

Introduction
Internal migration is a demographic variable as common as birth and death. This concept is defined as a change of residence within a country. The relationship between health and internal migration is complex. Health status can encourage or prevent internal migration1. Internal migration can contribute to the country’s economy and development if successfully managed. It is considered an integral part of socioeconomic transformation in a country2. It may lead to a positive impact on health when people migrate in order to earn higher income, raise living standards and increase employment opportunities3. The opportunities may be better for health services in the destination place. Living and health conditions may be better and the individual can use health care in need. This situation may be interpreted positively for those who migrated.
Although there are some advantages, internal migration may lead to negative health outcomes in some cases4. If economic weaknesses continue at the destination, it may affect the health of those who migrated. For instance, access to health services is generally better in urban areas in Turkey, but some individuals may not be able to afford the financial costs of health care and their health may deteriorate. Thus, internal migration may negatively affect health status of migrants by causing problems such as in maternal and child health, infectious and chronic non-communicable diseases, occupational health, sexual health and reproductive health5.
The measurement of health status provides important contributions in order to measure the efficiency or effectiveness of medical interventions, assess the quality of health care, estimate the needs of populations, improve clinical decisions and understand the causes and consequences of health differences6. Birth weight, stunting and overweight/obesity of children are among the most important child health indicators that cause concerns all over the world. The assessments of children’s health status are based on these three variables in this study.
An infant’s birth weight is considered an important indicator for survival and future development of children7. Many sociodemographic and socioeconomic factors have received considerable attention for birth weight. Low birth weight is generally associated with numerous factors such as socioeconomic status, calorie intake, urinary tract infection, prenatal care, health service utilization during pregnancy and maternal age8,9. In addition, there are some arguments that special characteristics of urban and rural settings on birth outcomes have been relatively neglected. The place where a pregnant woman lives (urban or rural) may influence the outcome of a pregnancy due to the quality and extent of health services available7. When international literature is examined, there are some empirical studies that show inadequate birth weight differs according to regional differences7,10.
Stunting is defined as the impaired growth and development that children experience from poor nutrition, repeated infection and inadequate psychosocial stimulation. Some consequences of stunting are poor cognition and educational performance, lost productivity and an increased risk of nutrition-related chronic diseases11. Some empirical studies indicate that stunting is higher in rural areas than urban areas, and regional differences (urban-rural, etc.) may be an important determinant for stunting in children12,13. Based on international literature findings, stunting of children may be affected by sociodemographic and socioeconomic factors such as the age of children12,14,15, and maternal education12,16.
Overweight/obesity may influence not only the health and development of children, but have a critical impact on health in adulthood. Obesity may increase the risk of chronic non-communicable diseases and disabilities for children under five in future17. In international literature, the prevalence of overweight/obesity differed in terms of regional differences. A few studies indicate that overweight/obesity of children is higher in urban areas than rural areas18-20. Based on international literature findings, overweight/obesity in children may differ according to various sociodemographic and socioeconomic factors. Age21-24, gender25-28 and maternal education21,22,29 are among those sociodemographic and socioeconomic factors in intenational literature.
This study aims to determine the distribution of birth weight, stunting and overweight/obesity in children under five according to internal migration and various sociodemographic and socioeconomic factors in Turkey. Another purpose of this study is to investigate the course of birth weight, stunting and overweight/obesity in children between 1993 and 2013 in Turkey. Only the migration variable is not sufficient to explain the health status of children. The changes in living conditions are also influential30. Therefore, the effects of various sociodemographic and socioeconomic factors have been investigated on birth weight, stunting and overweight/obesity of children. This study has been carried out on the nationally representative five Turkey Demographic and Health Surveys. In this context, birth weight, stunting and overweight/obesity were examined in children aged less than 5 years.
Methods
The source of data for this study was the nationally representative five Turkey Demographic and Health Surveys (TDHSs) (1993, 1998, 2003, 2008, 2013 TNSA). The Turkey Demographic and Health Survey was conducted by Hacettepe University Institute of Population Studies. The population of the research consisted of women in the reproductive age in the TDHSs, and the information about the health status of children was obtained from the mothers. The sample was 6519 in the 1993 research, 8576 in the 1998 research, 8075 in the 2003 research, 7405 in the 2008 research and 9746 in the 2013 research. In the study, the sample selection was conducted by weighted, multi-stage and stratified cluster sampling approaches.
The data for stunting in children were collected in five periods (1993, 1998, 2003, 2008, 2013). The data for birth weight were collected in the 1998, 2003, 2008 and 2013 periods. The data for overweight/obesity in children aged less than 5 years were collected solely in 2013. Therefore, the variables were examined for the periods when the data were collected.
The dependent variables of the study were birth weight, stunting and overweight/obesity in children aged less than 5 years. The data for the birth weight were collected according to the mothers’ views about the weight of the infant at birth in TDHS research. Stunting in children meant that children, who showed minus two standard deviations (–2 SD) from the median value of the reference group, were ‘shorter’ according to their age. The children who showed minus three standard deviations (–3 SD) from the median value of the reference group were ‘seriously short’ in TDHS research. Overweight/obesity in children aged less than 5 years referred to the children with two standard deviations (+2 SD) above the median value of the reference group in TDHS research.
The independent variables were migration status, study year and sociodemographic and socioeconomic factors. Migration status was examined in four categories according to the women’s childhood residential area. Migration status was determined by women’s childhood residential area. If a woman’s childhood residential area was rural and current residential area was urban, she was included in the category of ‘rural to urban’. If a woman’s childhood residential area was urban and current residential area was rural, she was included in the category of ‘urban to rural’. Moreover, if a woman’s childhood residential area was rural and current residential area was rural, she was included in the category of ‘rural’. In other words, woman had not migrated, and lived in the rural area for a lifetime. In the opposite case, if a woman’s childhood residential area was urban and current residential area was urban, she was included in the category of ‘urban’. In other words, the woman had not migrated, and lived in the urban area for a lifetime31. The sociodemographic and socioeconomic factors differed for each variable. Maternal education, birth order, receiving prenatal care, age of the child, gender of the child, residential area and childhood residential area were involved in the study. The data were gathered by combining data for five periods in order to compare the periodic change of the variables, and to see the effect of each variable.
All statistical analyses were performed using Statistical Package for the Social Sciences v20.0 (IBN; http://www.spss.com). Logistic regression analysis was used in order to determine the effect of migration status, sociodemographic and socioeconomic factors on birth weight, stunting and overweight/obesity in children aged less than 5 years. The analyses were performed in five models. The effect of migration status was examined in model 1. The effect of migration status and study year was examined in model 2. The effect of migration status, period and sociodemographic factors was examined in model 3. The effect of migration status, period and socioeconomic factors was examined in model 4. The effect of all variables was examined in model 5 in order to see the effect of each variable.
Ethics approval
This study was approved by the Institutional Review Board at Hacettepe University Institute of Population Studies. Publicly available secondary data were used in this study. Since the data can be accessed by the requesting researchers, the data is exempted from ethics committee permission.
Results
Table 1 shows the results of logistic regression analysis to determine the impact of migration status, sociodemographic and socioeconomic factors on birth weight of children. Internal migration affected inadequate birth weight. Only the impact of migration status on birth weight of children was examined in model 1. Compared to the children living in urban areas, inadequate birth weight was statistically significantly higher in children living in rural areas (odds ratio (OR): 1.566) and in children who had migrated from urban areas to rural areas (OR: 1.466). OR calculated for children migrated from rural areas to urban areas was not statistically significant. Despite the decrease in ORs for migration status with the increase of the number of variables added, the migration status was statistically significant in all five models.
For the study year variable, it was determined that the 2003 period was significant compared to the reference category 2013 period, and OR was 1.140 in model 5. As birth order increased, inadequate birth weight decreased. In model 5, inadequate birth weight was 1.430 times higher in children with first birth order compared to the children with fourth birth order. Considering model 5, inadequate birth weight was found to be 1.339 times higher in women without prenatal care. It was determined that inadequate birth weight decreased as maternal education increased. According to model 5, compared to the reference category, inadequate birth weight was statistically significantly higher in women with no education or incomplete primary school (OR: 1.922) and women with primary school education (OR: 1.487). In model 5, compared to the west region, OR was statistically significant for the other three regions, except the north region. Considering model 5, OR was 1.862 for the east region compared to the west region.
Table 2 presents the results of logistic regression analysis to reveal the impact of migration status, sociodemographic and socioeconomic factors on the stunting in children aged less than 5 years. The migration status variable was found to be significant in all five models. Considering model 5, rural areas and urban to rural areas were found to be significant compared to urban areas.
Considering the period variable, the stunting was statistically significantly higher in all study years compared to the reference category (2013) in model 5, where all variables were included. Stunting increased with age. Compared to the reference category, stunting was higher in children aged 12–23 months (OR: 3.028), children aged 24–47 months (OR: 4.444) and children aged 48–60 months (OR: 4.448). Stunting was not statistically significant according to sex in all models. Stunting decreased with increasing maternal education in this study. According to model 5, stunting was 3.249 times higher in children of women with no education or incomplete primary school, and 1.665 times higher in children of women with primary school education, compared in children of women with secondary education or higher. Stunting differed regionally. Compared to the west region, stunting was higher in the central region (OR: 1.205) and east region (OR: 1.995) in terms of the residential area. stunting in children was higher in the central region (OR: 1.248) and east region (OR: 1.473) in terms of childhood residential area.
Table 3 demonstrates the results of logistic regression analysis to reveal the impact of migration status, sociodemographic and socioeconomic factors on overweight/obesity in children aged less than 5 years. Obesity was higher in children living in urban areas, and children who had migrated from rural areas to urban areas compared to children living in rural areas.
Overweight/obesity was found to be higher in children aged 11 months and younger, and children aged 12–23 months. The odds ratios were statistically significant for these groups. In terms of gender, females were more at risk. Compared to males, overweight/obesity for height was 1.475 times higher for females, and overweight/obesity for age was 1.710 times higher for females. Overweight/obesity was found to be higher in children who had mothers with higher education. Compared to children in the east region, children in other regions had more overweight/obesity problems. In terms of childhood residential area, overweight/obesity was statistically significantly higher in children whose mothers lived in the west region in childhood compared to the children whose mothers lived in the east region in childhood.
Table 1: Impact of migration status, sociodemographic and socioeconomic factors on inadequate birth weight in children in Turkey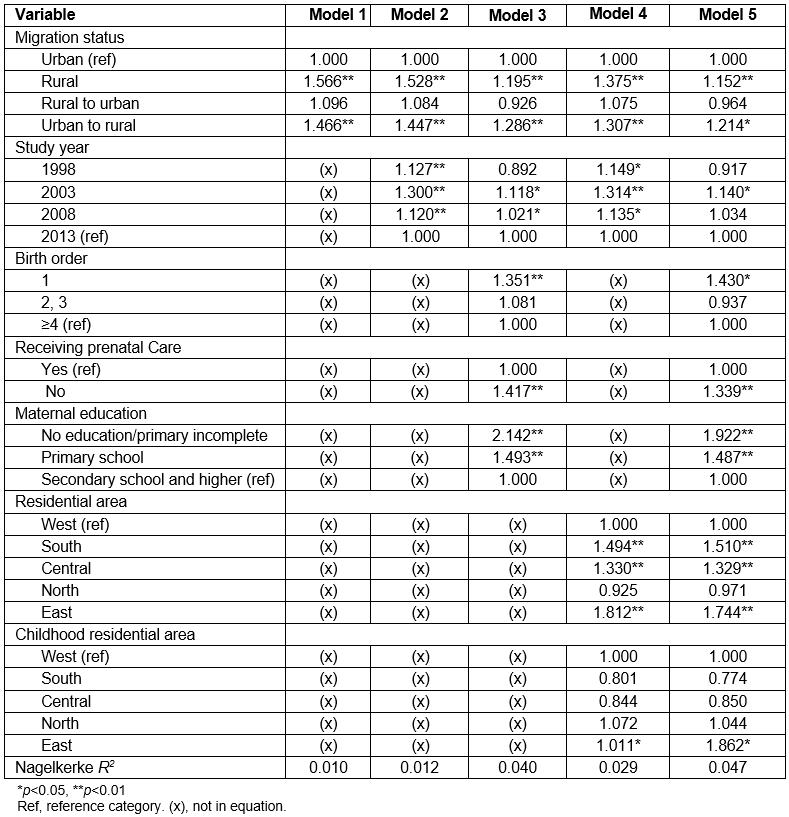
Table 2: Impact of migration status, sociodemographic and socioeconomic factors on stunting in children aged less than 5 years in Turkey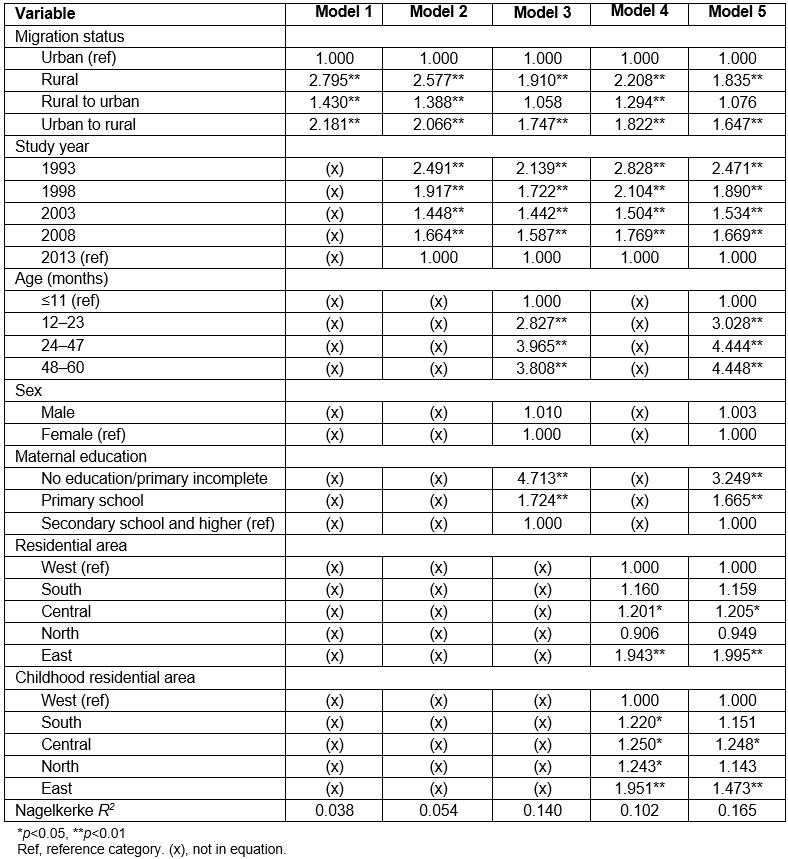
Table 3: Impact of migration status, sociodemographic and socioeconomic factors on overweight/obesity in children aged less than 5 years in Turkey 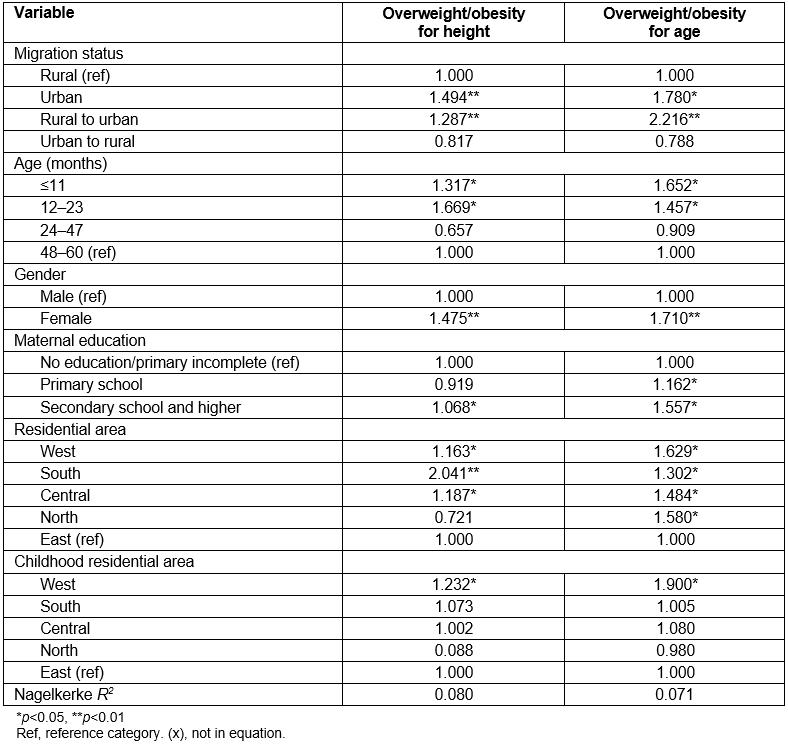
Discussion
The purpose of this study was to determine the distribution of internal migration and sociodemographic and socioeconomic factors on birth weight, stunting and overweight/obesity in children aged less than 5 years in Turkey.
A relationship was found between the birth weight of children and internal migration. The inadequate birth weight was found to be higher in children living in rural areas and in children who had migrated from urban areas to rural areas compared to children living in urban areas. This finding was also supported in another study10. Although not statistically significant, low birth weight has been found to be more common in children living in rural areas7. Prenatal care of pregnant women may contribute to the improvement of pregnancy outcomes. In this process, proper nutrition education and the provision of food supplements may affect birth weight for women. However, the socioeconomic situation is generally poor in rural areas, and women living in rural areas may not use prenatal care services or may use prenatal care services inadequately8. More effective use of prenatal care and primary health care services has the potential to affect inadequate birth weight32. This finding may be related to the mother’s nutrition during pregnancy. Women living in urban areas may have more balanced nutrition during pregnancy and consume more nutrients such as iron and folic acid compared to women living in rural areas. This situation may affect the birth weight.
The impact of internal migration on the stunting was consistent with birth weight, and stunting was higher in rural areas. This finding is supported by other studies12,13. Poor nutrition of migrants might cause significant health problems33. Growth failure may occur due to poor nutrition of children. Unlike birth weight and stunting in children, overweight/obesity was higher in children living in urban areas compared to children living in rural areas. This result was found in many studies18-20. This finding may be associated with the sedentary life of children in urban areas. Technological facilities (such as computers, mobile phones and elevators) become important elements of apartment life. Considering that these technological facilities are more intense in urban areas in Turkey, the children living in urban areas may have less physical activity. The nutrients are stored as fat in children’s bodies, instead of being converted to energy. All these mentioned reasons may trigger overweight/obesity in children living in urban areas.
In this study, inadequate birth weight decreased as the number of births decreased. Other studies also support this finding34-37. This may be related to the frequency of receiving the prenatal care in the first child. The quality of prenatal care and healthcare delivery may contribute to the prevention of side effects during pregnancy. The lack of awareness about the pregnancy process can lead to the low birth weight of a first child. Nutrition of pregnant mothers can be inadequate and unbalanced due to lack of knowledge during pregnancy with a first child. This nutrition may affect pregnancy outcomes37.
In this study, there was a relationship between birth weight and receiving prenatal care. Inadequate birth weight was found to be higher in children of women who did not receive prenatal care. Other studies have shown that timely and adequate prenatal care is important for birth weight8,9,38,39. One of the studies indicated that the frequency of receiving prenatal care might have an effect on birth weight. Compared with women who received prenatal care once, birth weight was found to be six times higher in women receiving prenatal care five times or more35. The purpose of prenatal care is to diagnose and treat any infection that may affect the health of mother or child. The correct diagnosis can only be made by trained medical personnel. The quality of prenatal care can contribute to the birth of babies with normal birth weights38.
The findings of this study revealed that maternal education affected the inadequate birth weight. This finding was consistent with other studies8,38-43. This finding may be related to the tendency of educated mothers to have information about adequate and balanced nutrition, immunization and prenatal care38. As maternal education increased, stunting reduced in children. Similar findings were found in other studies12,16. Educated mothers may play an important role in the problems related to malnutrition, and may contribute to the reduction of the prevalence of stunting by paying attention to the health of their children29. Overweight/obesity increased with increasing maternal education in children. In one study, a relationship was found between higher prevalence of obesity and high education21. However, other studies support the opposite and reveal that highly educated families have a lower risk of obesity in their children22,29.
In the study, birth weight and stunting differed according to the region in which the child was born. The number of inadequate birth weights was higher in the east region. The east region is among the regions where prenatal care services are received at low levels in Turkey. Low levels of regular pregnancy follow-up have the potential to affect the birth weight of women living in the east region. However, delivery rates are also known to be high due to lack of qualified family planning in women in the east region. These consecutive births may affect the pregnancy outcomes and may cause other babies to have a low birth weight. The short duration between two births may affect the birth weight of children. Similarly, stunting was found to be higher in the central region and the east region in Turkey. Chronic malnutrition is one of the important causes of stunting in children aged less than 5 years44. Nutrients (especially vitamins) should be part of a child’s nutrition program in order to protect the skeletal system and protect against cognitive decline, autoimmunity, cardiovascular diseases, etc. Maternal education may contribute to and support adequate and balanced nutrition for children. Since maternal education is generally at a low level in the east region, it may cause some disadvantages and inequalities for the east region in Turkey.
The prevalence of overweight/obesity differed in terms of residential area. Based on the findings of this study, the overweight/obesity problem was higher in other regions compared to the east region. Obesity rates are generally higher in urban areas in countries with low levels of income. Turkey is among those countries. It is easier to access cheap but unhealthy foods for children living in urban areas. Unhealthy eating habits in children (‘junk’ food, fast food, fizzy drink consumption, etc.) may be higher in the west region with the impact of urbanization and economic development. This may lead to a high risk of overweight/obesity in the west region.
Stunting increased with the age of children. Other studies also supported this finding12,14,15,45. This finding may be explained by the protective effect of breast milk on growth and development in the early stages of life. Women may use supplementary foods after 12 months for their children. These supplementary foods may lead to inequality of nutrition between children. Also, obesity increased with the increasing age of children. Other studies also supported this finding21-23. It may be related to increased mobility of children. Children want to move more when they are able to crawl and walk. So, this situation may contribute to the reduction of overweight by causing energy transformation.
Sex was found to be a significant determinant of overweight/obesity in children aged less than 5 years. In this study, overweight/obesity was higher in females compared to males. Other studies also found that females were more obese compared to males25-27. This finding may be related to different biological characteristics of males and females. While fat tissue and distribution may be higher in females than in males, muscle distribution in males may be more than in females28.
Conclusion
This study revealed the interregional disparities in terms of children’s health status in Turkey. East and central region swere disadvantaged regions in terms of the indicators of birth weight, stunting and overweight/obesity in children aged less than 5 years. The study shows that there is a need for policymakers to overcome the regional disparities that create disadvantages in rural areas. The authors suggest measures to encourage adequate and balanced nutrition and/or increases in physical activity. Childhood obesity has critical impacts on health in adulthood. Therefore, stakeholders should come together to reduce overweight/obesity in children living in urban areas. Individuals, government, media and the food industry are among those stakeholders. The consumption of ready-to-eat foods should be reduced for the children with the help of realistic health and food policies.
According to another important finding, improvements in health status indicators increased with maternal education. Only overweight/obesity was higher in children of educated mothers, unexpectedly. There have been concrete steps in the field of education in Turkey. Compulsory education, public education centers for women and literacy campaigns are among those steps. Increasing education level and health literacy levels can lead to development of child health. Family health and community health centers should be considered as an important strategic step that facilitates the provision of health education for women at different levels of literacy. In these centers, training programs and training materials can be prepared for women to improve maternal and child health. In particular, since receiving prenatal care affects the birth weight of children and shaping the health of children in later years, raising the awareness of mothers is an important issue.
Because TDHS data has been used in this study, the study was designed within the framework of secondary data. So, the migration status was determined according to the women’s childhood residential area. In future studies, migration status could be investigated according to information about migration carried out at least once in the last five years, lifelong migration and migration by previous residential area. Future studies may include the experiences of children and women on internal migration, and the experiences of migrants in access to health services.
References
You might also be interested in:
2015 - Indonesian medical students' preferences associated with the intention toward rural practice