those who had been recruited from outside the local town (non-locals)42. Lonne’s study of Australian social workers found that non-locals experienced a more difficult adjustment lasting 12–18 months43. Lonne proposed that non-locals’ adjustment was five-phased and U-curved in shape44. These phases accord closely with the experiences described by non-locals in this study, although arguably their initial fall was faster and sharper than Lonne’s, as a honeymoon stage was usually not experienced.
The basic social process: The extent of an individual’s professional and personal satisfaction was found to be influenced by their stage of adjustment to the job. The identified basic social process concerned adjusting to change and involved four adjustment stages: initial adjustment, continuing adjustment, having adapted, and weighing it all up. All participants discussed experiencing a difficult initial adjustment upon starting their CMH job, described as ‘rabbit in the headlights type daunting’ (P10). This stage involved becoming familiar with the workplace. For those who had previously worked in public health, this initial adjustment stage tended to last only a few months. However, for those who had no, or very little, prior public health work experience, this initial adjustment stage could last up to 12 months. Participants in this latter group were usually the beginners, as P13’s experience as a beginner social worker highlights:
I think my learning has gone on a massive curve ball in the first twelve months and in that time, it’s [my learning] just been constant [continual].
After the initial adjustment stage, there was a less intense but still challenging stage of continuing adjustment. This stage involved gaining mastery of the job and developing the skills and knowledge to confidently work with clients and navigate the health system. The greater the level of an individual’s relevant work experience, the less time it took to gain the requisite competencies, generally taking individuals around 12 months to gain mastery. However, for those who had little or no prior work experience (beginners), mastery of the job could often take between 18 months and two years, as P6 describes:
And I remember having several conversations just saying: ‘I don’t feel like I’m doing a good job, but I don’t even know what a good job would look like’. I had nothing to guide me, so it probably took a good 18 months for me to really find my feet.
Once having learned to perform the job competently, most participants described feeling comfortable in the job (having adapted), as P18’s experience highlights:
I’d say after about a year I became really confident doing assessment before that I was really panicking …. [In the beginning] I was doing the case management and the not very complex clients ones, the light ones. … but now they’re very complex ….
At the time of interview, most participants had already made an assessment as to whether the job and/or the town was meeting their (and any significant other’s) needs (weighing it all up) and deciding whether they would stay or leave their job and/or the town (turnover intention). Turnover intention was found to usually be decided early on in employment, generally around 12–18 months of working and for some participants it was even earlier than this.
A major finding from the identification of the basic social process was that, in the adjustment stages (initial and continuing), turnover intention was most strongly affected by professional experiences, in particular those relating to the job role, workplace relationships and level of access to CPD. In this stage, personal satisfaction mostly concerned those with limited social connections in the town (ie non-local – newcomers). After having adapted, the major influence on turnover intention shifted to personal satisfaction, and this was most strongly affected by an individual’s life stage (Fig2). By drawing on the turnover intention theory and the basic social process, it was possible to make a risk assessment of turnover intention. Three levels of risk were identified: highly vulnerable, moderately vulnerable and not very vulnerable (Fig3).
The adjustment stages of the basic social process were found to closely accord with those outlined by Duchscher’s stages of transition theory, which identified a 12-month adjustment process for new graduate nurses to professional practice45. Lea and Cruickshank also drew on Duchscher’s framework for their study on the adjustment of Australian rural-based nurses, and their findings concurred with Duchscher’s stages and timeline, as well as identifying a harder adjustment experience for nurses working in rural settings46. They attributed this to the rural work environment and additional work demands placed on nurses working in rural services, which accords with the present study’s findings. Erikson’s theory of life stages provides useful context for these findings, particularly the three stages of adulthood: young, middle and late47. While there is considerable debate as to the chronological ages relating to life stages, there is general agreement concerning the characteristics of each particular stage48-50. Young adulthood focuses on career advancement, pursuit of social activities and pair-bonding, while middle adulthood is concerned with stability, settling down, and is focused on family and work47,48,50. Hay observed that place attachment strengthens at the beginning of middle adulthood and is often linked to the place in which the person is living at the time51. These life-stage characteristics and place-attachment experiences all resonate strongly with the experiences of the participants in this study.
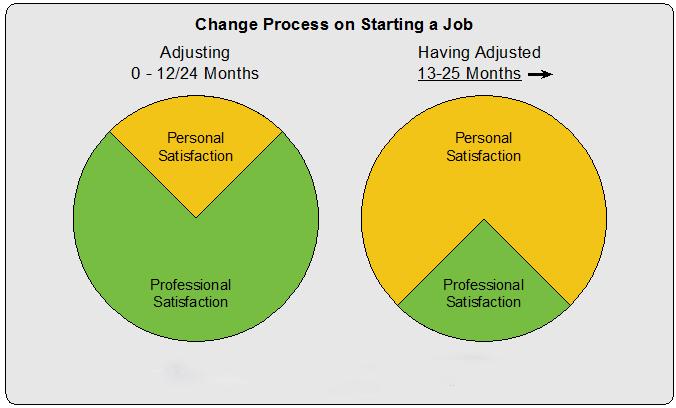 Figure 2: Changes in influence of personal and professional satisfaction on expectations being met over time.
Figure 2: Changes in influence of personal and professional satisfaction on expectations being met over time.
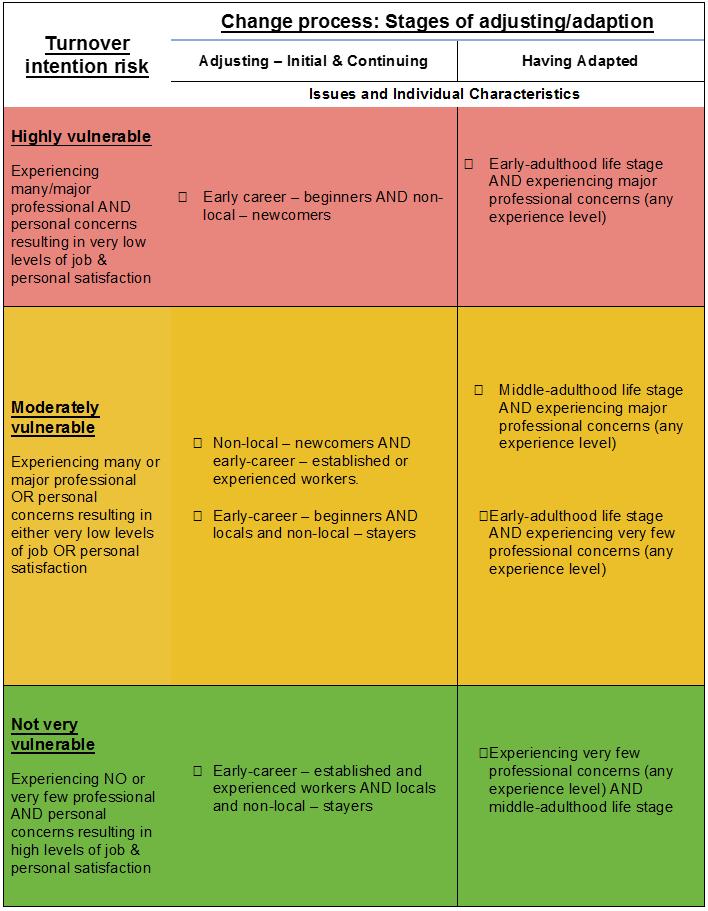 Figure 3: Turnover intention risk matrix.
Figure 3: Turnover intention risk matrix.
Discussion
This study provides a deeper and more nuanced understanding of the full range of life factors (scope of job, workplace relationships, access to CPD, career advancement opportunities and social and personal factors) and how these impact collectively at critical time points in the adjustment process of rural-based, early-career health professionals. It also identifies the major determinants on professional satisfaction for this cohort of workers (level of professional experience and time in the job) as well as on personal satisfaction (time living in the town and current life stage). These determinants were found to strongly affect individuals’ turnover intention risk. The study found that early-career beginners and non-local newcomers were the most at risk of turnover intention and more experienced workers in middle adulthood life stage the least. Interestingly, the study found that rural background (locals) had limited influence on turnover intention and life stage was the primary determinant.
Study limitations
As this was a cross-sectional, qualitative study asking participants to retrospectively discuss elements of their life, recall bias by the experienced participants when reflecting on their early-career experiences is a study limitation. The study is geographically limited by only being undertaken in rural and remote NSW and having very few participants from remote areas (RA4) and none from very remote (RA5) areas. The study’s focus solely on staff working in CMH services and only involving participants from a limited range of allied health disciplines are other notable study limitations. Other rural-based, early-career allied health and nursing professionals working in different public health services, in different health service types or settings, or different Australian states, may have similar or different experiences. To help determine this, future research should extend the study to other Australian states, covering all rural and remote ASCG-RA classifications and including a broader range of health service types. In any future studies, participants should be drawn from a broader range of the allied health professions.
Conclusions
This study offers a holistic explanation of life factors influencing the turnover intention of early-career health professionals working in public health services in rural NSW. These findings and the turnover intention risk matrix are considered suitable for use by Australian public health services and governments as well as other highly industrialised countries, for assistance in the development of policies and strategies tailored for individual health professionals’ work-experience level and life stage. By doing this, health services and governments will better address the life aspirations of rural-based, early-career health professionals and could likely assist in the reduction of avoidable turnover. The study’s key findings and the turnover intention risk matrix have been drawn on by the first author to develop a whole-of-person retention program, which is currently being piloted in two public health services operating in rural Victoria, Australia.
Acknowledgements
The authors acknowledge the early-career CMH professionals who generously gave their time to participate in this study and the NSW rural LHDs that supported its undertaking. We also acknowledge the contribution made by the University of New England’s Collaborative Research Network for Mental Health and Wellbeing in Rural and Regional Communities, which was supported by the Department of Industry, Innovation, Science, Research and Tertiary Education, Commonwealth Government of Australia. The development of this article by the first author was supported by the Australian Government Department of Health through the Rural Health Multidisciplinary Training Programme.