
Introduction
From a public health point of view, injury should be regarded as a ‘disease’ rather than an accident. This disease currently represents the leading cause of death of children, adolescents and young adults, and is the eighth leading cause of death for all age groups1. Road traffic injuries (RTIs), being the leading mechanism of major trauma, claim more than 1.35 million lives each year1. In low- and middle-income countries, the phenomenon of rapid motorization necessitates actions and measures to make roads safer. The problem should be addressed in a holistic manner, which requires designing safer infrastructure and incorporating road safety features into land-use and transport planning, improving vehicle safety standards, improving post-crash care for trauma patients, setting and enforcing laws relating to key risks, and raising public awareness2.
Efforts during the last decade have resulted in a plateau regarding road traffic fatalities, which has been welcomed as a first step but it is not enough. Unfortunately, the ambitious goal set by WHO in 2015, which was a 50% reduction in road traffic-related deaths and injuries by 2020, is unlikely to have been met1,3. However, progress made during the previous Decade of Action for Road Safety 2011–2020 has encouraged WHO to take accelerated action in the years ahead. In August 2020, the United Nations General Assembly proclaimed the Decade of Action for Road Safety 2021–2030, with the ambitious target of preventing at least 50% of road traffic deaths and injuries by 20303. Greece faces the effects of road traffic accidents (RTAs) to a great extent every year. Greece was committed to reduce fatalities to fewer than 640 by 2020. Despite the significant progress that has been made during the last decade, this goal is unlikely to have been achieved4.
Injuries usually follow a pattern that is influenced by a variety of causative factors. These include age, gender, social and demographic factors, and alcohol and drug abuse. By studying the patterns of occurrence within a given population, one can identify potential ways of controlling, mitigating or modulating them, with the aim of reducing the health burden of injuries5.
In order to prevent RTAs and mitigate their consequences, it is necessary to systematically analyze them at a macro- and micro-scopic level. The macroscopic level is served by the data collected from the total of road traffic incidents by the traffic police, which are analyzed by the Hellenic Statistical Authority (ELSTAT). At a microscopic level, the Hellenic Institute of Transport collects and keeps a record from a sample of the accidents, thus providing an in-depth analysis. Unfortunately, in Greece no electronic national trauma registry has been implemented throughout healthcare facilities6. Consequently, in the absence of an established national trauma registry, regionally developed hospital-based trauma registries represent the only means of injury surveillance6-9. Prionas et al performed a systematic review of published trauma registry literature from Greece in 2018 and concluded that trauma auditing in Greece is still in an embryonic state6.
The present study represents an epidemiological approach to RTIs presenting to a secondary hospital located along the North Road Axis of Crete; the study aims to describe the pattern of occurrence of RTIs and indicate possible preventive measures and actions.
Methods
Study design
The study was conducted in Rethymnon General Hospital between January 2018 and February 2020. Data from all trauma patients who presented to the emergency department (ED) after RTAs were retrospectively collected from patients’ medical records. Information was recorded regarding patient demographics (age, gender), type of accident (automobile, motorcycle, bicycle, pedestrian), timing of the accident (tourist season vs rest of the year, weekdays), mode of arrival to the ED (ambulance vs other means), type and severity of injuries, treatment details, emergency operations, length of hospital stay and final outcome. Patients were divided into three age groups based on life circumstances and habits as well as the legislation on driving licenses in Greece: ≤17 years (mainly students who are only entitled to drive bicycles or motorcycles up to 50 cm3), 18–67 years (working adults), and ≥68 years (elderly citizens who are usually retired). The severity of injury was graded using the Injury Severity Score (ISS), which remains the most widely used anatomical scoring system5,10.
Definitions
RTI was defined as any injury caused by a crash originating from, terminating at or involving a vehicle partially or fully in a public pathway11. Specific RTIs were defined as follows12:
- Pedestrian injury: an injury that is associated with a vehicle while the victim was not riding in or on the vehicle; includes injuries while standing, walking, running, roller skating or skateboarding, as long as the injury is associated with a vehicle.
- Motorcycle-related injury: an injury that is associated with operating or being a passenger on a motorcycle; includes injuries from falls or burns while riding a motorcycle.
- Bicycle-related injury: an injury that is associated with riding or being a passenger on a bicycle; includes injuries from falls or burns while riding a bicycle.
- Automobile-related injury: an injury that is associated with operating or being a passenger in or on a motor vehicle other than a motorcycle; includes any injury associated with cars, buses, mini-buses, trolleys, street cars and trains.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences v23 (IBM; https://www.ibm.com/products/spss-statistics). Categorical variables are presented as absolute number and percentage n (%) and continuous variables are presented using mean (±standard deviation) or median (interquartile range) for variables having non-normal distribution. Chi-square tests were performed to compare categorical variables and Cramer’s V coefficient is presented as a measure of association. For continuous variables, non-parametric tests (Mann–Whitney U-test and Kruskal–Wallis test) were performed whenever the assumptions of normality for independent sample t-test were not met. Post-hoc analysis was used in order to determine which category of a variable was responsible for a statistically significant result. A two-sided significance level of 0.05 was used for all statistical tests.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki of 1975 and its amendments in 1983. Permission for the study was obtained from the institutional review board (Rethymnon General Hospital, approval number 17/05-02-2020).
Results
During the study period, a total of 1582 trauma patients presented at the ED of the hospital after RTAs. There were 1079 male patients (68.2%) and 503 female patients (31.8%) and the median age was 30 years (IQR=26). Most of the patients (n=1275, 80.8%) were adults between 18 and 67 years, 194 (12.3%) were less than 17 years and 108 (6.8%) were seniors older than 68 years. Motorcyclists accounted for most of the study population. Of the 1582 traffic accident victims, 818 were motorcyclists (51.7%), 497 were car occupants (31.4%), 165 were cyclists (10.4%) and 102 were pedestrians (6.4%). RTAs were unevenly distributed throughout the year with the majority (n=1001, 63.3%) taking place during the tourist season (May to October) and far fewer (n=581, 36.7%) during the rest of the year. Regarding transportation to the ED, 601 patients (38%) were transferred by ambulance and 981 (62%) were transferred by other means. Demographic data of the study population and accident data are presented in Table 1.
Isolated injuries were present in 670 patients (42.7%). Extremity injuries predominated in 921 patients (58.2%). Furthermore, 554 thoracic injuries (35.3%), 541 head injuries (34.4%), 271 facial injuries (17.4%), 203 abdominal injuries (12.9%) and 162 pelvic injuries (10.3%) were recorded. The overall median ISS was 2 (IQR=4). In six cases, emergency operations were necessary (0.3%). The median ISS in those cases was 14.5 (IQR=15). A total of 1123 patients were discharged from the ED after the evaluation was completed, while 405 others were admitted (25.6%). The median length of stay was 3 days (IQR=6). Transportation to a tertiary hospital was necessary in 41 patients (2.6%) who presented a median ISS of 17 (IQR=12). Finally, death in the ED was recorded in 13 patients (0.8%) who presented a median ISS of 75 (IQR=75). Table 2 summarizes data regarding initial patient condition, type of injuries sustained and final outcome.
Statistical analysis identified significant association between patient age group and type of accident (p<0.001; Cramer’s V=0.30, p<0.001). Most patients under 17 years were injured while riding bicycles (42.3%); most adults were involved in motorcycle-related accidents (56.5%). Furthermore, significantly more injured pedestrians than expected belonged in the age group >68 years (19.4%). A statistically significant difference in ISS between different age groups (p=0.008) was also found. Post-hoc analysis on each pair of groups provided strong evidence (p=0.007) that individuals younger than 17 years tend to present with significantly lower ISS than seniors older than 68 years.
Moreover, patient gender presents a statistically significant association to the type of accident (p<0.001; Cramer’s V=0.265, p<0.001). Specifically, men suffer mainly motorcycle-related injuries (59%) while women mainly suffer automobile-related injuries (43.3%). Furthermore, male patients presented significantly higher ISS than women (p=0.001).
The differences in type and severity of RTIs between the tourist season (May to October) and the rest of the year (November to April) was also investigated. When the type of accident was compared with the period of the year, no statistically significant difference (p=0.196) was found. Additionally, there was no statistically significant variation in ISS between the different periods of the year (p=0.751).
The frequency of RTAs over the days of the week was also recorded: 239 RTAs took place on Monday (15.1%), 199 on Tuesday (12.6%), 212 on Wednesday (13.4%), 221 on Thursday (14.0%), 212 on Friday (13.4%), 241 on Saturday (15.2%) and 258 on Sunday (16.3%). Further analysis showed that there was no statistically significant variation in the ISS of patients over the days of the week (p=0.268).
Furthermore, patients who were transferred to the ED by ambulance had a significantly higher ISS than those who arrived by other means (p<0.001). However, the majority of patients transferred by ambulance (53.7%) still had ISS≤4. A statistically significant association was also found between the type of accident and transportation by ambulance (p<0.001; Cramer’s V=0.192, p<0.001). In the majority of accidents involving motorcycle or bicycle driving (64.7% and 83.9% respectively), the patient arrived in the ED not by ambulance but by other means of transportation.
Finally, a significantly higher ISS in patients after motorcycle-related accidents was identified compared to those presenting after automobile-related accidents (p<0.001).
Table 1: Demographics of 1582 consecutive trauma patients and characteristics of related road traffic accidents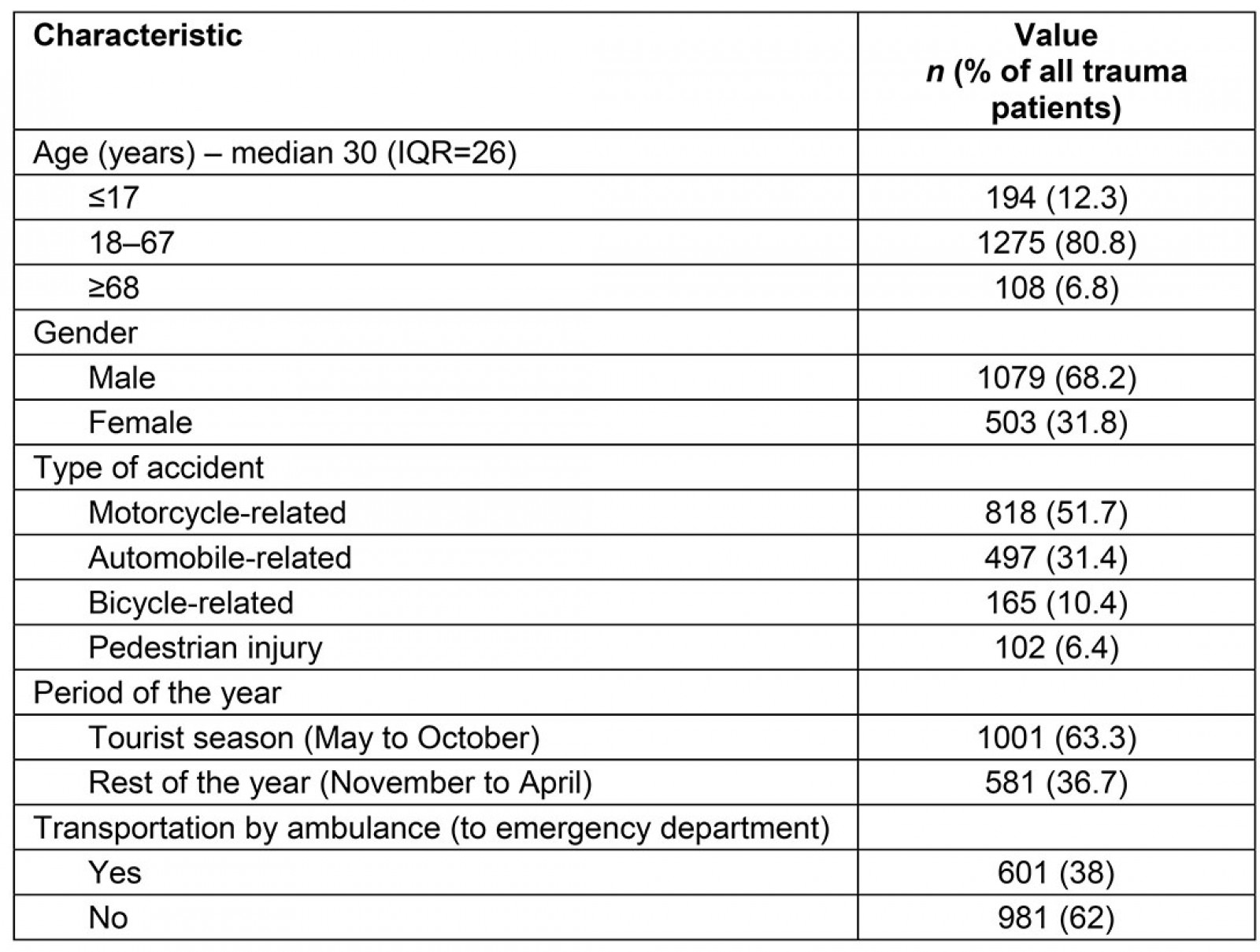
Table 2: Initial condition, type of injuries sustained and final outcome of 1582 consecutive road traffic victims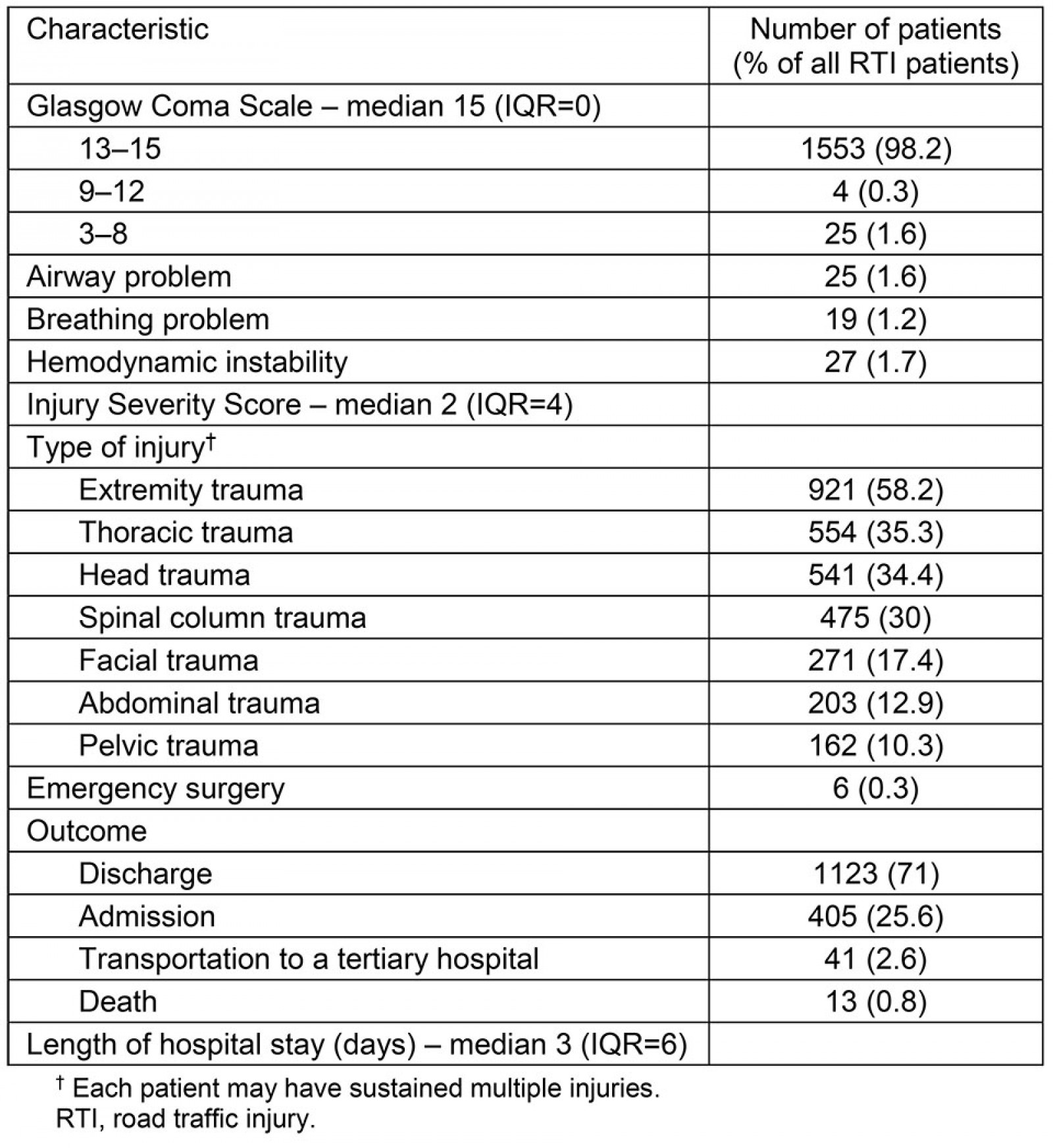
Discussion
Deaths and injuries resulting from RTAs remain a serious concern globally despite the integrated approach implemented by WHO, and current trends suggest that this will continue to be the case at least in the near future1. In Greece, road traffic-related deaths have been significantly reduced, from 1456 in 2009 to 688 in 2019, according to ELSTAT4. This decrease is the result of implementing increased law enforcement strategies, the upgrade of the motorway infrastructures and the Greek financial crisis13,14. Specifically, the island of Crete presents a disproportionally high rate of RTAs and fatalities, given its surface area and population size. Possible explanations of this phenomenon include the dramatic increase in population during the tourist season as well as the low quality of the existing road network. Road network characteristics include, but are not limited to, one-lane roads with no barriers or guardrails, road surface disintegration with potholes and cracks, poor or absent lighting and blind curves. For example, the North Road Axis of Crete is notorious for being one of the deadliest roads in Greece. It is indicative that 49 people lost their lives in RTAs in Crete during 2019, corresponding to 77.2 mortalities per million inhabitants4.
ISS was used to classify injury severity in the present study. ISS summarizes a person’s injuries calculated as the sum of the three highest Abbreviated Injury Scale scores squared in different body regions10. Given the retrospective nature of the study, an anatomical scoring system was chosen over physiological ones. Scoring systems combining anatomical and physiological data were not used because of their complexity. Among anatomical scoring systems, ISS was chosen over the Maximum Abbreviated Injury Scale (MAIS) as a better aggregator for use in the clinical setting. In other settings such as automotive design and occupant protection, MAIS is a useful tool for comparing specific injuries and their relative severity and the changes in those frequencies that may result from evolving motor vehicle design. It is noteworthy that MAIS was adopted by the European Commission in 2013 for the definition of serious injuries15. However, MAIS ignores information provided from other injuries5.
The incidence of RTAs in the district of Rethymnon follows a seasonal pattern, displaying a substantial increase during the tourist season. While on vacation, people tend to travel more, use unfamiliar road networks and increase their alcohol consumption. This seasonal pattern is also common among other countries in the same geographical region16. Although it has been suggested that poor weather and road surface conditions during winter (slippery surface and decreased daytime illumination) pose an increased risk of RTIs for drivers, especially motorbike riders17, this correlation has not been confirmed in other studies, including this one18. Moreover, the type of accidents and the severity of injuries were similar between the tourist season and the rest of the year. It should be stressed that the almost twofold increase in the number of incidents during the tourist season must be dealt with by an already understaffed hospital. Consequently, the highest priority should be given to hospital staffing, especially departments responsible for trauma care.
Regarding time distribution of RTIs over weekdays, it has been reported that RTIs are both more frequent and more severe during weekends18,19, and there is a pronounced increase in RTA rates during the course of week, with each weekday from Monday to Friday being significantly higher than the previous one20. Contrary to previous studies, the current results did not indicate significant variation in the frequency of RTIs or the relevant ISS over the days of the week.
Distribution of RTAs by age revealed that bicycle-related accidents were more frequent among young individuals, motorcycle-related accidents were more frequent among middleaged individuals and pedestrian injuries were more frequent in the elderly. Furthermore, individuals younger than 17 years presented with less severe injuries than seniors older than 68 years, despite the fact that the former are prone to aggressive driving behavior in conjunction with minimal driving experience. The current findings are in accordance with those of other studies that have highlighted the role of age in the outcome of injured persons17,18,21. A possible explanation is that elderly people are more vulnerable due to decreased reflexes, vision or hearing impairment, decreased physiologic reserves and chronic medications such as antithrombotic and psychoactive drugs22.
Significant differences were also found regarding the type of accident. Motorcycle/bicycle-related injuries in the cohort represented 62% of the total, a percentage similar to previous reports from the same region but significantly higher than that from other European and non-European countries23. Specifically, motorcycle accidents were associated with more severe injuries than automobile accidents. In fact motorcycle/bicycle-related injuries were responsible for the majority (69%) of fatalities in the present study, whereas the corresponding percentage on a national basis is 36.5%, as low as 16% for the whole of Europe and 28% globally1,4. It is indicative that in 2016 Greece ranked first among all EU countries in the death rate per population of motorbike drivers. Supporting evidence is also provided by Anagnostou et al, who found a fivefold and threefold risk of death for bicycle and any kind of motorcycle driver, respectively, when compared to cars. According to the authors this discrepancy is mainly attributed to the exposed position of motorcycle drivers and passengers, along with the non-use of protective equipment and illegal driving behavior18. According to WHO, although Greece has adopted national motorcycle helmet laws, helmet-wearing rate is 75% for drivers and only 46% for passengers, whereas the relevant enforcement rating is only 4 out of 101. Consequently, traffic police should aim to upgrade the level of law enforcement regarding the safety of road users with emphasis on motorcycle drivers and passengers. Moreover, implementation of road safety educational strategies and upgrade of infrastructure are needed to reduce the impact of motorcycle/bicycle-related injuries.
Regarding gender, the majority of injured patients and, most importantly, 11 out of 13 fatalities, were men. Moreover, male gender was associated with a higher ISS, indicating a tendency towards more severe injuries. According to WHO, 73% of all road traffic deaths occur among young males under 25 years24. Possible explanations for the male predominance include non-use of seatbelts and helmets, as well as driving under the influence of alcohol or drugs, characteristics that are more frequently noticed among men18. Alonso et al found that the perception of risk of traffic accident as a result of driving under the influence seems to be higher in women than in men25. Male gender also presented a strong association with bicycle-related injuries, whereas women were more frequently implicated in automobile accidents.
Another interesting observation is that although patients transferred to the ED by ambulance had suffered more severe injuries, 54% of them still had an ISS≤4, which means that they had sustained either light injuries or no injuries. It should be noted that the whole region of Rethymnon is covered by only two ambulances. Given that ambulance shortage remains a matter of life and death in prehospital care in Greece, the aforementioned observation should be seriously taken under consideration. Of course, the primary aim should be to strengthen the capabilities of the National Center for Emergency Care’s ambulance fleet. Also, educational strategies and information campaigns should be implemented that aim to confront inappropriate ambulance use.
Regarding the outcome, it must be stressed that the decision for transportation to a tertiary center was made due to lack of appropriate specialty healthcare facility (mainly neurosurgical and spinal surgery services) or lack of available ICU bed in the hospital and not trauma severity. Among 541 patients with head injury, 47 were diagnosed with either intracranial hemorrhage or skull fractures. Unfortunately, these patients do not have immediate access to neurosurgical attention in Rethymnon General Hospital. In 19 of them, transportation to a tertiary center with neurosurgical services was necessitated, one patient died and the other 27 were admitted to the hospital’s surgical department for observation.
Before drawing any conclusions from the abovementioned findings, a list of study limitations should be taken into account. These include the retrospective manner of data acquisition. Important information regarding the circumstances of the RTAs was not available, given the resource-limited setting under which the study was conducted. Moreover, no data were collected about lifelong disabilities or psychological trauma from RTIs. Additional details that ideally should be provided by a trauma registry include, but are not limited to, the location of the accident (urban or rural area) and long-term follow-up data regarding the severely injured trauma patients. Finally, statistical processing was restricted to univariate analysis, which did not permit adjusting for confounding factors.
Conclusion
In conclusion, the healthcare burden of RTIs in the district of Rethymnon calls for urgent action from the state and relevant authorities in the following directions: first, traffic police should aim to upgrade the level of law enforcement regarding the safety of road users, especially motorcycle drivers and passengers. Moreover, educational strategies and information campaigns should be implemented to deal with inappropriate ambulance use. For as long as an established national trauma registry does not exist, regional health facilities should be encouraged to develop trauma registries as the only means of injury surveillance. Finally, the overwhelming burden of RTAs, especially during the tourist season, for a secondary hospital with significant lack of personnel should be strongly considered. Consequently, adequate hospital staffing with emphasis on ED organization is paramount.