

Introduction
Historically, health research has discredited Aboriginal and Torres Strait Islander cultural values, exploited communities, and perpetuated unjust health disparities1-3. Equitable and genuine research partnerships with Aboriginal and Torres Strait Islander Peoples are hallmarks of high-quality, ethical research1,2,4. Research centred on such partnerships is needed to support Indigenous sovereignty, ensure research is relevant, prioritise community needs and aspirations, and contribute to the development of holistic, accessible, and equitable healthcare services5. This requires attention to ethical conduct throughout the research process and active reflection upon research principles and goals. How do we ensure that research involving Aboriginal and Torres Strait Islander Peoples is community-led, reflects shared values and diverse needs, and guarantees that Aboriginal and Torres Strait Islander communities are the primary benefactors?
The CONSolIDated critERia for Strengthening the Reporting of Health Research Involving Indigenous Peoples (CONSIDER statement) was developed to advise on approaches to conducting research with Indigenous Peoples1. Based on a collaborative review and meta-synthesis of several national and international statements regarding the ethical conduct of Indigenous health research, the CONSIDER statement includes eight domains comprising 17 criteria. The domains are governance, relationships, prioritisation, methodologies, participation, capacity, analysis and findings, and dissemination (Fig1).
Our project, ‘Enhancing harm reduction services (BBV and STI) for Aboriginal and Torres Strait Islander people who inject drugs through improved engagement’ (hereafter referred to as the project), explored opportunities to improve equitable access and cultural safety of harm reduction services, and to thereby support better health outcomes for Aboriginal and Torres Strait Islander people who inject drugs, including lower rates of exposure to blood-borne viruses (BBVs) and STIs. Aboriginal and Torres Strait Islander people who inject drugs have high rates of exposure to BBVs and STIs compared to non-Indigenous people who inject drugs6. Accessible, holistic, and responsive harm-reduction services, including needle and syringe programs, are essential for reducing the transmission of BBVs and STIs among people who inject drugs7. Despite their demonstrated success8,9, harm-reduction programs are not always designed to meet the diverse needs of Aboriginal and Torres Strait Islander Peoples, including those living in regional and remote locations, who face barriers to accessing health services due to the social marginalisation of injecting drug use10, a lack of integrated and holistic service provision11, and experiences of stigma, discrimination and racism12. The project aimed to work in partnership with local stakeholders and Aboriginal and Torres Strait Islander people with lived and living experience of injecting drug use to identify culturally safe approaches and local priorities towards developing harm reduction services for Aboriginal and Torres Strait Islander people who inject drugs. The project rationale reflected sustained disparities in increasing BBV and STI rates13,14 and gaps in knowledge about designing culturally responsive services and resources for Aboriginal and Torres Strait Islander with lived and living experience in regional Queensland, Australia15. The project adhered to national ethical guidelines for conducting research with Indigenous communities, including the AIATSIS Code of Ethics for Aboriginal and Torres Strait Islander Research and the NHMRC ethical guidelines for research with Aboriginal and Torres Strait Islander Peoples11,16.
The aim of this study was to critically assess the project’s research process against the CONSIDER statement domains. This involved reflexive analysis of meeting notes, stakeholder feedback from fieldwork activities, correspondence with research partners, and stakeholder interviews.
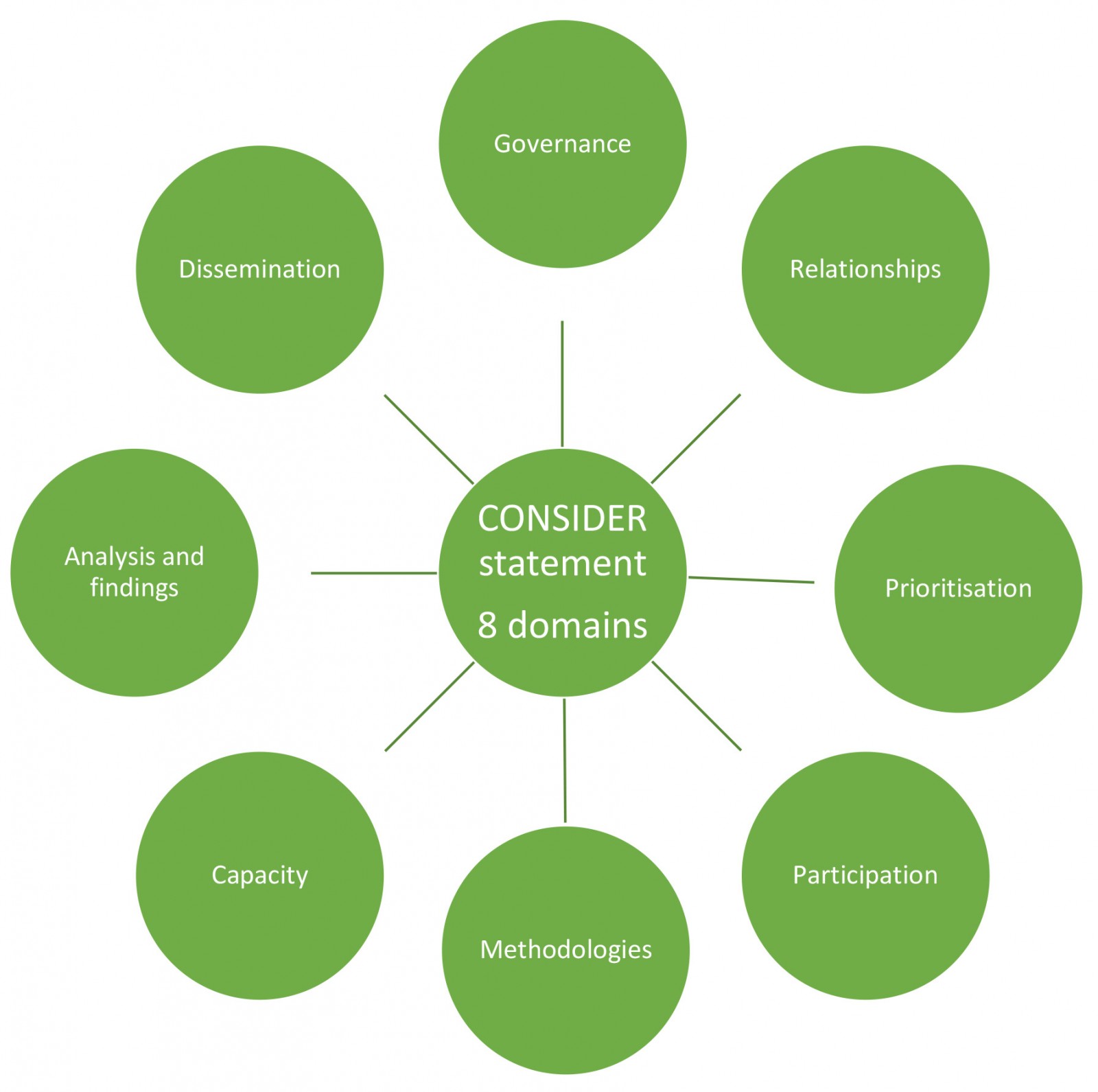 Figure 1: The eight CONSolIDated critERia for Strengthening the Reporting of Health Research Involving Indigenous Peoples (CONSIDER statement) domains.
Figure 1: The eight CONSolIDated critERia for Strengthening the Reporting of Health Research Involving Indigenous Peoples (CONSIDER statement) domains.
Methods
Project design
The project was a partnership between the University of Queensland’s School of Public Health, the Queensland Aboriginal and Islander Health Council (QAIHC), the Queensland Injectors Health Network (QuIHN), and Youth Link. QAIHC is the Queensland peak body representing Aboriginal Community Controlled Health Organisations, and advocates for accessible and equitable comprehensive primary health care for Aboriginal and Torres Strait Islander Peoples. QuIHN and Youth Link both operate primary NSPs that dispense sterile injecting equipment to people who inject drugs and adjacent services including group counselling and homelessness support. Several other partnerships were established with alcohol and other drugs services, sexual health services, and other social and emotional wellbeing services. The chief investigators comprised Aboriginal and non-Aboriginal members including a proud Mbabaram man and lead investigator from QAIHC. The project coordinator is a proud descendant of the Yamatji Peoples and had an active role in sharing knowledge with the chief investigator team, ensuring research activities and processes were culturally safe and accounted for cultural practices such as Sorry Business.
Recruitment and research activities
We recruited 109 participants who met the eligibility criteria of identifying as Aboriginal or Torres Strait Islander and having injected drugs within the past year. Participants were recruited at community-based NSPs at each research site using location-based convenience sampling and took part in point-of-care testing for a range of BBVs and STIs, a supported quantitative survey, and interview yarns. NSP staff at each site informed eligible clients about the project. Participants were offered a $40 voucher for completing the point-of-care testing and survey, and a $20 unconditional, pre-paid, refer-a-friend incentive was offered to participants to refer a friend or family member to the research. Relying on the principle of reciprocity, participants received this voucher regardless of whether their referral participated. Participants who completed an interview yarn were offered an additional $40 voucher. Flyers about the research were also distributed by some community pharmacies that dispense injecting equipment. Table 1 outlines the project’s research activities and data sources.
Table 1: Activities and data sources – qualitative and quantitative methodologies17-19
| Activity | Description/rationale |
|---|---|
| Survey self-administered by Aboriginal and Torres Strait Islander people with lived and living experience of injecting drug use | This survey gathered information regarding NSP participants’ experiences accessing harm-reduction services. Questions pertained to their experiences accessing services, patterns of obtaining injecting equipment, and factors that may impact access, including discrimination and stigma. Demographic data, service use and other administrative data were collected. Validated instruments were used to measure levels of discrimination and stigma. Strength-based questions were included to acknowledge the resilience of participants13. Participants provided informed consent and completed the survey on an electronic device with support from the research coordinator while waiting for their point-of-care testing results (see below). |
| Clinical intervention | Point-of-care testing in Australia has become an increasingly accessible and beneficial testing model that provides rapid diagnostic results for a range of BBVs and STIs14,15. This study piloted point-of-care testing at NSP study locations to evaluate its role in increasing client engagement and access to referral and treatment. Best-practice testing protocols and referral procedures were used for all conditions, developed by QuIHN in consultation with the Queensland Syphilis Surveillance Service and research partners. Those testing positive for any BBV/STI were directly referred to services for confirmatory testing (where applicable), assessment, and care, including the Better Access Medical Clinic at the QuIHN Brisbane site and sexual health services at the other sites. |
| Semi-structured interviews with Aboriginal and Torres Strait Islander people with lived and living experience of injecting drug use | A proportion of NSP participants (14/109) were invited to participate in a semi-structured interview yarn. Questions were open-ended, pertaining to participant expectations, needs, and experiences accessing harm-reduction services, including NSPs and mainstream healthcare services. These qualitative interview yarns offered a more in-depth understanding of participant experiences and were analysed in parallel with the quantitative survey data. |
| Preliminary stakeholder interviews | Preliminary stakeholder interviews wereconducted with program managers and frontline staff, including Aboriginal Health Workers, from QuIHN, Youth Link, and other health services such as sexual health and alcohol and other drugs services. Questions pertained to observations of how Aboriginal and Torres Strait Islander Peoples experience harm-reduction services, emerging health issues for Aboriginal and Torres Strait Islander people who inject drugs, recommendations for service design, barriers and enablers in the community that affect client engagement, and suggestions for the NSP participant surveys. These interviews informed subsequent stages of the research. |
| Stakeholder workshops | Workshops were co-hosted by partners and stakeholders at health or community service sites after fieldwork, involving collaborative yarning activities to explore ideas and uphold ethical research governance. Preliminary findings were presented, and participants collaborated in yarning circles to interpret findings and explore ideas, using them to guide the development of harm-reduction services and policy. |
BBV, blood-borne virus. NSP, needle and syringe program. QuIHN, Queensland Injectors Health Network.
Data analysis
Analysis of meeting notes, stakeholder feedback from fieldwork activities, correspondence with research partners, and stakeholder interviews was informed by reflexive thematic analysis6,20, which involves the researchers’ interpretive analysis of the data and their reflective and thoughtful engagement with the analytic process. The process of theme development was flexible and organic, did not involve codebook development, and evolved throughout the analytical process20. Themes were produced by organising codes around core commonalities that the researcher interpreted from the data20. Throughout the analysis, we engaged in iterative reflection, challenging initial interpretations and seeking alternative explanations, and obtained feedback from colleagues to gain diverse perspectives, including Aboriginal co-authors.
Ethics approval
This study is part of a project funded by the Sexual Health Ministerial Advisory Committee Research Fund. Ethical approval for this project was obtained on 12 August 2021 from the University of Queensland Human Research Ethics Committee (approval number: 2021/HE000742).
Results
Three major themes emerged following reflexive analysis: equal research partnerships, collaborative stakeholder engagement and recruitment, and capacity building. We drew on the CONSIDER statement to critically assess these fundamental aspects of the project’s research design and processes.
Theme 1: Equal research partnerships/governance
Domains 1 (governance) and 2 (prioritisation) of the CONSIDER statement recommend that partnerships between the research institution and Indigenous organisations are established to recognise the ‘centrality of Indigenous self-determination and leadership’ in research conduct1. As part of this domain researchers must describe partnership agreements between the research institution and Indigenous-governing organisation for the research, describe accountability and review mechanisms within the partnership agreement that addresse harm minimisation, and specify how the research partnership agreement includes protection of Indigenous intellectual property and knowledge arising from the research, including financial and intellectual benefits generated (eg development of traditional medicines for commercial purposes or supporting the Indigenous community to develop commercialisation proposals generated from the research.
This project established equal research partnerships with Aboriginal and Torres Strait Islander organisations (domain 1), ensuring that research processes honoured cultural safety and meaningful community engagement. The research team carried out extensive preliminary consultations with QAIHC to support development of the research aims and proposal prior to funding submissions. Co-investigators included QAIHC staff members, including an Aboriginal lead investigator who brought extensive experience to the research at both policy and community levels (domain 2). QAIHC actively participated in project planning and the establishment of fieldwork sites and processes. Drawing on local knowledge of organisations within the sector, QAIHC advised on stakeholder engagement at each study location, supporting the research team in building relationships with local services. Regular team meetings strengthened rapport and facilitated a space for collaborative yarning, research accountability, and reporting progress (domain 1). Building rapport was important; research partnerships may be difficult to manage in their early stages and require considerable time to establish trust to achieve research outcomes7. Meetings also provided an opportunity to adapt project timelines to fit with stakeholder priorities, including local COVID-19 public health responses.
QAIHC provided cultural expertise on resources such as the terms of reference for Aboriginal and Torres Strait Islander people with lived and living experience, ensuring these resources aligned with the interests and legal rights of Aboriginal and Torres Strait Islander Peoples (domain 4 methodologies: ‘Describe the methodological approach of the research including a rationale of methods used and implication for Indigenous stakeholders’, ‘Describe how the research methodology incorporated consideration of the physical, social, economic and cultural environment of the participants and prospective participants as well as Indigenous worldviews’). The project also received guidance from an Aboriginal research champion and care coordinator from the Institute for Urban Indigenous Health in Brisbane. They gave advice on the survey and interview yarn instruments, including culturally representative gender expressions (eg sistergirl, brotherboy) and strength-based questions on stigma and discrimination.
Under domain 5 of the CONSIDER statement, researchers must specify how individual and collective consent was sought to conduct future analysis on collected samples and data and described how the resource demands (current and future) placed on Indigenous participants and communities involved in the research were identified and agreed upon, including any resourcing for participation, knowledge, and expertise. A collaborative research agreement (domain 1 (governance) and domain 5 (participation)) was signed by each organisation and outlined the funding, roles, responsibilities and actions of each partner. Such agreements must be consistent with the principles of honesty, transparency, fairness, respect, and accountability21. Aboriginal and Torres Strait Islander Peoples have a right to maintain, protect and develop their intellectual property over such cultural heritage, traditional knowledge, and traditional cultural expressions1. The research team agreed to take all necessary steps to protect, maintain and enforce Indigenous intellectual property made available for the purpose of performing the project and protection of intellectual propertyu emphasised with participants during consent process for team meetings and individual yarns. Stakeholders were given the opportunity to provide feedback on research findings and outputs during workshops and inform co-designed resource development (domain 5 (participation)). Researchers ensured knowledge and data collected during project are available for use by current and future generations, and project findings will be disseminated to key Indigenous and non-Indigenous health services within the sector, including participating NSP sites (domain 5 (participation)).
Theme 2: Collaborative stakeholder engagement and recruitment
Domains 2 (prioritisation) and 3 (relationships) of the CONSIDER statement emphasise that connecting with relevant stakeholders provides greater opportunities for designing health programs to meet the needs of Aboriginal and Torres Strait Islander Peoples14. Under domain 3, researchers must specify measures that adhere to and honour Indigenous ethical guidelines, processes, and approvals for all relevant Indigenous stakeholders, recognising that multiple Indigenous partners may be involved, report how Indigenous stakeholders were involved in the research processes, describe the expertise of the research team in Indigenous health and research. Some research team members were outsiders to study locations; thus, it was imperative to draw on the knowledge of local communities held by stakeholders, who possess a unique understanding of community needs and harm-reduction service characteristics, and who have had considerable experience engaging with local people who inject drugs and other socially marginalised groups10.
All stakeholders played an active and valued role in the implementation of the research, helping to connect researchers with study participants and establish treatment referral pathways, and were provided with regular progress updates (domain 3). The research team conducted interviews with stakeholders at an early stage of the research to gather advice on engagement with people with lived and living experience, research processes, and survey questions. Fieldwork support from stakeholder services was provided only to the extent permitted by available time and resources (domain 6 (research capacity): ‘Explain how the research supported the development and maintenance of Indigenous research capacity’, ‘Discuss how the research team undertook professional development opportunities to develop the capacity to partner with Indigenous stakeholders’). Cairns Sexual Health staff assisted Youth Link NSP workers with point-of-care testing when they had capacity. However, the level of demand for testing far exceeded expectations at the Cairns Youth Link site; participants often waited in line for testing. This created logistical problems and pressure on the staff conducting the testing, meaning some participants were turned away and told to return the following day. In future, careful contingency planning is needed to ensure participating services are not overburdened and participant engagement is not jeopardised.
Theme 3: Capacity building
Under domain 6 (research capacity), ‘research should be of benefit to Indigenous stakeholders as well as to the research group’1. Reporting the capacity-building components of the project reinforces the research team values for working with Aboriginal and Torres Strait Islander Peoples1. The project created opportunities to embrace the knowledge of Aboriginal and Torres Strait Islander Peoples through their active engagement in the research process. The project coordinator, who organised and conducted most of the fieldwork, is a proud Aboriginal person (domain 6). Their professional development and right to self-determination were supported by all project partners throughout the research, and they were provided with appropriate research training (eg research design, interview skills, and data analysis). Specific expertise brought by the project coordinator and stakeholders included knowledge of racism and the impacts of colonisation, culturally informed research skills (eg yarning), and ways of identifying community needs (domain 6). The Aboriginal research coordinator presented findings at international and national conferences, including the 2022 World Indigenous Peoples Conference on Viral Hepatitis, and the 2024 UNSW Tackling Stigma Conference. All conference materials presented acknowledged Aboriginal and Torres Strait Islander authors and project contributors. Aboriginal and Torres Strait Islander partners and stakeholders will be consulted on all publications and reports arising from this project (domain 7 (analysis and interpretation): ‘Specify how the research analysis and reporting supported critical inquiry and a strength-based approach that was inclusive of Indigenous values’).
This project facilitated community capacity building at each study location (domain 6). Partners and stakeholders co-hosted workshops where preliminary research findings were presented, and participants helped contextualise and interpret them and guide the development of service recommendations and policy. These workshops promoted inter-agency collaboration and revitalised inter-agency networks, which may have increased the capacity of services to deliver actionable grassroots change (domain 6). Workshop participants included Aboriginal and Torres Strait Islander care services, Queensland Sexual Health and Wellbeing teams, mainstream healthcare and alcohol and other drugs services. A representative of people with lived and living experience participated in one workshop. Reciprocity was the foundation of all workshops, demonstrated by stakeholder collaboration to identify recommendations, including diverse community priorities and potential resources that will directly benefit communities (eg service map and increased outreach) (domain 8 (dissemination)).
Discussion
The CONSIDER statement was a valuable tool for critical reflection on research partnerships and processes undertaken in the harm-reduction project. Researchers identified that project timelines should be flexible and adaptive. Future research should allow feasible time frames for consultation with local health services and service providers. Engaging with research projects can be challenging for people with lived and living experience; it is recommended that researchers engage meaningfully and transparently throughout the research process, allowing adequate time to build reciprocity and trust. Using Indigenous research methodology with yarning as a method strengthened strengthened cultural safety and supported ethical research practices.
Resourcing and allocating time for community consultation
Under domain 5 (research participation), researchers must consider how to resource the participation of Indigenous partners and investigators, including providing adequate time and funding for face-to-face consultation1. The 2-year project duration did not allow sufficient time to initiate and build sustainable relationships with local Aboriginal and Torres Strait Islander stakeholders to conduct all research activities in line with existing community efforts. In previous research, Aboriginal and Torres Strait Islander communities and services have expressed feeling pressured and hurried during research projects12, making participation unsafe, unethical and burdensome. In future, respectful and reciprocal relationships between stakeholders and researchers must be built slowly, safely, and throughout the research process. Researchers must deeply listen to needs of local services and appreciate that their capacity may be limited at times22. Relationship building and consultation are fundamental in developing research plans and processes that contain frameworks of ethical practice and align with the values and goals of local stakeholders and communities.
Challenges and recommendations for peer engagement
‘Peers’ or people with lived and living experience of injecting drug use are vital stakeholders and should be engaged in processes of understanding and reporting on research data, ensuring findings are relevant and appropriate21,22. People with lived and living experience can help researchers understand and contextualise complex perspectives and experiences and ensure that sensitive issues are interpreted and managed in a respectful manner21. Service and community perceptions of client needs and substance-use patterns may not reflect the real experiences and histories of people who inject drugs. Thus, the direct inclusion of Aboriginal and Torres Strait Islander people who inject drugs – in research, programming, and policy development – is critical.
One Aboriginal person with lived and living experience was recruited through stakeholder connections. Drawing on their knowledge of local services and barriers faced by Aboriginal and Torres Strait Islander people who inject drugs, they reviewed study materials, including the survey and interview yarn protocol, and participated in a stakeholder workshop, for which they were paid.
A major challenge for the project was an inability to form a full peer representative group, comprising people with lived and living experience from all study locations, partially due to time and resourcing restraints. This limitation may also reflect inherent challenges of finding people with lived and living experience who are willing to engage in research. People may be reluctant to engage due to concerns about privacy, stigma, racism, and distrust of academic or government institutions23,24. Some may also be concerned about the burden of participation or reliving distressing memories24-27. There were issues organising peer remuneration and communicating the requirements of this complex, unfamiliar, and often lengthy process. In future, it is recommended that all documentation for remuneration is explained and completed in person at the earliest opportunity (where possible) to reduce the risk of conflict and confusion and ensure people with lived and living experience do not feel undermined. Researchers should engage meaningfully and ethically with people with lived and living experience in transparent and trustworthy manners throughout the research process to develop reciprocity and support the confidence and safety of people who inject drugs24.
Collaborative yarning methodology
Incorporating collaborative yarning as an Indigenous research methodology was a major strength of this project. Yarning is a method of knowledge exchange that embodies the oral traditions of Aboriginal and Torres Strait Islander Peoples28 and is conducive to an ‘Indigenous way of doing things’. Its strength is in the cultural safety it creates for Aboriginal and Torres Strait Islander Peoples29. Bessarab and Ng’andu29, authors of the most well-known yarning scholarship, propose there are four different types of yarning: social, collaborative, therapeutic, and research topic. Research topic yarning was used during participant interview yarn and encouraged in-depth discussions that resulted in ‘thick descriptions’ of a range of issues29. A semi-structured and relaxed interview yarn format generated in-depth discussions, ensuring participants’ narratives and truths were prioritised and valued. Prior to the interview yarn, the research coordinator introduced themselves and shared their cultural identity and intentions for the interview. This initial social yarning built trust and established commonalities, enabling the interviewer to explore the topic in more depth and potentially identify themes that a more formal interviewing style may have missed.
Collaborative yarning was used in the stakeholder workshops, to explore ideas and share interpretations of research findings. The process entailed dividing participants into smaller yarning groups of four or five people. To guide discussions, groups were provided with themes and prompts related to the project findings, policy recommendations, and resource development. The first yarning group activity was focused on program design and delivery and explored ideas around peer support, destigmatising services, service modalities, staffing, and staff development. The second group activity focused on policy and health service impacts, exploring ideas and recommendations for health service navigation, interagency coordination, policy and resourcing to support program development, and how to create enabling service environments and cultures. These smaller yarning groups allowed members to safely voice their views in an informal, respectful space. Butcher’s paper was supplied so participants could write or draw ideas if they felt uncomfortable speaking to the group. These yarns were consensually recorded and photographed.
There is potential for yarning methods to be subjected to cultural appropriation from dominant cultures and institutions, that may view connection and relationality at a surface level and fail to acknowledge the deeper meaning and importance of such knowledge exchange and connection30,31. It is imperative that Aboriginal and Torres Strait Islander researchers review and refine research methods and data analysis so that we can maintain ‘holism of stories’30,32.
Limitations
A major limitation to using the CONSIDER statement was that it was reflected upon after the research took place. In future, researchers should intend to use the CONSIDER statement as a guiding tool to inform, advise, and plan research with Aboriginal and Torres Strait Islander communities, organisations, and stakeholders. It is hoped this critical refection inspires other researchers to utilise the CONSIDER statement as a tool to inform research partnerships with Aboriginal and Torres Strait Islander Peoples and improve health outcomes through emancipatory and culturally responsive research practices.
Conclusion
The CONSIDER statement was a valuable tool for critically reflecting on the project’s research partnerships and processes. Researchers identified that project timelines should be flexible and that, in future, adequate time should be allocated for building relationships with local services and Aboriginal and Torres Strait Islander stakeholders. Engaging with people with lived and living experience can enhance the integrity of research; it is recommended that researchers engage meaningfully and transparently throughout the research process to develop trust and build reciprocity. Using collaborative yarning as an Indigenous research method strengthened cultural safety, encouraged two-way knowledge sharing, and supported ethical research practices. Researchers must continually review and revise Indigenous research methods to ensure they are grounded in Indigenous ways of doing and being and not subjected to surface-level Western appropriations. A major limitation was that the CONSIDER statement was reflected upon after the research took place. In future, researchers should use the CONSIDER statement as a guiding tool to inform and plan research with Aboriginal and Torres Strait Islander communities and stakeholders. We hope that this critical reflection inspires other researchers to utilise the CONSIDER statement as a tool to inform research partnerships with Aboriginal and Torres Strait Islander Peoples and improve health outcomes through emancipatory and culturally responsive research practices.
Acknowledgements
The authors and project members extend their respect and gratitude to the Aboriginal and Torres Strait Islander people with lived and living experience, the various stakeholders and harm reduction workers involved in this project. They acknowledge Nadine Horasak (Youth Link), Julie Markham (QuIHN), Nikki May (QuiHN), and Carla Gorton (Cains Sexual Health Service) for their input, passion, and support throughout different phases of the project.
Funding
This project was funded by a Sexual Health Research Fund Grant and was a collaboration between the University of Queensland, Queensland Aboriginal and Islander Health Council, QuIHN, and Youth Link, and was funded by the Queensland Sexual Health Research Fund.
Conflicts of interest
There were no conflicts of interest for this study.
References
You might also be interested in:
2022 - Social support in rural communities in Manabi province, Ecuador
2005 - Recruiting undergraduates to rural practice: what the students can tell us