

Introduction
The provision of eye health care in regional Australia is challenging due to a longstanding medical workforce shortage in regional communities throughout Australia1. Data from the Australian Institute of Health and Welfare in 2019 found that major cities had a full-time equivalent rate (FTER) of four ophthalmologists per 100,000 persons, whereas inner regional areas had three FTER, outer regional areas had two FTER, and remote and very remote regions had insufficient numbers of ophthalmologists to calculate rates2. This shortage is even more pronounced in Western Australia (WA), where certain remote areas had coverage that was 20 times lower than metropolitan areas3. In addition, the recent national eye health survey (2025) demonstrated that remote areas have four times the rates of bilateral vision impairment compared to all other regions4.
Lions Outback Vision (LOV), established in 2010 with support from Lions Eye Institute and the University of Western Australia, is committed to improving eye health for people in rural and remote WA, particularly those in Aboriginal and Torres Strait Islander communities. It provides specialist ophthalmology services throughout regional WA by a mobile Vision Van (Fig1), a permanent tertiary eye clinic in Broome (in the Kimberley region) and scheduled outreach and telehealth, with no out-of-pocket costs for patients5. In addition, visiting optometry services reach 40 regional and remote communities. The multidisciplinary team includes ophthalmology specialists, junior doctors, optometrists, Aboriginal Health Workers and administrative staff. The Vision Van runs rotating circuits across WA (Fig2). The schedule is published online and adjusted yearly for demand, staffing, and local clinic and theatre availability6.
The Goldfields region (Fig3) does not have a resident ophthalmologist and is serviced by visiting outreach clinics. As of 2021, the full-time equivalent (FTE) of consultant ophthalmologists in the region was 0.1127. LOV utilises telehealth services as an adjunct to enhance access to specialist eye care quickly. However, in-person ophthalmology services remain a necessity to provide procedures and surgeries. Details specific to service delivery in the Goldfields are described in the Methods section.
This report describes the trends in the provision of specialist eye care in the Goldfields region for three common causes of vision loss in Australia: cataracts, diabetic retinopathy, and neovascular age-related macular degeneration8. Cataract surgery and intravitreal injections are used as the key indicators, as they represent the standard of care for managing these conditions9,10.
This report encompasses four key aspects of the service between 2017 and 2023: the number of ophthalmology services provided, changes in the cataract surgery rate over the specified period, service provision volume to Aboriginal and Torres Strait Islander patients, and change in the FTE consultant ophthalmologist time dedicated to the region.
We quantify clinical and surgical demand and FTER of specialist ophthalmologists in the Goldfields region. The purpose is to inform WA state public health service and Aboriginal Community Controlled Health Organisations (ACCHOs) of the workforce gap and demand for ophthalmology care, and the consequent need to scale up service provision in the region.
 Figure 1: The Lions Outback Vision Van mobile specialist clinic facility.
Figure 1: The Lions Outback Vision Van mobile specialist clinic facility.
 Figure 2: The Lions Outback Vision Van circuit across Western Australia.
Figure 2: The Lions Outback Vision Van circuit across Western Australia.
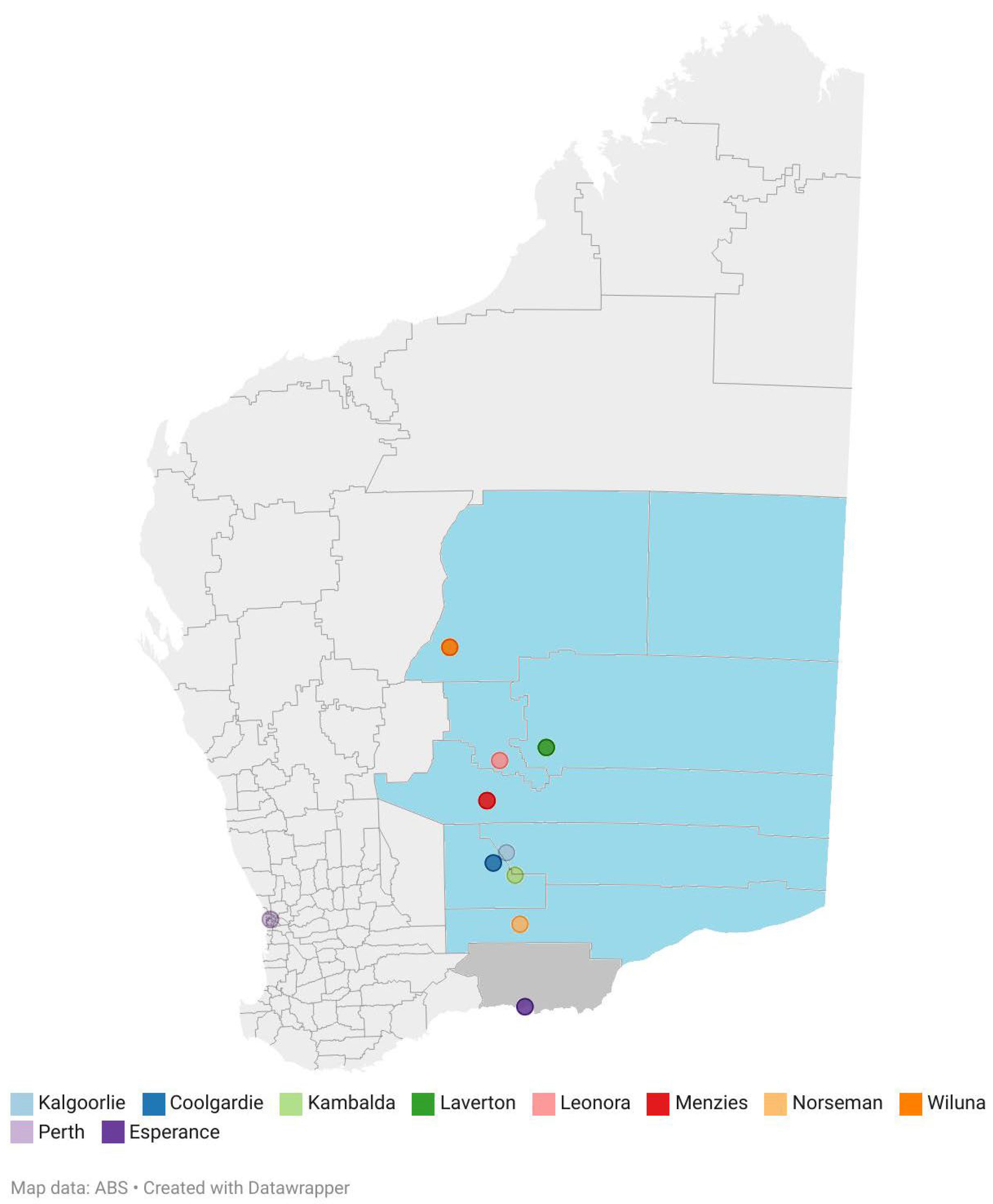 Figure 3: Map of Western Australia illustrating the Goldfields–Esperance region in relation to the capital city of Perth, Western Australia. Area highlighted in blue represents the region included in this study. Relevant locations serviced by Lions Outback Vision are labelled. ABS, Australian Bureau of Statistics. Area highlighted in blue represents the region included in this study. Relevant locations serviced by Lions Outback Vision are labelled. ABS, Australian Bureau of Statistics.
Figure 3: Map of Western Australia illustrating the Goldfields–Esperance region in relation to the capital city of Perth, Western Australia. Area highlighted in blue represents the region included in this study. Relevant locations serviced by Lions Outback Vision are labelled. ABS, Australian Bureau of Statistics. Area highlighted in blue represents the region included in this study. Relevant locations serviced by Lions Outback Vision are labelled. ABS, Australian Bureau of Statistics.
Methods
An observational retrospective clinical audit was conducted using data over a 7-year period (January 2017 to December 2023).
Setting and population
LOV is the sole local provider of ophthalmology services in the Goldfields region (which excludes Esperance). We defined the study region as the Australian Bureau of Statistics (ABS) Goldfields census area (Statistical Area Level 3). According to ABS census-night counts for the Goldfields census area, the population was 39,097 in 2016 and 38,267 in 2021. The census area covers 714,525 km2, which is a population density of 0.14 persons per km211.
Lions Outback Vision service model and referrals
Initially from 2010, LOV visited the Kalgoorlie Regional Hospital four to six times per year for surgery. In 2016, the Vision Van initiative commenced serving the region to provide specialist equipment in smaller communities throughout WA. The funding for the services was provided in equal parts by state government and federal government (via Rural Health West) and philanthropic donations for operations. The initial capital outlay included philanthropic support and federal government support. Further advocacy enabled a gradual increase in outreach specialist visits to the hospitals, which currently provide for monthly 3-day visiting clinics. LOV delivers care to the Goldfields region via outreach clinics, telehealth consultations, surgeries conducted at Kalgoorlie Regional Hospital, and services provided through the Vision Van mobile specialist clinic facility. Kalgoorlie Regional Hospital is one of the largest regional hospitals in WA, with a 106-bed inpatient facility, located almost 600 km from the nearest public tertiary centre12. Referrals are accepted from GPs, community optometrists, ACCHOs, and hospitals.
Data collection
De-identified data from all LOV patients seen in the Goldfields region from 2017 to 2023 were extracted from the LOV electronic medical records system. This included demographic and routine clinical data including sex, age, procedures performed, surgeries performed and location of service. Esperance data were excluded as LOV is not the sole provider of ophthalmological services there.
Culturally safe design
An Aboriginal Health Worker accompanies the Vision Van to coordinate care, engage with local communities, and work with ACCHOs to organise clinics and arrange patient transport. In partnership with ACCHOs, we also identify suitable locations for the Vision Van to run clinics, enhancing engagement with the Aboriginal communities. LOV was the first program to co-design, with the Aboriginal Health Council of Western Australia, the Community Compact for the Principles and Protocols for Delivery of External Health Services to Rural and Remote Communities in Western Australia, in 201613.
Data analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences for Windows v29 (IBM Corp; https://www.ibm.com/products/spss-statistics) and Microsoft Excel. Data were analysed both collectively over the 7-year period and by year. Data are presented as percentage and mean (standard deviation) for normally distributed data. The occasions of service in total per calendar year and per region were calculated. For common procedures including cataract surgery, intravitreal injections, laser (retinal laser, neodymium-doped yttrium aluminium garnet (Nd:YAG) peripheral iridotomy, Nd:YAG capsulotomy), pterygium surgery and other surgeries, the proportions of services per calendar year were compared using χ2 test.
The cataract surgery rate was determined by calculating the number of surgeries performed each year divided by the population of the Goldfields ABS census area (from the most recent census data available) and multiplied by 1 million. The 2016 ABS census data were used to calculate the rate for 2017–2020, and the 2021 census data were used to calculate the rate for 2021–20237,14. The full-time equivalent (FTE) was calculated by determining the number of days a consultant ophthalmologist worked in the region divided by 260 working days in a year. The FTER was calculated by dividing the FTE by population count (most recent census data available) and multiplying by 100,000.
Ethics approval
An ethics exemption was obtained from the University of Sydney Human Research and Ethics Committee, and patient consent was not required, in accordance with the National Health and Medical Research Council’s National Statement on Ethical Conduct in Human Research15. This project conforms to the principles of the Declaration of Helsinki 2013.
Results
Lions Outback Vision service in the Goldfields
The number of visits, FTE and FTER to the Goldfields region increased over time, as shown in Table 1. The greatest FTER was 0.342 in 2023.
Table 1: Full-time equivalent and full-time equivalent rate of consultant ophthalmologist time provided by Lions Outback Vision to the Goldfields region, Western Australia per year, 2017–2023
| Year | Outreach visits | Vision Van visits | FTE | FTER† |
|---|---|---|---|---|
| 2017 | 5 | 11 | 0.019 | 0.049 |
| 2018 | 20 | 25 | 0.077 | 0.197 |
| 2019 | 20 | 23 | 0.077 | 0.197 |
| 2020 | 17 | 43 | 0.065 | 0.167 |
| 2021 | 29 | 52 | 0.112 | 0.291 |
| 2022 | 33 | 58 | 0.127 | 0.332 |
| 2023 | 34 | 66 | 0.131 | 0.342 |
† 2016 Australian census data was used to calculate FTER for 2017–2020 (n=39,097) and 2021 census data was used to calculate the FTER for 2021–2023 (n=38,267).
FTE, full-time equivalent. FTER, full-time equivalent rate.
Total occasions of service
A total of 12,146 occasions of service were provided by LOV across the Goldfields–Esperance region in the 7-year period. A total of 330 occasions from Esperance were excluded. Of the 11,816 occasions of service included, 2854 (24.2%) were provided to Aboriginal and Torres Strait Islander people. The mean age of patients was 61.8 (standard deviation 17.9) years.
There has been a consistent increase in occasions of service provided to patients in the Goldfields region over time (Table 2), with a more than sixfold increase in occasions of service in 2023 (n=3007) as compared to 2017 (n=459). Most (82%) of the occasions of services were conducted in Kalgoorlie. The occasions of service provided to and the number of Aboriginal and Torres Strait Islander patients engaging the service has gradually increased over time (Table 2).
Table 2 shows the number of common procedures performed during each year. The frequencies of intravitreal injections, cataract surgery, pterygium surgery, and Nd:YAG laser capsulotomies increased. The frequencies of other surgery, retinal laser and Nd:YAG peripheral iridotomy were relatively stable. Of note, there was a statistically significant increase in the proportion of intravitreal injections. The surgical case rate in 2023 was 33.5%, representing the proportion of surgical procedures provided from all in-person attendances.
Table 2: Number (percentage) of all occasions of service provided to Aboriginal and Torres Strait Islander people and for specific procedures in the Goldfields region (which excludes Esperance), Western Australia, 2017–2023 per year and in total, 2017–2023
| Occasion of service | n (%) | Total | p-value (trend) | ||||||
|---|---|---|---|---|---|---|---|---|---|
|
2017 |
2018 | 2019 | 2020 | 2021 | 2022 | 2023 | |||
| All | 459 | 939 | 1188 | 1549 | 2112 | 2562 | 3007 | 11,816 | |
| Aboriginal and Torres Strait Islander people | 114 (24.8) | 269 (71.4) | 357 (30.1) | 421 (27.2) | 469 (22.2) | 469 (18.3) | 755 (25.1) | 2854 (24.2) | |
| Telehealth appointments | 56 | 159 | 182 | 228 | 331 | 267 | 248 | 1471 | |
| Intravitreal injections | 35 (7.6) *** | 83 (8.8) *** | 210 (17.7) | 429 (27.7)*** | 485 (23.0)* | 446 (17.4) | 589 (19.6) | 2277 (19.3) | <0.001 |
| Cataract surgery | 60 (13.1) *** | 120 (12.8) *** | 111 (9.3) | 77 (5.0) *** | 102 (4.8) *** | 195 (7.6) | 247 (8.2) | 912 (7.7) | <0.001 |
| Pterygium surgery | <5† | <5† | 6 (0.5) | 6 (0.4) | 12 (0.6) | 21 (0.8) | 14 (0.5) | † | 0.271 |
| Other surgery | 5 (1.1) | <5† | 6 (0.5) | <5† | <5† | 10 (0.4) | 9 (0.3) | † | 0.03 |
| Nd:YAG capsulotomy | 14 (3.1) | 8 (0.9) | 25 (2.1) | 33 (2.1) | 18 (0.9)^ | 47 (1.8) | 53 (1.8) | 198 (1.7) | 0.001 |
| Nd:YAG peripheral iridotomy | 5 (1.1) *** | <5† | <5† | <5† | <5† | 6 (0.2) | <5† | † | <0.001 |
| Retinal laser | 8 (1.7) *** | <5† | 11 (0.9)* | 7 (0.5) | <5† | 6 (0.2) | 9 (0.3) | † | |
*p<0.05, **p<0.01, ***p<0.001 when compared to 2023 with Bonferroni adjustment for pairwise comparisons.
† Data withheld to ensure patient privacy.
Nd:YAG, neodymium-doped yttrium aluminium garnet.
Intravitreal injections
There was a greater than 16-fold increase in injections performed in 2023 (n=589) compared to 2017 (n=35). Injections accounted for 19.3% of all occasions of services throughout the 7-year period, emerging as the most frequently performed procedure. The service transitioned from ad-hoc injection based on availability to a treat-and-extend protocol.
Cataract surgery
Phacoemulsification and intraocular lens implant are the standard technique utilised, similarly to the technique in most parts of Australia. The number of cataract surgeries performed increased fourfold over the 7-year period (n=247 in 2023 compared to n=60 in 2017). Figure 4 illustrates the calculated cataract surgery rate for each year. The rate increased from 1535 per million in 2017 to 3069 per million in 2018. There was a subsequent decline in 2018 and 2019 before an increase again after 2021. In 2023, the cataract surgery rate peaked at 6455 per million7,14.
According to data from the Australian Institute of Health and Welfare, ophthalmology was the surgical specialty with the highest median waiting time in 2021–2022, of 107 days2. Data from the Kalgoorlie Regional Hospital waitlist indicates that in December 2023 there were 290 surgeries pending of which 267 were for cataract surgery.
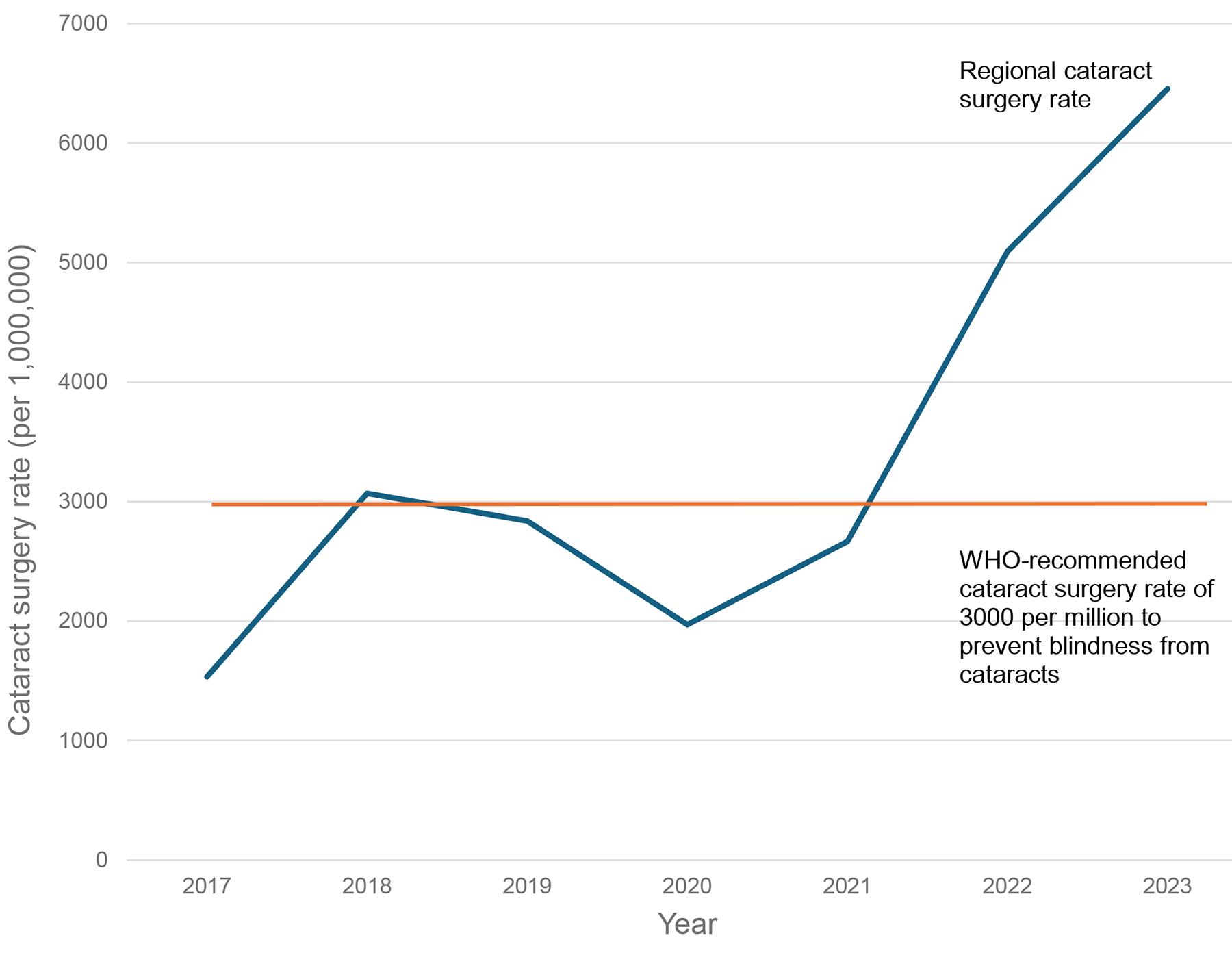 Figure 4: Cataract surgery rate per 1,000,000 population, Goldfields region, Western Australia, 2017–2023.
Figure 4: Cataract surgery rate per 1,000,000 population, Goldfields region, Western Australia, 2017–2023.
Telehealth
A total of 1471 telehealth appointments were conducted over the 7-year period. The utilisation of telehealth facilitated by regional optometrists has increased over time, with peak utilisation occurring in 2021. In 2017, there were 56 telehealth appointments, rising to 331 appointments in 2021.
Discussion
LOV has expanded ophthalmology services and ophthalmologist workforce in the Goldfields region annually for 7 years (2017–2023). The population of the region has remained stable throughout the report period and, despite the increasing service, the region still has a significant unmet need for ophthalmology services7,14. As a visiting service only, any acute eye care required has resulted in patients having to travel approximately 600 km to the nearest centre (the capital city of Perth)12.
Strong advocacy, collaboration with local services and teleophthalmology are key factors that have contributed to LOV’s successful expansion of service in the region. Through longstanding co-management between resident optometrists and the visiting ophthalmology services, efficient triage has meant the surgical case rate at 33.5% is higher than documented Australian outreach service averages (5–25%)16. LOV advocacy for optometry-facilitated telehealth reimbursement by Australia’s Medicare Benefits Schedule that commenced in late 2015 has formed the framework for co-management17. This enables effective and efficient triage as well as reducing time taken for patients needing surgery to be waitlisted18. This service model has been demonstrated to reduce surgical waiting times across regional towns in WA19. Specialist outreach services have been demonstrated to save patients both time and money, improve outcomes, as well as reduce government costs associated with access and transportation20-22.
Despite the expansion of services in the region, the specialist workforce supply in the region remains less than 11 times that of the national average2. Considering the significant population of 55,000 people in the Goldfields region and the distance from the metropolitan capital of Perth, there is a compelling case for establishing a full-time resident ophthalmology service in the area23-25. This would yield significant benefits over the current outreach model, including improved access to specialist eye care, more timely management and improved clinical outcomes, a reduced need for patients to travel to Perth, and cost savings for both patients and the health system. For example, the timing of intravitreal injections could be closely tailored to patients’ needs, as practised in major centres26-28, and treatments such as retinal laser could be performed in the region. Over time, we expect that community awareness of the service would also grow, leading to improved access, patient attendance and potentially contributing further to closing the gap for Aboriginal and Torres Strait Islander eye health29.
Implication for policy and practice
The results of this audit support scaling up ophthalmology services in the region, potentially commissioning a resident ophthalmology FTE role in the Goldfields region to meet clinical and surgical demand, reduce the travel burden and improve equitable access to care. Recent investment in regional public ophthalmology services in the Kimberley region in northern WA to match the Australian average have seen significant improvements in access for surgical pathways (particularly for the Aboriginal and Torres Strait Islander population), which is now equitable in the region. Similar investment to meet the population-based demand could yield improved access, which would result in prevention of blindness30. The recent Australian Eye and Ear Health Survey revealed the rates of bilateral vision impairment for the population aged over 50 years were four times higher in remote regions and there is an urgent need for accessible services with no cost barriers, closer to where people live4.
Conclusion
Despite growth in activity under the LOV model, the cataract surgery rate in the Goldfields region of WA is still below target and ophthalmologist FTER is below national levels. The region should scale services by planning for a state-funded, permanent resident ophthalmology service to meet the population-based demand and tackle the burden of vision loss and blindness.
Funding
No funding was received for this research.
Conflicts of interest
LOV provides ophthalmology services to the community described in this report.
AI disclosure statement
The authors did not use any artificial intelligence tools to formulate hypothesis, design, conduct experiments, draft part of paper, summarise, paraphrase or significantly revise, synthesis textual contact, translate part or entirety of the paper, to extract data for review of the literature, to identify knowledge gaps or to generate synthetic data and images reported in the paper or used in research.