

Introduction
Type 2 diabetes mellitus (hereafter ‘diabetes’) is currently one of the fastest growing health emergencies in the world. The International Diabetes Federation reported that diabetes caused approximately four million deaths in 20191. India has experienced a large increase in non-communicable diseases in the past several decades2, and now has the second greatest number of people with diabetes in the world at 77 million individuals1. This number is expected to increase to over 101 million people with diabetes in the next 10 years1. Broader societal processes such as urbanization and globalization, along with dietary changes and declining physical activity, have been primary drivers of the diabetes epidemic in low- and middle-income countries such as China and India3. Risk of developing diabetes is dependent on both modifiable factors (eg lack of physical activity and obesity) and non-modifiable factors (eg age and family history of diabetes)4. Diabetes carries a large economic burden due to disability and death from several complications, including retinopathy, kidney failure, and heart disease, among others5. The long-lasting pathology of disease complications can have severe impacts on individuals, families, communities, and healthcare systems. Individuals with diabetes from families of low socioeconomic status, who already face financial hardships, often spend as much as 60% of their household income to care for family members with diabetes3.
Many studies have shown that diabetes is an increasing concern in South India, and especially in the state of Tamil Nadu2,6,7. Diabetes affects approximately 4.8 million individuals in Tamil Nadu8, with a current age-standardized prevalence of 10.8%7. The increasing prevalence of diabetes in Tamil Nadu has been associated with increased waist-to–hip ratio, BMI, tobacco consumption, urban residency, decreased physical activity9, as well as male sex, age, obesity, scheduled castes, family history of diabetes4,10, alcohol intake, and hypertension11.
The low awareness of diabetes and prediabetes in India has also been highlighted in several studies12-17. Low awareness can lead to high prevalence of undiagnosed diabetes, which is a serious public health concern; indeed, estimates suggest that approximately half of diabetes cases are undiagnosed in India18. It is therefore necessary to investigate both the level of awareness of, as well as factors associated with knowledge of, diabetes, to identify priority areas for targeting educational campaigns, public health surveillance, and diabetes screening. This is particularly true in rural and socioeconomically disadvantaged regions, where limited access to education and healthcare resources is a substantial barrier to health literacy and diabetes awareness19,20. Within this context, the primary objectives of this study were to assess the overall awareness of diabetes, and to determine associations between sociodemographic factors and diabetes knowledge in a rural population located in north-western Tamil Nadu. With a high statewide prevalence of diabetes7, it is increasingly important to ensure relevant health education is targeted towards high-risk groups in Tamil Nadu to mitigate the ongoing diabetes epidemic.
Methods
Study design and data collection
Data were collected as a component of a cross-sectional health study conducted in 17 villages in a rural region of Krishnagiri District, Tamil Nadu9. Previous publications using these data have identified and discussed other specific health outcomes from this study, including newly diagnosed diabetes9, overweight and obesity21, and anemia22; however, this analysis is the first conducted on diabetes awareness using this dataset. Specific sampling techniques, including a sample size calculation, as well as other data collection methods, are described in detail elsewhere9. In brief, the research team conducted systematic random sampling to recruit adult participants (≥19 years) using the Kish method23. Following recruitment and informed consent, a survey was administered to participants by a trained researcher to collect information on demographics, occupation and livelihood characteristics, self-reported health, and household assets. Knowledge on diabetes was assessed using a validated questionnaire developed by Mohan et al (2005), which consisted of five questions assessing awareness of diabetes, including symptoms, causes, and complications24.
Definitions and explanations of variables
Although all villages included in the study were rural by the definition as described by the Census of India, the rurality of each village was assessed as a predictor variable using a rurality index, adapted from Weinert and Boik25. The two variables incorporated into the rurality index were distance to the primary healthcare center (given half a positive weighted value), and the population size of each village (given a full negative weighted value). The results were standardized to a mean of zero and standard deviation of one, with a positive score indicating a more rural residence, and a negative score reflecting a less rural residence.
Data on household assets and community facilities (such as toilet facilities and water pumps, if applicable) were collected to assess socioeconomic status. These data were collected using an adapted questionnaire from the second National Health and Family Survey, originally consisting of 29 questions to create a Standard of Living Index26. Those questions relevant to the study population were used, with a total of 13 weighted questions for a maximum score of 26. Weights of items such as type of housing, community or household water and toilet facilities, household possession of televisions/radios, and ownership of livestock, were developed by the International Institute of Population Sciences in India and based on a priori knowledge of the significance of each indicator in determining household socioeconomic status27.
Additional demographic information was collected from each participant, including religion, caste, and sources of income in the previous year. Time per day spent watching TV and information on health-seeking behaviour (type and frequency of healthcare sought) were collected. Religion was assessed as a binary variable (Hindu or ‘other’), and caste was given the categories of low caste (scheduled tribes and caste), lower-middle caste (backwards castes, most backwards castes, other backwards castes), middle-upper caste (general category), and high caste (Brahmin caste). Data on occupation were collected by asking about sources of income within the last year, including local labour, agriculture, livestock, migrant work, merchant work, shop/small business, government schemes, or Mahatma Gandhi National Rural Employment Guarantee Act (MGRNEGA). For ease of interpretation, livelihood information was given the categories of local labour, farming (agriculture and/or livestock), migrant work, business (merchant and/or small business owner), and government funds (MGNREGA and/or other government schemes) and assessed as binary variables (‘yes’ or ‘no’ for each individual source of income). Time per day spent watching television was collapsed into four categories: less than 0.5 hours per day, between 0.5 hours and 1 hour per day, more than 1 hour and up to 2 hours per day, or more than 2 hours per day.
Age was categorized into four groups – 20–34, 35–49, 50–64, and ≥65 years – based on similar methods used by Shrivastava et al16 and Murugesan et al13. Type of health care typically accessed included government, private, natural (ie ayurvedic and/or other alternative medicines), and none, and each was assessed as a binary variable. Frequency of healthcare visits was collapsed into three categories: once a month or more, less than once a month but more than once a year, and once a year or less. Information on school grade achieved was collected and had a range of 0–15, with anything greater than 12 indicating post-secondary education. For ease of interpretation, this variable had the categories of no schooling, primary education (grades 1–8), secondary education (grades 9–11), and graduate or post-secondary education (grades ≥12), based on similar methods used previously among Indian populations13,24.
Knowledge on diabetes was collected using a validated questionnaire developed by Mohan et al (2005)24, and included questions about diabetes such as risk factors, complications, and prevention. The first question, ‘Do you know what diabetes is?’ acted as a screening question such that those who answered ‘no’ were automatically given a score of 0 and did not answer the remaining questions. For each response, weights were applied according to Mohan et al (2005) to calculate a composite knowledge score ranging from 0 to 824.
Statistical analysis
Data were cleaned using Microsoft Excel. All statistical analyses were conducted using Stata/IC v16.1 (StataCorp; http://www.stata.com). Due to zero inflation and heteroscedasticity of residuals, a linear regression model was not appropriate to model the composite knowledge score as a continuous variable. Therefore, diabetes knowledge had the categories of score of 0 (no knowledge), scores of 1–4 (moderate knowledge), and scores of 5–8 (good knowledge) for all statistical models.
Descriptive analyses were first conducted to establish the sociodemographic characteristics of the study population, overall diabetes knowledge scores, knowledge scores broken down by education level, and the proportion of the study population who answered questions correctly in the diabetes knowledge questionnaire. Following this, collinearity was tested by calculating the intraclass correlation coefficient. A coefficient higher than 0.8 was the cut-off point used to determine collinearity between variables. The linearity assumption was also tested against continuous predictor variables (such as age) and the log-likelihood of the outcome. Because the outcome variable contained three categories, a normal logistic regression could not be used to test linearity. Therefore, each predictor variable had to be tested against binary categories of the log-likelihood of the outcome (ie knowledge score in category 1 v 0, 2 v 0, and 1 v 2) using logistic regression. A LOWESS curve was first used to assess the linearity assumption, followed by the inclusion of a quadratic term. Variables that proved to be non-linear and could not be modelled with a quadratic term were then categorized.
To control for confounding bias, all individuals with self-reported diagnosed diabetes were omitted from the data analysis. All sociodemographic factors were then fit for univariable analysis with the outcome, using ‘no knowledge’ as the referent outcome category. These variables included age, sex, wealth index, education, religion, caste, methods of earning income, rural index, television exposure, and type and frequency of healthcare usually received. Only independent variables significant to a liberal p-value of 0.2 were short-listed for inclusion in the initial multivariable model.
Following this, a manual backward elimination method was used to fit an adjusted multinomial regression model to assess associations between sociodemographic factors and knowledge score categories, with a knowledge score of zero as the referent. Due to clustering of the data by village, village was added to the model as a random effect variable. To incorporate the use of a random effect in a multinomial model, the Stata program GLLAMM was used to fit a generalized linear latent and mixed model, using village as a discrete random effect, and knowledge score as a polytomous outcome with the mlogit link. Adaptive quadrature was also used to ensure the most precise estimates were given for the log-likelihood of the two-level model28. Following the backward elimination process, each variable was removed independently from the full model and the partial model was then tested for significance (p<0.05), using likelihood-ratio tests and Wald tests. As each variable was removed from the model, it was simultaneously tested for confounding by determining if any coefficients of interest changed by 20% or more following exclusion. All plausible interactions were then generated and assessed for significance using a p-value of <0.05. No confounding was found to be present, and no interaction variables were statistically significant in the adjusted multinomial model.
After the multinomial model was finalized, diagnostics were performed for GLLAMM using the gllapred command28. Upper residuals (empirical Bayes predictions) were produced, along with Pearson and deviance residuals. Upper residuals were tested for homoscedasticity and normality, and Pearson and deviance residuals were used to assess outliers and their impact on the model. There were no outliers with a strong enough impact to justify their removal from the model, and no participants with a missing knowledge score. Therefore, only participants who did not fit the inclusion criteria for the model (ie were previously diagnosed with diabetes) were removed for analysis.
Ethics approval
This study received ethics clearance for research on human participants from the University of Guelph Research Ethics Board (certificate 12MY023). Permission for the study was granted by the High Commission of India in Ottawa, Canada. Upon arrival to the research site and prior to the recruitment process, researchers sought and received permission for the study from local authorities (panchayat councils, local police officials, and hospital medical staff). Informed verbal consent was obtained from all research participants prior to enrollment in the study.
Results
The response rate among the 812 recruited individuals was 92.7%, with 753 individuals completing the diabetes knowledge survey (341 males and 412 females). Descriptive characteristics of the study participants are presented in Table 1. The average age of participants was 47 years (standard deviation ± 14.7 years). Over half of the population (59.1%) had no formal schooling, with only 35.1% reporting full literacy (could read and write). Only about one-third of the population reported knowing about diabetes. More men reported having any knowledge of diabetes when compared to women (36.9% v 30.3%); however, this difference was not significant. Those who reported being aware of diabetes were invited to participate in the full diabetes knowledge survey. Full results of the diabetes knowledge questionnaire are reported in Table 2.
Of those who reported awareness of diabetes, 62.6% answered ‘yes’ to the question, ‘Do you know if diabetes is increasing?’. About half of the participants who were aware of diabetes believed that it is preventable. In total, only 16.4% and 17.0% achieved moderate and good knowledge scores, respectively. Even among those with the highest level of education, 42.2% did not know what diabetes was.
Literacy and education had high collinearity (intraclass correlation coefficient of 0.84), leading to the omission of literacy as a predictor variable. After individuals with self-reported diagnosed diabetes were removed, 705 individuals were included in statistical analyses. After assessing univariable analyses of each predictor variable, all variables were included for multivariable analysis except religion, television exposure, and migrant work as a source of income. The final multinomial regression model is presented in Table 3. Wealth, education, rurality, frequency of healthcare visits, ownership of a business, and government funds as a source of income were all associated with moderate and/or good knowledge of diabetes in the final model. Notably, education was strongly associated with a good knowledge score in the final model. Specifically, those who were in the highest education category (having graduated high school or who had higher post-secondary education) were greater than 11 times more likely to have a good knowledge score over no knowledge, compared to those having no formal education as the referent (relative risk ratio (RRR) 11.1, 95% confidence interval (CI) 4.4, 27.6). A gradual increase in RRRs for having a good knowledge score was seen with each increasing category of education – primary (grades 1–8), secondary (grades 9–11), and high-school graduate or post-secondary (grades ≥12), respectively (RRR=3.2, 8.4, 11.1); however, this increasing trend was not seen for having a moderate knowledge score (RRRs= 1.8, 3.2, 1.3). Having a good knowledge score was also positively associated with frequency of healthcare usage, meaning those with less frequent healthcare visits had a lower relative risk of having a good knowledge score. Rurality was negatively associated with any knowledge of diabetes, indicating that those participants living in more rural locations had lower awareness and knowledge of diabetes.
Table 1: Descriptive characteristics of a sample of individuals in rural Tamil Nadu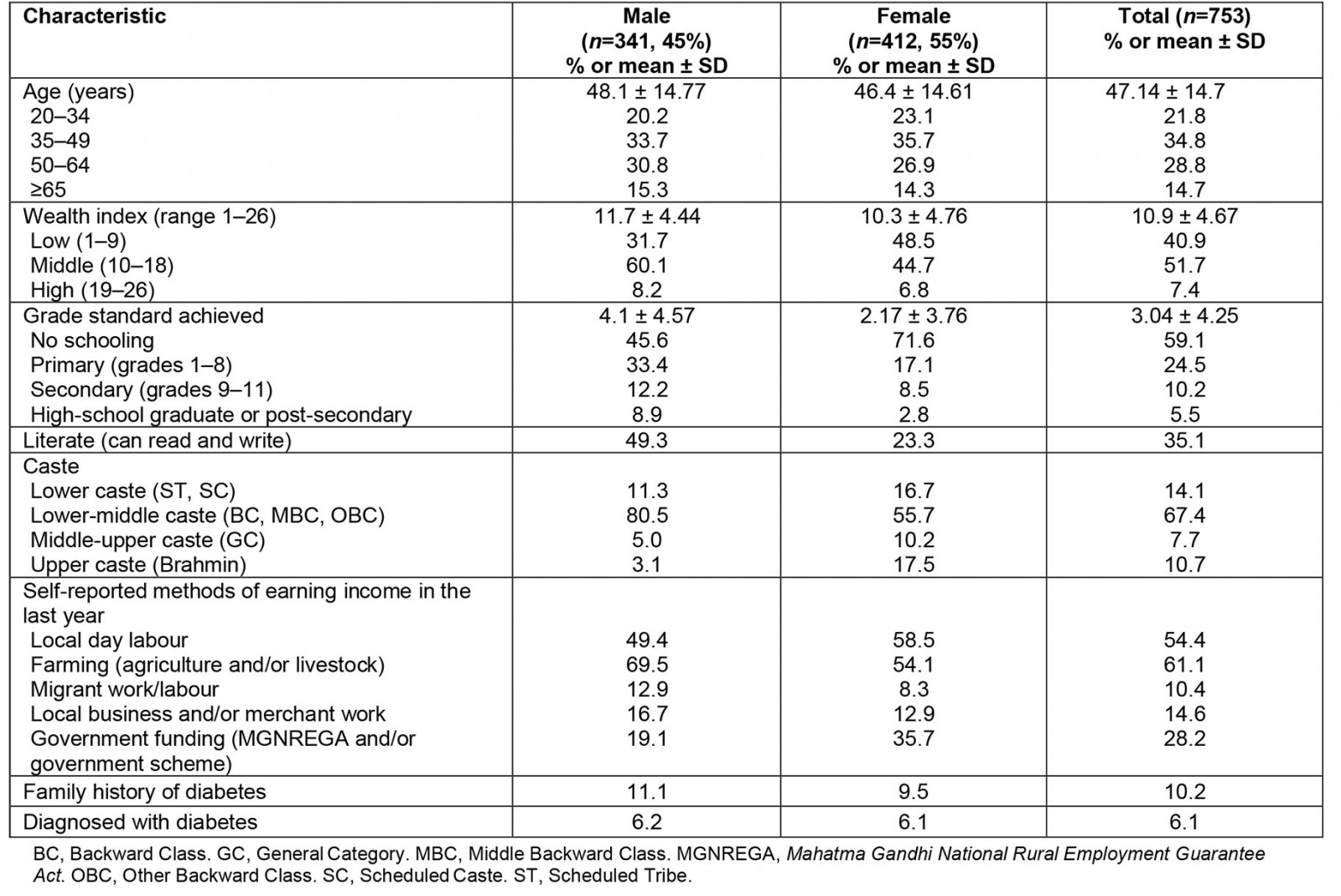
Table 2: Questions correctly answered by a rural Tamil Nadu population from a diabetes knowledge survey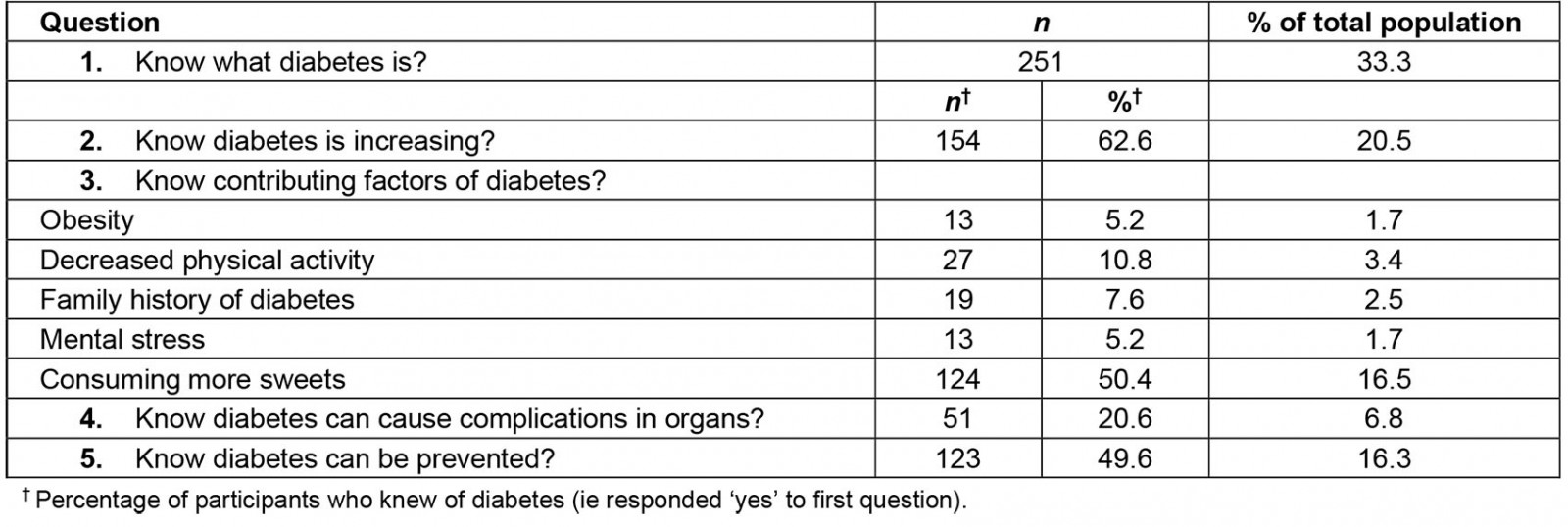
Table 3: Associations of sociodemographic factors in the final multinomial logistic regression model on diabetes knowledge score in a rural Tamil Nadu population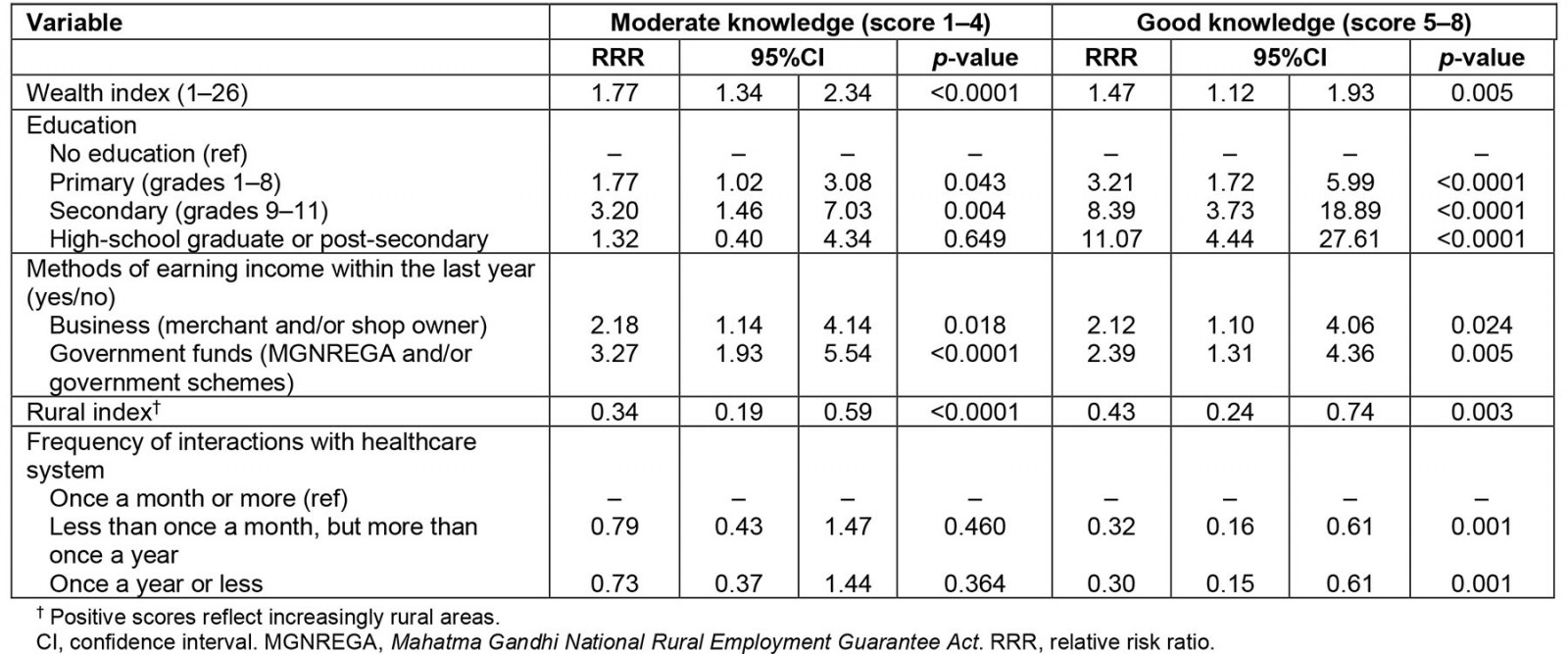
Discussion
This cross-sectional survey of adults residing in rural areas of Tamil Nadu showed poor knowledge of diabetes among the population. All participants – even subgroups with higher wealth and education – demonstrated a lack of knowledge of diabetes. Among those in the highest education category, over 40% had a knowledge score of zero, meaning they answered ‘no’ to the question, ‘Do you know what diabetes is?’. Such results indicate that, even among the most educated individuals in the study population, general knowledge of diabetes was low. Although these findings are consistent with other studies12,14,17,24,29,30, this rural region of Tamil Nadu demonstrated one of the lowest levels of knowledge in India reported to date, with 66% of participants being unaware of diabetes altogether. A study conducted by Shrivastava et al (2015) in another region of rural Tamil Nadu assessed knowledge and self-care practices among patients with diabetes and showed that, even among those with diabetes, knowledge of the disease was poor. Indeed, the study found that 49% of participants with diagnosed diabetes believed that diabetes was curable16. A similar qualitative study looking deeper into themes regarding diabetes knowledge among individuals with diabetes, showed that 96% of participants answered, ‘I don’t know’ when asked, ‘what happens inside your body when you get sick with diabetes?’31. The low awareness of diabetes shown in these studies corresponds with the present study’s findings and should be considered a serious public health concern in rural regions of South India.
Although levels of diabetes knowledge and awareness are consistently low across most studies in rural India, awareness varies across other regions in South Asia. A study conducted with adults from both urban and rural regions of Punjab, Pakistan, found that 86% of respondents had heard of diabetes32. The higher levels of education and socioeconomic status of this population could be an explanation for the heightened knowledge scores as compared to the present study. Another study conducted on a lower-middle class urban population in Chennai, the capital of the state of Tamil Nadu, showed that over 90% of the general population knew of diabetes13. Such findings suggest that diabetes awareness and knowledge may be better in urban regions, where information, messaging, and resources for diabetes may be more accessible. The association between higher wealth, education, and lower rurality and diabetes knowledge is consistent with other studies in India12,13,17, and other low- and middle-income countries, including Jordan33, Bangladesh34, Southeast Ethiopia35, Oman36, and Pakistan32.
Doctor–patient interactions in healthcare settings are important opportunities for patient education, as shown by the strong association between frequency of healthcare visits and diabetes knowledge. This finding corresponds with previous research in the study region showing that patients with diabetes perceived doctors as the most important source of knowledge on diabetes31. However, this study adds to the body of evidence suggesting that healthcare professionals in rural regions of South India do not adequately educate patients on diabetes; indeed, previous research in the study site31, and India in general37,38, found that both public and private healthcare practitioners often failed to provide even basic health education and support to patients with non-communicable diseases.
An intriguing result was the association between source of income and knowledge score. Individuals working as a merchant or shop owner were more knowledgeable about diabetes, perhaps due to increased income and socioeconomic status, allowing for more exposure and access to accurate health information when compared to farmers or labourers. Individuals of higher socioeconomic status may also be at increased risk of cardiometabolic diseases such as diabetes, perhaps increasing the likelihood that a healthcare professional might educate them on such topics, or that they access information from peers of similar social status and diabetes risk39. The nature of being a merchant and/or shop owner also creates opportunities for social interaction with community members, which may lead to discussions on health topics. Conversely, little exposure to people living with diabetes could also be a plausible explanation for the association between low diabetes knowledge and increased rurality in the present study, particularly given the lower prevalence of diabetes in rural versus urban and urbanizing settings9.
Accessing government schemes (eg MGNREGA) as a source of income was strongly associated with increased knowledge of diabetes. To the authors’ knowledge, this association has not yet been established in any previous studies. The MGNREGA scheme provides employment security for adult (over age 18 years) applicants who reside in rural households throughout all districts of India40. The main goal of the MGNREGA program is to provide employment opportunities within a radius of 5 km of a person’s home for at least 100 days in a year. Most jobs involve manual unskilled labour and pay minimum wage; however, some higher skill jobs (eg project supervisor) are available with higher compensation41. MGNREGA creates work projects for members of rural communities involving different forms of labour, sometimes including the construction of permanent assets in participating communities, such as wells, roads, and bridges40,42. While critiques of MGNREGA exist41,43-47, involvement in this program throughout rural communities has the potential to foster local economic and employment activity, improve household income security, and improve quality of life41,42,48.
While the association between diabetes knowledge and MGNREGA involvement has not been previously noted in the literature, this finding begets a number of plausible hypotheses that bear further exploration. Household income security through MGNREGA participation has been associated with increased household expenditure on education and health care41,42,49-51, possibly increasing healthcare access, and thereby exposure to diabetes knowledge. However, MGNREGA wages are often delayed and unpredictable, and may be insufficient on their own to sustain households42,43,45,47,48,50. Additionally, involvement in government programs such as MGNREGA may improve participation in other government social welfare programs, although research in this area is lacking. One study in particular found that women involved in MGNREGA had a high awareness of other existing government schemes, with some even expressing concern for over-dependency on government benefits and programs42. Engagement in several government or social welfare programs may have the potential to foster trust and improve uptake in other government services and sources of information. In the present study, it is possible that those participants involved in MGNREGA were more likely to seek and trust health information from government sources. Lastly, MGNREGA can improve community cohesion and bonding among those involved in the program42,48. Involvement in MGNREGA work may provide a platform to discuss common issues and interests, including health concerns42. Overall, the association between MGNREGA participation and diabetes knowledge is novel and possible mechanisms should be explored further.
Several studies highlight understandings and perceptions of diabetes among Indian populations that occasionally conflict with biomedical models. For example, a common perception in India is that consuming excess sugar is a primary cause of diabetes14,16,17,24,29. Additionally, ‘tension’ or mental stress are often also cited as direct causes of diabetes14,17, and herbal or religious remedies are often recognized as effective treatments for diabetes12,14. Such patterns are consistent with the present study, as the most common perceived risk factor of diabetes was consuming sweets (16.5% of the study population). Correspondingly, as described in a previous study in the same region, the local colloquial term for diabetes was translated as ‘sugar disease’31. Mental stress was also reported as a risk factor by 5% of those who knew of diabetes, the same proportion who reported obesity as a risk factor. This exemplifies how cultural and local understandings of health and disease (such as ‘tension’) may influence perceptions of diabetes causation14,31. Evidence also indicates that, for many individuals in South Asia, family and friends are a main source of information on diabetes52,53. Reliance on social networks for health information further perpetuates localized understandings of diabetes, grounded in experiences of individuals rather than information from health authorities.
The low number of individuals in this study who reported obesity as a risk factor to diabetes (1.7% of the total population) is particularly concerning, considering obesity is one of the strongest predictors of type 2 diabetes4,8-10. Such findings correspond with a similar study investigating diabetes knowledge in a rural north-eastern Indian population, which found that only 40% of those who were overweight knew they had an increased risk of diabetes15. Sociocultural constructs regarding what is ‘healthy’ and ‘unhealthy’ may perpetuate this perception; indeed, some studies suggest that overweight and obesity are perceived as ‘healthy’ in subpopulations in rural India, especially among low socioeconomic status individuals, because overweight can be a sign of wealth and food security52.
The fragmented healthcare system in India, along with poor investments in public health initiatives and health education, limit access to reputable and relevant information regarding health and disease, especially for rural populations. Many studies highlight the difficulty of receiving care for simple health issues, often citing the unavailability of doctors, long wait times, high costs, and lack of healthcare coordination54,55. Despite the greater expense, private health care is often perceived as superior to public health care for major health problems such as diabetes55. Regardless, both public and private healthcare facilities often face resource constraints that limit their ability to disseminate information regarding diabetes. Further, poverty and social inequities act as barriers to accessing health care in rural India. Healthcare centres are often located in urban cities (thus requiring transportation), are focused on tertiary care, and only affordable to the urban affluent, with rural poor individuals being faced with limited healthcare options56. Many individuals in rural areas face financial hardships and use their income to sustain daily living, often avoiding healthcare services unless for life-threatening conditions54.
India is currently grappling with an epidemiological transition that is driving an increasing burden of non-communicable diseases such as diabetes2. So far, diabetes prevention efforts have been woefully unsatisfactory in India, especially in rural areas56,57. It is therefore crucial and timely to improve efforts and allocate resources to alleviate the burden of diabetes. The associations of sociodemographic factors with diabetes knowledge in this study highlight priority areas for targeting initial public health efforts in Tamil Nadu. Specifically, efforts should emphasize the dissemination of accurate knowledge of diabetes signs, symptoms, prevention, and treatment to rural and isolated regions where populations lack access to formal education and seldomly interact with healthcare systems. Importantly, improved knowledge on diabetes has been associated with positive attitudes and better self-care practices towards diabetes treatment and prevention16,33,35,36. Thus, investing in stronger public health efforts to improve healthcare access, quality, and focusing on non-communicable disease prevention and treatment, presents a crucial tool for lessening the severity and impacts of the diabetes epidemic in India. Additionally, structural factors grounded in economic and political realities – for example, food environments, access to sustainable livelihoods, and availability of recreational opportunities – are also crucial components to preventing and managing non-communicable diseases, and must be incorporated into any regional or national strategy to prevent burdens of diabetes58,59.
Strengths of this study include the use of systematic random sampling to reduce sampling bias, the use of validated tools to measure socioeconomic status and diabetes knowledge to reduce the risk of misclassification bias, and the use of a statistical modelling technique that accounted for confounding bias and incorporated a polytomous outcome. This study also examined rurality on a continuous scale instead of a binary urban–rural divide, allowing for increased granularity in examining the relationship between rurality and diabetes knowledge. This study also had some limitations. Importantly, cross-sectional surveys are unable to establish causation. Because most sociodemographic data and knowledge on diabetes was self-reported, some data may have been be influenced by misreporting or social desirability bias. Finally, weaknesses of the diabetes knowledge questionnaire have been well documented24, and include open-ended questions being inhibited by memory and recall bias, and closed-ended questions possibly encouraging respondents to provide guesses instead of informed answers.
Conclusion
The present study contributes to the large body of research regarding diabetes knowledge in India and South Asia. Specifically, this study sought to investigate the overall knowledge of diabetes in a rural population, as well as to examine the influence of different sociodemographic factors on knowledge of diabetes. Overall, this study highlighted the low levels of knowledge regarding diabetes in this rural population in Tamil Nadu. Positive associations were identified between knowledge score and wealth, education, MGNREGA and business ownership as sources of income, as well as frequency of health care received. Increasing rurality was negatively associated with knowledge score. Given the high prevalence of diabetes as well as prediabetes in this specific rural population9, as well as in the Tamil Nadu state in general7, this lack of general knowledge presents a major public health concern. Findings on the sociodemographic factors associated with knowledge of diabetes underscore the need for targeted education programming that aims to improve health literacy and diabetes awareness among those of lower socioeconomic status who lack formal education and reside in isolated and rural regions.
References
You might also be interested in:
2015 - 2014 Rural Clinical School Training and Support Program Snapshot survey