
Introduction
Infectious diseases threaten not only human health, but also social and economic wellbeing in a variety of ways1. As such, solid and sensitive infectious disease surveillance systems need to be developed and implemented to prevent and control epidemics2. In many countries, designated target infectious diseases must be reported to national infectious disease surveillance systems3-5.
In Japan, the National Epidemiological Surveillance of Infectious Diseases Program is conducted as a type of statutory national infectious disease surveillance system under Articles 12–16 of the Act on the Prevention of Infectious Diseases and Medical Care for Patients with Infectious Diseases since April 1999. This surveillance system mainly consists of pathogen and patient reporting. Legally targeted infectious diseases are reported to population-based or sentinel surveillance systems. Population-based surveillance systems require all medical institutions to report all cases of the target infectious diseases, whereas sentinel surveillance systems require medical institutions designated as sentinel reporting sites to report cases of target infectious diseases weekly or monthly. All reports are analyzed, interpreted, and published weekly or monthly by national and prefecture-level infectious disease surveillance centers and local public health centers6,7.
Although efforts are made to generate and share information regularly, frequently, and in a timely manner in statutory national infectious diseases surveillance systems4,8, previous reports have pointed out their limitations, which include underreporting, a lack of timeliness, a lack of representativeness, and, in particular, the low sensitivity of sentinel surveillance systems9-11. Large-scale sentinel surveillance systems cannot identify all local outbreaks that occur in small communities10. To overcome these limitations of statutory national infectious disease surveillance systems, the development of local community-based systems is needed12,13. Local community-based infectious disease surveillance systems may improve the early detection of diseases and assessment of outbreaks because they are close to small local communities, which are typically the first to know about unusual happenings12,13. Moreover, the complementary presence of surveillance systems at large-scale national and small-scale local community levels may increase the sensitivity of the overall surveillance of infectious diseases13,14. Local community-based surveillance systems suited to the characteristics of each community need to be developed, especially in remote and rural areas, which are low-resource settings; therefore, it is necessary to devise systems that meet local community needs and can deal with constrained resources13,15.
Isa city is a remote rural area located inland in the northernmost part of Kagoshima Prefecture, Japan. Isa city is one of the cities that compound the Aira-Isa Secondary Medical Care Area, a medical administrative area based on the Medical Care Act 1948, a regional unit that provides medical admission (Fig1). The population of Isa city is about 24 000, and the proportion of the older population (≥65 years) is 41.6% (2020). Isa city’s primary industries are agriculture and healthcare services. The city also has six hospitals and 15 clinics, including two ophthalmology clinics. The entire Aira-Isa Secondary Medical Care Area is under the jurisdiction of the Aira Public Health Center, with one branch of the Okuchi Public Health Center in Isa city.
In the Aira-Isa Secondary Medical Care Area, both population-based and sentinel surveillance are reported to the Aira Public Health Center from medical institutions that serve as reporting sites through statutory survey forms sent by fax or postal mail. Then, the Aira Public Health Center registers the survey data in a national online database. Medical institutions in Isa city follow the same survey process. After registration, the Aira Public Health Center publishes weekly reports on the number of cases of infectious diseases subject to sentinel surveillance separately under the jurisdiction area of the Aira Public Health Center and the Okuchi Public Health Center. The surveillance period is from Monday to Sunday, and the aggregated weekly reports are published on Thursday or Friday of the following week. It takes 4–5 days from the surveillance data collection to data reporting by the statutory infectious disease surveillance systems in the entire Aira-Isa Secondary Medical Care Area. In its weekly reports, the number of cases of all legally targeted infectious diseases by sentinel surveillance (influenza, infectious diseases to be reported by pediatric sentinel sites, infectious diseases to be reported by designated core sentinel sites), except for sexually transmitted diseases, are reported separately under the Aira Public Health Center and the Okuchi Public Health Center, because there are reporting sites in both areas. However, only the number of cases of the legally target infectious eye diseases (acute hemorrhagic conjunctivitis and epidemic keratoconjunctivitis) under the Okuchi Public Health Center are not reported. Only the number of cases under the Aira Public Health Center are reported in weekly reports. The reason for this is that although Isa city has all other sentinel surveillance systems of target infectious diseases, in which the number of cases is published in weekly reports, it does not have a statutory ophthalmology sentinel surveillance system under the jurisdiction of the Okuchi Public Health Center. The nearest medical institution that serves as an ophthalmology sentinel reporting site is in the neighboring Kirishima city; this medical institution is the only sentinel reporting site serving as a statutory ophthalmology sentinel surveillance system for the entire Aira-Isa Secondary Medical Care Area.
In January 2016, a physician, hospital administrator, and certificated infection control doctor at hospital A (82 beds), a community-based medium-sized hospital in Isa city, heard from a community resident that an eye disease was prevalent in the city. Upon inquiring with ophthalmologists in Isa city, they discovered that the number of patients with epidemic keratoconjunctivitis was increasing. However, this increasing trend in Isa city was not indicated by the statutory ophthalmology sentinel surveillance system for the entire Aira-Isa Secondary Medical Care Area. As mentioned above, this incident made clear how large-scale statutory sentinel surveillance systems cannot capture all local outbreaks that occur in small communities10. Therefore, a decision was made to develop a voluntary and unique local community-based ophthalmology sentinel surveillance system in Isa city (OSSS-Isa), with hospital A taking the leading role.
Several local community-based infectious disease surveillance systems have been reported in Japan, including a real-time infectious disease surveillance system in Gifu Prefecture, a pediatric infectious disease surveillance system in Shizuoka Prefecture, and an infectious disease surveillance system in Kawasaki city16-18. These surveillance systems were developed in response to the needs of their respective communities; likewise, OSSS-Isa. A major feature of these initiatives is that the leading roles are played by public administrations, prefectural-level medical associations, or large hospitals that assume a core medical role in the region. In addition, these surveillance systems use advanced information and communications technology (ICT). In a voluntary influenza surveillance system in Iki city, Nagasaki Prefecture, a remote and rural community with characteristics similar to those of Isa city, the leading roles are also played by the local medical association and public health center19. Regarding OSSS-Isa, the leading role is played by a physician in a community-based medium-sized hospital. Moreover, a notable objective of OSSS-Isa is to devise a small-scale infectious disease surveillance system that meets the needs and characteristics of the community while complementing the statutory surveillance systems, in this case, a remote and rural aging area with few resources and actors. Thereby, the findings of the present study could make practical contributions to the further development and implementation of local community-based infectious diseases surveillance systems led by community-rooted physicians in remote and rural areas in a feasible way appropriate to the characteristics of local communities.
Given this background, this study aimed to develop, implement, and evaluate OSSS-Isa, a voluntary and unique local community-based infectious disease surveillance system.
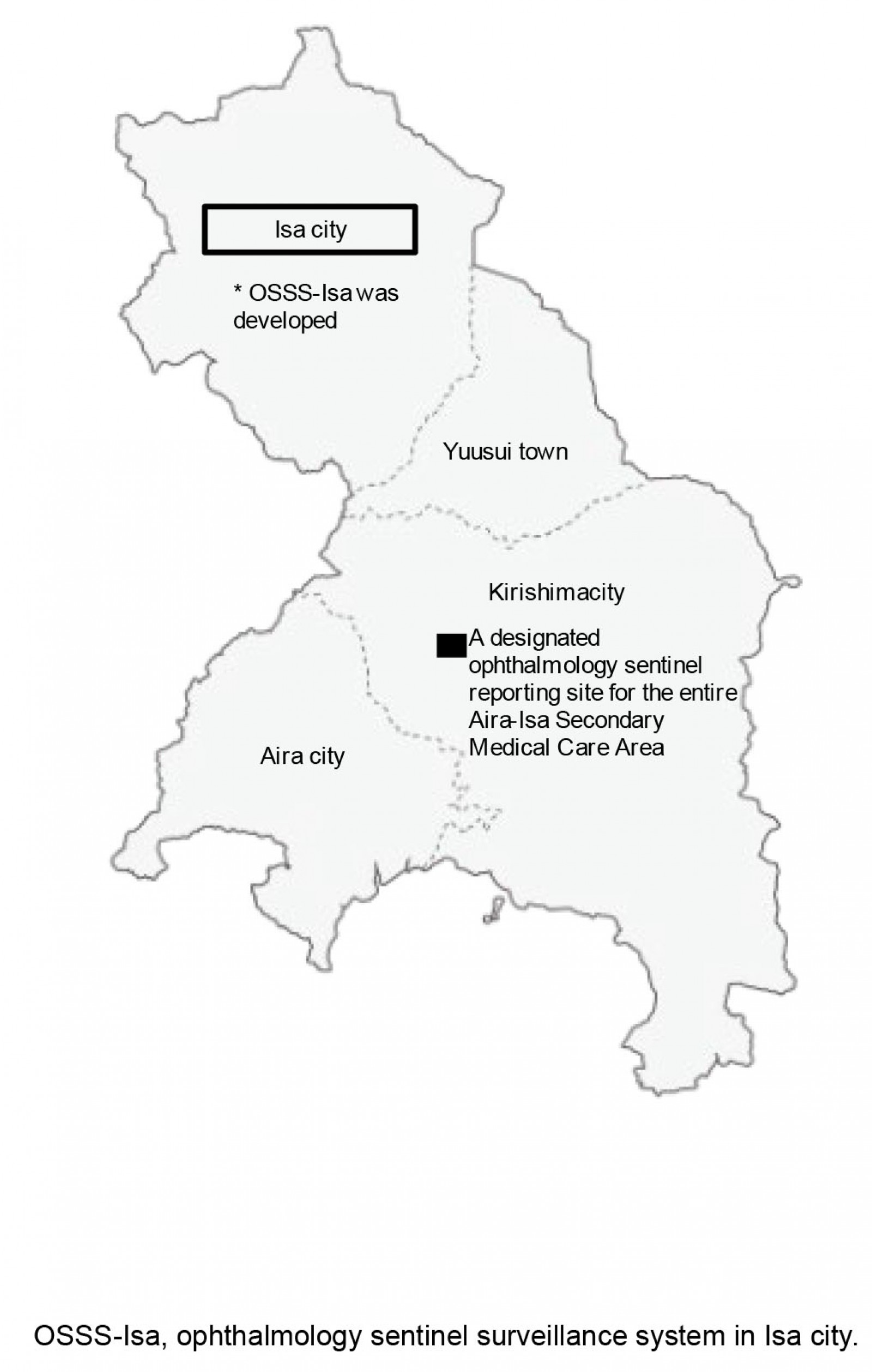 Figure 1: The entire Aira-Isa Secondary Medical Care Area and location of Isa city.
Figure 1: The entire Aira-Isa Secondary Medical Care Area and location of Isa city.
Methods
Development of OSSS-Isa
First, in January 2016, a physician, hospital administrator, and certificated infection control doctor at hospital A in Isa city enlisted the cooperation of two ophthalmology clinics as ophthalmology sentinel reporting sites. Estimated from the administrative data on ‘the rates of estimated ophthalmic outpatients per 100 000 population (per day) for Kagoshima Prefecture in 2017’, which were 23520, 61 outpatients visited the two ophthalmology clinics in Isa city daily in that year (235 × 25 813 persons (the population of Isa city in 2017)/100 000 persons). Thereby, it was estimated that in 2016, a total of about 60 outpatients visited the two ophthalmology clinics in Isa city daily. Then, the physician at hospital A developed a network with 20 hospitals and clinics in Isa city as actors to obtain surveillance data from hospital A while explaining the community needs and significance of OSSS-Isa (Fig2). Acute hemorrhagic conjunctivitis and epidemic keratoconjunctivitis were targeted to be reported in OSSS-Isa in accordance with the legally targeted infectious eye diseases in the statutory ophthalmology sentinel surveillance system. One of the significant roles of OSSS-Isa is to complement statutory ophthalmology sentinel surveillance systems on a small, local community level; hence, the rationale is to set the reporting target eye disease in OSSS-Isa according to the legally targeted infectious eye disease.
Surveillance was conducted on a weekly basis from Monday to Sunday. The two ophthalmology clinics, which served as sentinel reporting sites for OSSS-Isa, reported weekly cases of acute hemorrhagic conjunctivitis and epidemic keratoconjunctivitis, using a paper-based survey form (Fig3), and sent them to hospital A by fax every Monday. Then, hospital A aggregated the numbers of patients with the two targeted infectious eye diseases by sex and age group on the same day, compiled the surveillance data into a paper-based report form with the same design as the survey form (Fig3), and promptly sent it by fax to 20 hospitals and clinics in Isa city simultaneously on the same day (ie Monday). Compared with weekly reports published by the Aira Public Health Center and distributed to the entire Aira-Isa Secondary Medical Care Area on Thursday or Friday of the following week, the surveillance data collection, aggregation, and information reporting by OSSS-Isa was 4–5 days faster than that of existing statutory infectious disease surveillance systems.
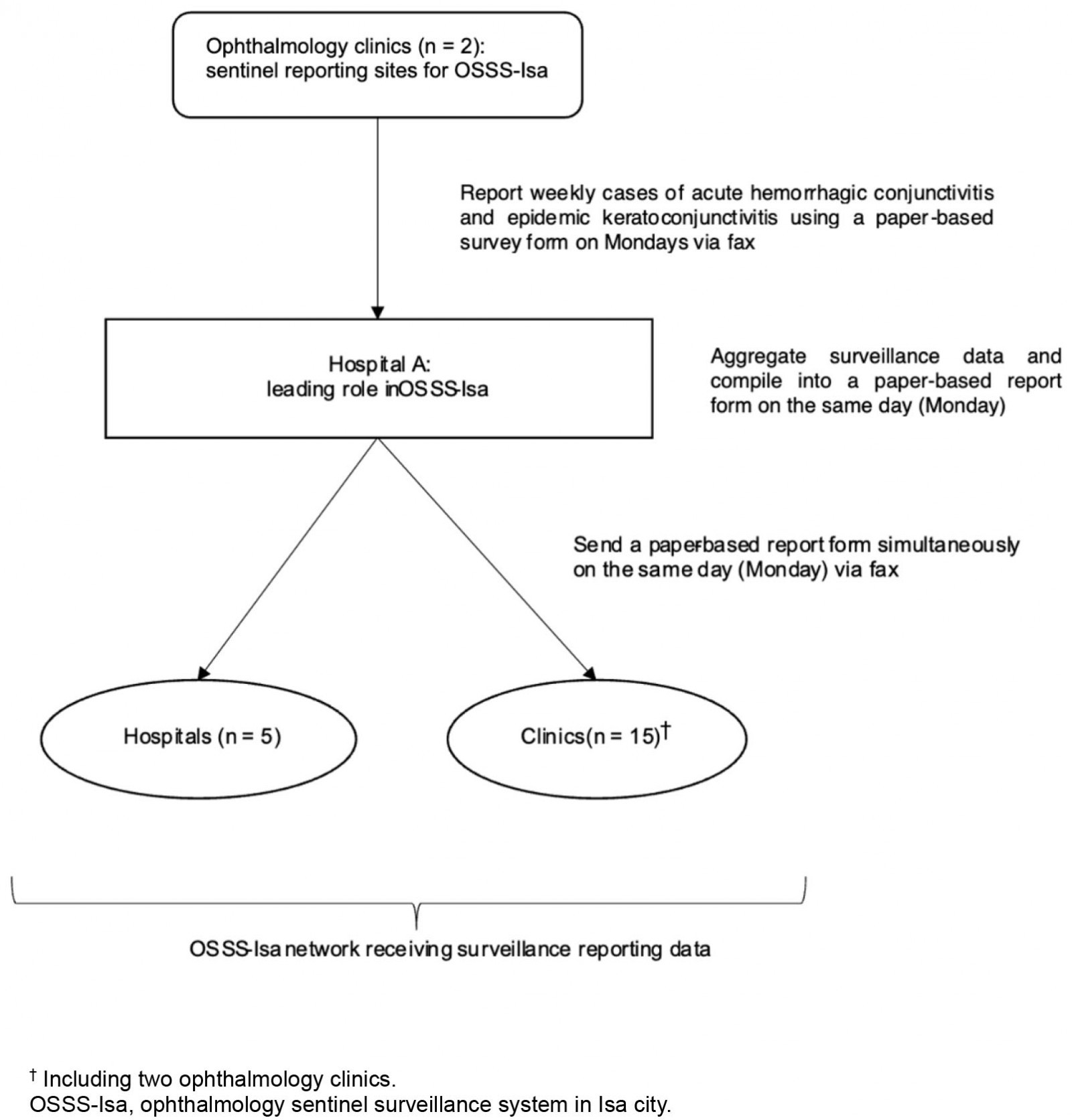 Figure 2: Local community-based ophthalmology sentinel surveillance system in Isa city.
Figure 2: Local community-based ophthalmology sentinel surveillance system in Isa city.
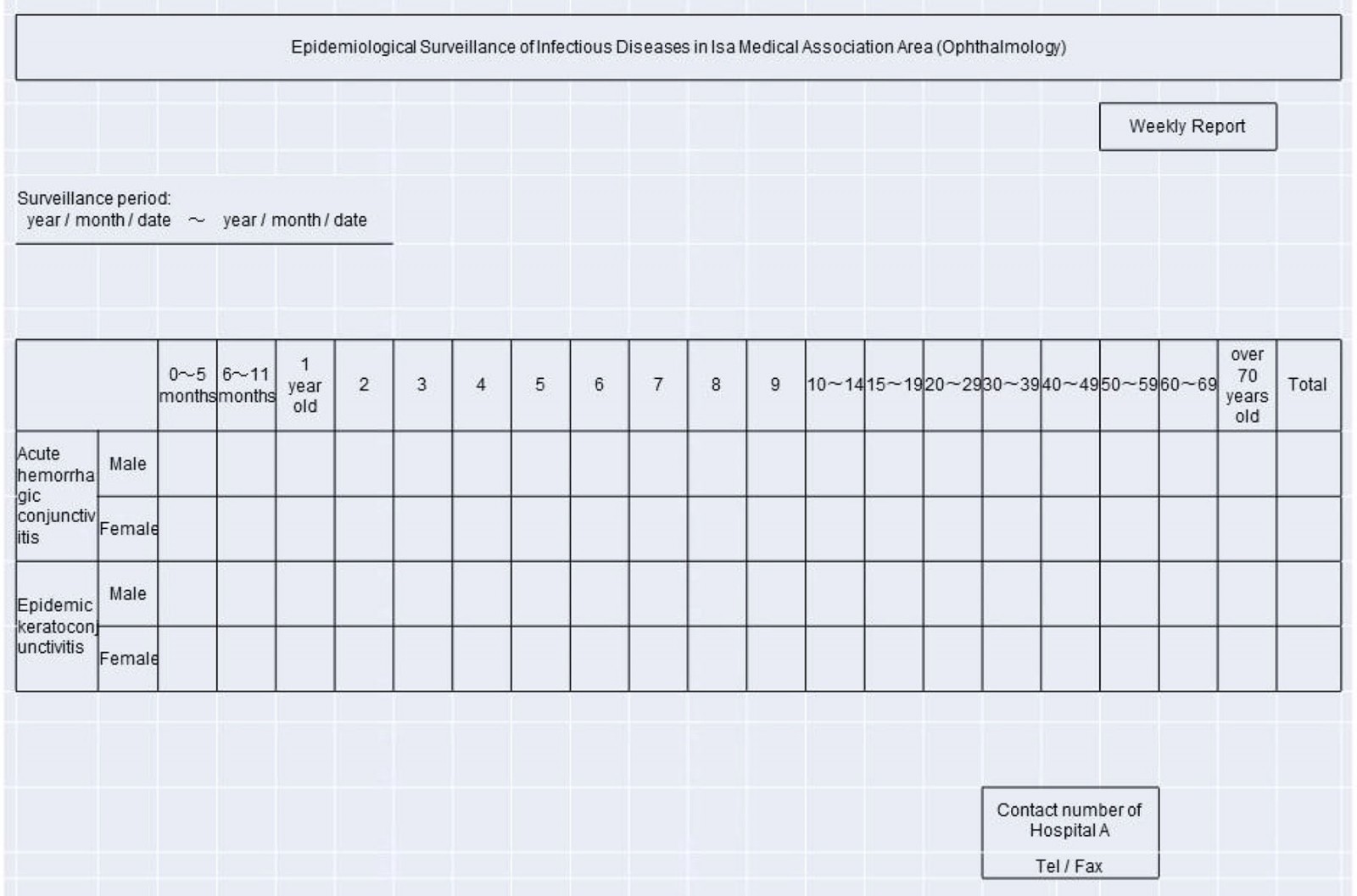 Figure 3: Paper-based survey and report form used in ophthalmology sentinel surveillance system in Isa city.
Figure 3: Paper-based survey and report form used in ophthalmology sentinel surveillance system in Isa city.
Evaluation of OSSS-Isa
A questionnaire survey was conducted to evaluate the utility of OSSS-Isa. The survey followed the updated guidelines for evaluating public health surveillance systems proposed by the Centers for Disease Control and Prevention21 for selecting evaluation criteria for infectious disease surveillance systems and developing a questionnaire. The criteria selected for the questionnaire survey were simplicity, flexibility, data quality, acceptability, timeliness, and stability. The face and content validity of the questionnaire were reviewed by an expert committee composed of researchers, and their views were applied in minor revisions. The responses were evaluated on a five-point Likert scale from 1 to 5. A more positive response regarding each evaluation criterion was indicated by a higher score. Each question item and corresponding Likert scale are shown in Table 1. The questionnaires were distributed to all medical institutions in Isa city (five hospitals and 15 clinics), except hospital A. The questionnaires were distributed and collected by postal mail.
Data analysis
All data were analyzed using Microsoft Excel 2021 (Microsoft Corporation, http://www.microsoft.com) to calculate absolute and relative frequencies and mean scores.
Ethics approval
This study was approved by the Ethics Committee on Epidemiological Studies, Kagoshima University (approval no. 220148Eki).
Results
Implementation of OSSS-Isa
The implementation of OSSS-Isa started in February 2016. From February 2016 to September 2018, surveillance for epidemic keratoconjunctivitis and acute hemorrhagic conjunctivitis remained at 0 or 1 case each week. However, in the first week of October 2018, three cases of epidemic keratoconjunctivitis were reported in men and women as a trigger, and a total of six cases of epidemic keratoconjunctivitis arose over a wide age range (0 to >70 years) during the second and third weeks of the same month (Fig4). Infected patients were reported from both ophthalmology clinics serving as sentinel reporting sites for OSSS-Isa. This unusual happening suggested that a local outbreak of epidemic keratoconjunctivitis was occurring in Isa city. However, at the same time, the statutory ophthalmology sentinel surveillance system for the entire Aira-Isa Secondary Medical Care Area continued to show 0 or 1 case of epidemic keratoconjunctivitis during that same period of October 2018, which did not reflect the unusual happening indicating a possible sign of an infectious eye disease outbreak in Isa city (Fig4). During the second and third weeks of October 2018, hospital A twice issued the following alert regarding an outbreak of epidemic keratoconjunctivitis to the 20 hospitals and clinics in the OSSS-Isa network, using the weekly report form: ‘The number of cases of epidemic keratoconjunctivitis is increasing. Please take standard precautions, such as handwashing’. During the fourth week in October 2018, the number of cases of epidemic keratoconjunctivitis in Isa city decreased to 1, and by the fifth week, no cases of epidemic keratoconjunctivitis remained in the local area.
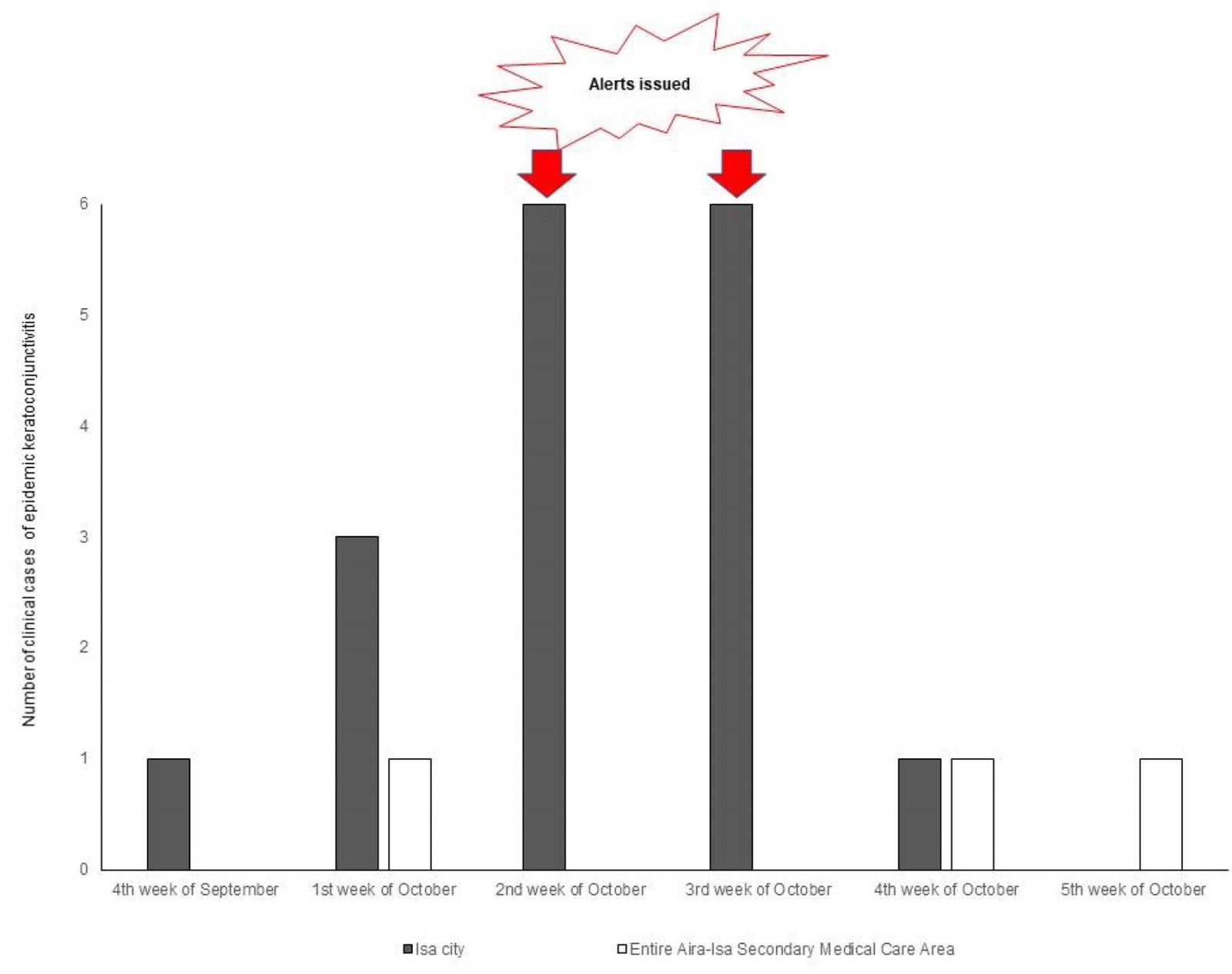 Figure 4: The number of clinical cases of epidemic keratoconjunctivitis in Isa city and the entire Aira-Isa Secondary Medical Care Area from the fourth week of September to the fifth week of October 2018.
Figure 4: The number of clinical cases of epidemic keratoconjunctivitis in Isa city and the entire Aira-Isa Secondary Medical Care Area from the fourth week of September to the fifth week of October 2018.
Evaluation of OSSS-Isa
We received questionnaire surveys from 18 hospitals and clinics (response rate 90%). All respondents were physicians who were either hospital or clinic administrators. The results of the questionnaire survey are shown in Table 1.
For the first question regarding simplicity, which was asked only to the two ophthalmology clinics serving as sentinel reporting sites for OSSS-Isa, both clinics responded that filling out the OSSS-Isa survey form was ‘simple’. For the second question regarding simplicity, the majority of respondents (14/18, 77.8%) felt that it was ‘very simple’ or ‘simple’ to understand the sequence of data collection, aggregation, and reporting for OSSS-Isa. For the third question regarding simplicity, the majority of respondents (15/18, 83.3%) felt that it was ‘very simple’ or ‘simple’ to understand the results of the OSSS-Isa weekly data report.
Regarding flexibility, 61.2% (11/18) of respondents felt that OSSS-Isa was ‘very flexible’ or ‘flexible’ in accommodating changes in the system, such as adding collaborating institutions or target diseases to be monitored. Regarding data quality, which was asked only to the two ophthalmology clinics, both clinics answered that they ‘rarely’ answered with incomplete/unknown responses in the survey form when infectious cases were occurring. Regarding acceptability, the majority of respondents (15/18, 83.4%) were ‘clearly aware’ or ‘aware’ of the objective of OSSS-Isa to ‘detect infectious eye disease outbreaks in Isa city in a timely and accurate manner’.
For the first question regarding timeliness, the majority of the respondents (15/18, 83.4%) answered that OSSS-Isa was operated in a ‘very timely’ or ‘timely’ manner, from case occurrence to data collection, aggregation, and reporting. For the second question regarding timeliness, the majority of respondents (14/18, 77.8%) felt that alerts about regional increases in eye infections and the need for standard precautions, which had been sent out twice to the OSSS-Isa network, were ‘very timely’ or ‘timely’ for their immediate action in clinical practice.
Regarding stability, the majority of respondents (15/18, 83.4%) felt that OSSS-Isa was ‘very stable’ or ‘stable’ for collecting, aggregating, and reporting the surveillance data.
The mean scores for each question regarding simplicity, data quality, acceptability, timeliness, and stability were all higher than 3.67. The mean score for flexibility was only slightly lower, at 3.61.
Table 1: Questionnaire items and results of the survey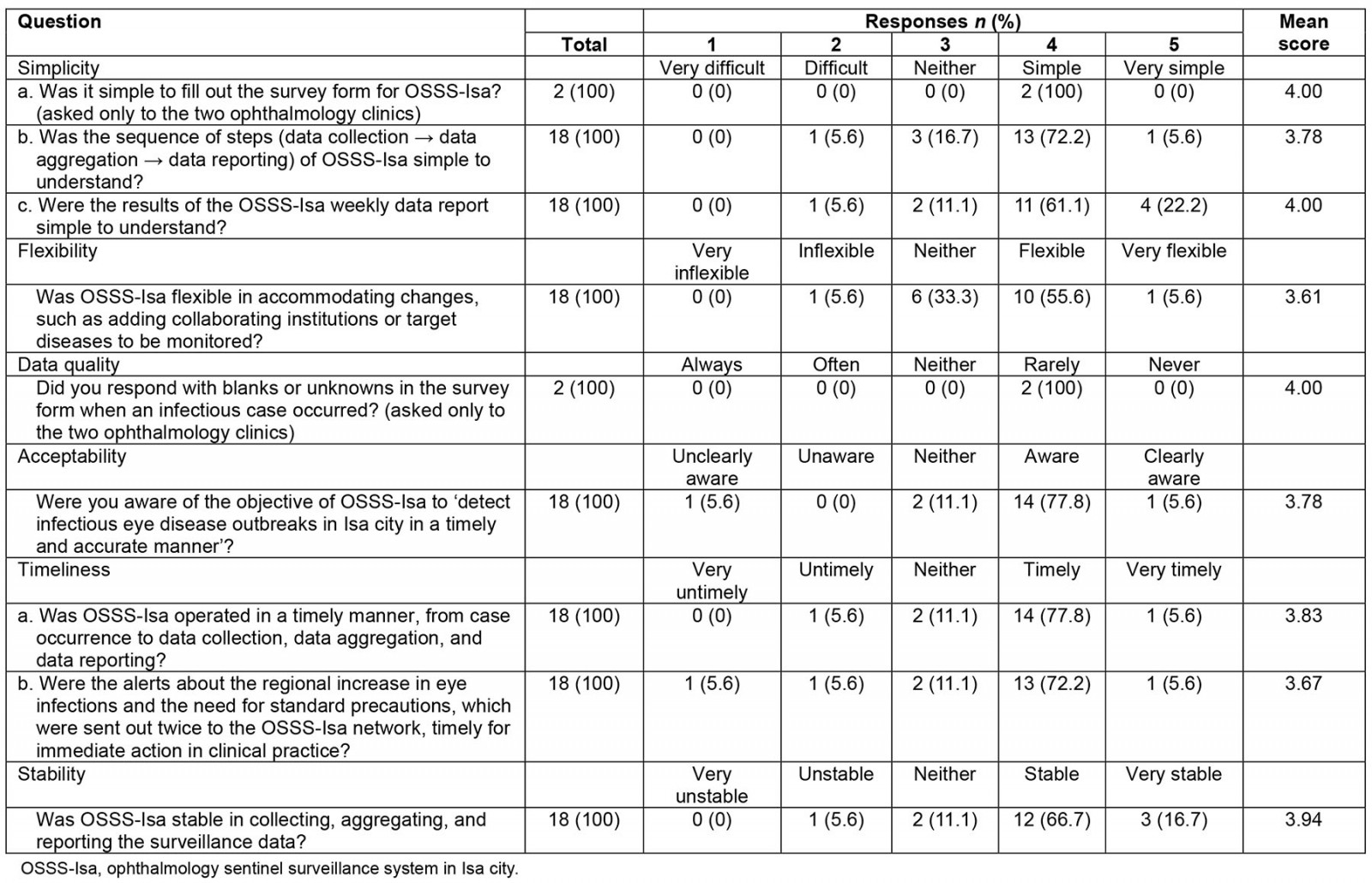
Discussion
In this study, an ophthalmology sentinel surveillance system in a small remote rural local community, OSSS-Isa, was developed, implemented, and evaluated. The results indicated that OSSS-Isa has high simplicity, data quality, acceptability, timeliness, and stability for local healthcare providers in Isa city. OSSS-Isa can quickly detect signs of infectious eye disease outbreaks emerging in small local communities, where unusual happenings often occur first, leading to fast and accurate alerts to surveillance system networks. The present study proposes a unique small-scale, local, community-based infectious disease surveillance system that helps overcome the limitations of large-scale statutory national infectious disease surveillance systems in remote rural communities.
In Japan, approximately 700 ophthalmologic medical facilities are designated as the statutory ophthalmology sentinel reporting sites. However, no ophthalmology sentinel reporting sites are designated for areas in the jurisdiction of a public health center with a population of less than 125 000, and only 1 + (population – 125 000 persons)/150 000 persons for areas in the jurisdiction of a public health center with a population of more than 125 0006. As efforts are made to be consistently representative, sentinel reporting sites are selected as randomly as possible, and the number of sentinel reporting sites per public health center is considered to cover areas as much as possible6. However, limitations in regard to the sensitivity and representativeness to outbreaks in large-scale statutory national sentinel surveillance systems have been noted not only in the previous literature9-11, but also as the catalyst of the OSSS-Isa initiative. The present study found that sometimes signs of an outbreak in a small local community cannot be captured accurately by large-scale statutory national sentinel surveillance systems. Our findings suggest that if small-scale, voluntary, local community-based infectious disease surveillance systems can complement the large-scale ones, the sensitivity of overall surveillance may be improved. This suggestion is in line with a previous study reporting that several types of complementary surveillance systems need to exist to capture outbreaks in various areas in resource-constrained settings14,15. In remote rural areas, where resources are necessarily limited, collaboration among actors in the community and existing resources is essential to implement scalable surveillance systems. Regarding OSSS-Isa, the local public health center requested to share the surveillance data from OSSS-Isa. The further possibility of complementary working is opening up between large-scale statutory surveillance systems and small-scale voluntary OSSS-Isa with collaboration among existing actors and resources in this small remote rural community.
OSSS-Isa was highly evaluated by local healthcare providers in Isa city. The high simplicity of OSSS-Isa seems to have been achieved by using a simple paper-based survey and report form for data collection, aggregation, and reporting. Also, regarding data quality, cases were rarely reported as blank or unknown on the simplified paper-based form. Moreover, the method for collecting and reporting the surveillance data was based on a fax-based system as opposed to advanced ICT, which seems to have been better suited to the characteristics of the aging population and limited resources in Isa city. Physicians in rural areas of Japan are older than those in urban areas22, so using advanced ICT in remote and rural areas involves limitations in both cost and access23. The trend towards the development of advanced ICT technology for large-scale surveillance systems is essential. However, the results of the present study also suggest that well-designed simplicity using easy methods is also important to establish small-scale infectious disease surveillance systems rooted in remote rural low-resource communities. To accumulate knowledge about both high-tech and simple methods, it may help to develop various complementary infectious disease surveillance systems to cover areas of different sizes.
In the present study, the timeliness and stability of OSSS-Isa were also highly evaluated by local healthcare providers in Isa city. In contrast, in a previous study conducted in a low-resource setting in a developing country, external factors such as facilities and technical problems had a negative impact on timeliness and stability15. From this comparison, such external factors seemed to be working safely in Isa city, even though it is a resource-constrained remote rural area. These findings suggest that ensuring a good state of external factors, such as the state of facilities and communication technologies, is important for operating accurate infectious disease surveillance systems in remote rural areas. Moreover, timeliness and stability are affected by human factors such as the reliance on the person in charge of the surveillance systems and perceptions of the importance of the surveillance tasks15. Regarding the OSSS-Isa network development process, the hospital A physician who assumed leadership of the initiative explained the community needs and significance of OSSS-Isa to local healthcare providers in Isa city. This effort is highly accepted by the network members, which was indicated by the result of acceptability that the awareness of the objective of OSSS-Isa was highly evaluated. It seems that the objective of the surveillance system was well shared across the network and may promote the responsibility of those involved with OSSS-Isa. The primary reason for this success seems to be that the hospital A physician who had assumed leadership was a certificated infection control doctor who had adequate knowledge of infectious diseases. In addition, this physician had been dedicated to providing healthcare services in Isa city for over 30 years; hence, the physician’s knowledge and experience as a leader was sufficient to treat infectious diseases through the systems developed in the small remote rural local community.
The high simplicity, data quality, acceptability, timeliness, and stability of OSSS-Isa, a small-scale, local, community-based infectious disease surveillance system, was supported by well-designed implementation methods, good external factors, and active human factors, and gained trust from local healthcare providers. The double alerts OSSS-Isa provided to the network were immediately utilized at a high rate in clinical practice. The reason for this seems to be that the system developed sufficient trust among the actors. Flexibility could have been rated higher if additional diseases and institutions had been actually added. However, with a rating of more than 60%, the local healthcare providers felt that the flexibility of OSSS-Isa still had some degree of assurance.
Limitations and further implications
This study had several limitations. First, the causal relationship between the OSSS-Isa initiative and the decrease in epidemic keratoconjunctivitis in Isa city cannot be stated statistically. However, we found that the double alerts from OSSS-Isa were immediately utilized by the local healthcare providers in clinical practice at a high rate. The high simplicity, data quality, acceptability, timeliness, and stability of OSSS-Isa seems to have gained trust from local healthcare providers, and thus, OSSS-Isa may contribute to the earlier and more accurate detection of signs of infectious disease outbreaks emerging in small, remote, rural local communities. Second, as the findings in the present study are based on a single case with no controls, and no comparisons were conducted, it is difficult to conclude unequivocally that OSSS-Isa is clearly effective for infection prevention and control. Moreover, the external validity is also limited. Further qualitative study with interviews is needed to assess whether the local healthcare providers in Isa city perceive OSSS-Isa as an effective surveillance system for infection prevention and control by asking about their recognition. However, the present findings suggest that OSSS-Isa has high utility for local healthcare providers in Isa city. The success factors that support the high utility of OSSS-Isa as a unique model of a small-scale local community-based infectious disease surveillance system in a remote rural community were carefully considered. As such, our findings may contribute to the further practical development and implementation of small-scale local community-based infectious disease surveillance systems in a feasible way appropriate to the characteristics of remote and rural communities. However, the present study identified only facilitators for developing and implementing a small-scale local community-based infectious disease surveillance system in a remote and rural area; further research is needed to identify inhibitors.
OSSS-Isa is currently limited to ophthalmology surveillance, but it has the potential to expand to become a community-rooted and scalable infectious disease surveillance system for additional target diseases, or to develop as a network with other actors in local communities, such as schools and welfare facilities. The OSSS-Isa initiative is also a meaningful practical example of health advocacy in which local healthcare providers get involved with a broader range of community actors to develop systems at the community level, going beyond the boundaries of routine medical practice. If complementary statutory large-scale and voluntary small-scale surveillance systems exist and work together locally, nationally, and internationally, it might be possible to improve the sensitivity of overall surveillance and detect small, unusual happenings in small local communities, such as emerging infectious diseases, and thereby help avert global outbreaks.
Conclusion
The present results indicate that OSSS-Isa has high simplicity, data quality, acceptability, timeliness, and stability, which is highly embedded with local healthcare providers in Isa city. OSSS-Isa contributed to the early and accurate detection of signs of an infectious eye disease outbreak emerging in the small, remote, rural local community. The success factors seem to include the well-designed implementation methods, good external factors, and active human factors suited to the characteristics of a small, remote, rural community. The OSSS-Isa initiative is also a meaningful practical example of health advocacy by healthcare providers to develop a system at the local social level while going beyond the boundaries of routine medical practice. If voluntary small-scale surveillance systems can complement statutory large-scale ones and work together locally, nationally, and internationally, it might be possible to detect small, unusual happenings that start in the community, such as emerging infectious diseases, thereby helping to avert worldwide outbreaks.
Acknowledgements
We wish to thank the local healthcare providers in Isa city, Kagoshima Prefecture, Japan, for their assistance with implementing and evaluating OSSS-Isa.
Funding
This research was supported by a Grant-in-Aid for Scientific Research (KAKENHI) Grant No. JP21K21169.
Conflict of interest
The authors declare no conflicts of interest.
References
You might also be interested in:
2012 - Physician in practice clinic: educating GPs in endocrinology through specialist-outreach