





Context
The US has a shortage of primary care providers, including physicians, nurse practitioners and physician assistants trained in pediatrics and mental health1. The literature demonstrates complex issues that contribute to the challenges of providing primary care services, which include growing provider shortages, especially in rural areas and pediatric specialties; limited mental health training; and limited exposure to rural care2,3. Nurse practitioners serve as providers and have proven high-quality care, positive patient outcomes, lower medical costs and higher quality of life among patients4,5. However, the transition to practice in rural settings is challenging and requires training and support beyond basic nurse practitioner education for many reasons. Most graduate-level nurse practitioner programs exist within universities located in urban areas of the US. Within rural health, finding willing preceptors to train students is difficult based on patient volume, inadequate office support and competition for placements among disciplines. Students may suffer hardship traveling to remote areas, unless they already live there and are interested in pursuing positions close to home2. Postgraduate fellowship and residency programs that offer training beyond traditional nurse practitioner programs began in 2007 in the US and offer additional training opportunities, but most pediatric programs exist in acute, critical and subspecialty areas of practice, with extremely limited pediatric-specific primary care programs identified6,7.
Considering demand for primary care and mental health providers in rural areas of the US and limited training, data regarding the pediatric population adds to care concerns. Chronic health conditions occur in one out of four children and pediatric mental health diagnoses have increased significantly, especially since the pandemic8,9. Between 2016 and 2020, 20–35% more children were diagnosed with anxiety and depression, with pediatric deaths rising8. Pediatric nurse practitioners (PNPs) in primary care must provide high-level care, astute identification of patient diagnoses and implementation of evidence-based care for a vulnerable population. Limited but promising reports indicate that nurse practitioners who enter practice through residencies or fellowships have better adjustment to practice, reduced burnout and greater intent to stay in their roles10. In 2010, the US National Academy of Medicine identified the necessity for fellowship and residency programs – and, based on provider and patient need, justification for nurse practitioner fellowship programs in primary care and mental health within rural and underserved areas is apparent11. These popular positions offer gradual transition to practice with opportunities for specialized training and clinical experience10,12.
While there is a dearth of research on educational needs of nurse practitioners working in rural health care, available data indicate barriers including few preceptors, competition for site placement and challenges getting trainees to travel and live in rural areas, contributing to reduced recruitment and retention2. However, exposure to clinical care in rural settings, having a supportive mentor, responsibility for a panel of patients, and a competitive salary and benefits package are factors that support nurse practitioners taking jobs in rural areas13,14.
Frameworks and examples to support high-quality pediatric primary care in rural areas are essential to developing programs, but additional data about successful postgraduate nurse practitioner training programs including efficacy and outcomes are needed. The purpose of this article, using a pediatric primary care fellowship example, is to outline the needs of graduate nurse practitioners, describe the rationale for postgraduate training, highlight our program content and structure, and identify ways to collect data for evaluating the quality and efficacy of primary care fellowship programs.
Issue
Nurse practitioner transition to practice
Nurse practitioners are well positioned to provide primary care services for populations of all ages, but undergraduate pediatric nursing content in the US has decreased based on limited opportunities for clinical experiences and the need to focus on technology, patient complexity and additional general nursing content, leaving nurses without these skills or knowledge when entering PNP programs15,16. Nurse practitioner graduates are expected to quickly support practice costs and overheads, therefore limiting time to learn the provider role, resulting in frustration, stress and decreased retention3,4. Within the rural map, nurse practitioners face challenges including keeping track of rapid changes in care practices and delivery, increasing patient complexity, limited support staff and a lack of time to navigate medical records, document and communicate with patients10. A formal fellowship process offers longer and more in-depth orientation, especially in rural areas where providers must take on additional and essential care in mental health and subspecialty services due to lack of local resources15,17.
An exemplar of rural and underserved communities
Within the state of Delaware, healthcare access is a concern, with more than two-thirds of the state considered rural and two of the three counties representing medically underserved areas18. Approximately 17% of the 230,000 children live in poverty, and this figure is growing19. Overall, 13% of children aged 10–17 years have a serious mental health condition and 52% of those aged 12–17 years have diagnosed but untreated depression20. The number of children experiencing anxiety and depression increased 33% since 2016, and Delaware is ranked 29 in the least healthy states for maternal and child health8. Delaware is ranked 38 among the states with the highest incidence of illicit drug use by children, with 9.9% of adolescents involved and deaths from overdose increasing20. Poverty is a social determinant of health driving child health issues contributing to behavioral and mental health problems, preterm birth, low birthweight and high first-year mortality rates. Table 1 displays data regarding maternal–child health issues from the state of Delaware in 2023 as compared to national averages21. Poverty, racial and ethnic discrimination and/or adverse childhood events are additional factors contributing to the incidence of pediatric physical and mental health conditions, but often go unnoticed and untreated19.
A large pediatric health system serves Delaware in addition to parts of Maryland, Pennsylvania and New Jersey, with 67% of the primary care centers located in US Healthcare Provider Shortage Areas. Families often travel 1–2 hours to access subspecialty care and mental health support, contributing to missed school days and meals, which contributes to food insecurity. The extensive health issues, and awareness of the social determinants of health with limited community resources, contributed to pursuit of PNPs as primary care providers and the fellowship as one way to implement sustainable high-quality comprehensive care.
Table 1: Data relating to infant and maternal health status in Delaware and the US
| Issue |
Delaware21 (%) |
US21 (%) |
|---|---|---|
| Prematurity | 11.0 | 10.5 |
| Low birthweight | 9.1 | 8.5 |
| Infants dying prior to age 1 year | 0.51 | 0.54 |
| Infants born to women who did not receive adequate prenatal care | 22 | 24.4 |
| Uninsured women of childbearing age | 6.6 | 11.6 |
Initiation of an advanced practice provider primary care fellowship
A lack of PNP educational programs in Delaware, nurse practitioners who are at or close to retirement age, and limited resources for mentoring and precepting, were additional reasons to initiate the PNP primary care fellowship in 201722,23. A targeted review of the literature demonstrated no PNP primary care fellowship programs, and limited content discussing family and pediatric acute care curriculums. Only three articles reported outcome data related to their programs4,5,24. As such, our aim was to develop a program to support nurse practitioners in their transition to independent practice with a focus on mental and rural health to meet the needs of our communities.
Due to the lack of outcomes related to fellowship programs, we felt it essential to identify and measure key elements supporting the development and sustainment of similar programs. This led to the creation of our secondary aim: measuring nurse practitioner confidence and competence over time to ensure program success and educational gaps of new-to-practice nurse practitioners are met.
Anxiety and lack of competence are associated with increased burnout and reduced retention, so these were the focus of our primary outcomes. The State Trait Anxiety Inventory assesses anxiety related to confidence25, and competence is evaluated using the Primary Care Knowledge Resident Competency Assessment developed by the Veterans Affairs centers for primary care26. This tool was modified to reflect the pediatric primary care competencies outlined by the National Organization of Nurse Practitioner Faculties27. Table 2 outlines these competencies. Confidence and competency are assessed at baseline, 1 month, 6 months and 12 months for all fellows in our program.
Additional program elements were modeled after other successful nurse practitioner fellowship programs10,12 and refined for pediatric patients living in rural populations. Our fellowship program follows a traditional academic year starting and ending in October. Annually, we ask fellows to provide program feedback so content can be modified to better support a robust and effective curriculum.
Characteristics of pediatric patients living in Delaware, geography and limited specialty care access and ongoing need to retain primary care pediatric providers added to the mission. Stakeholder support came from the institution’s chief nurse and primary care physician director. Experienced nurse practitioners were recruited as preceptors/mentors and educators. Practice manager support was required for PNP integration into primary care practices, and both patient and provider scheduling22,28. Extremely limited previous data documenting outcomes indicated a need for early and ongoing program evaluation.
The PNP primary care fellowship includes education in varied subspecialty clinics for the diagnosis and management of common problems and assists in keeping the child within the purview of the patient-centered medical home, limiting travel and interruptions in care when long appointment wait times occur. The program incorporates didactic content (Table 3) and hands-on treatment of conditions in the state that affect the lives of children, including prematurity, morbidity, vaccination rates, maternal health, postpartum depression screening, and complex and chronic physical and mental health problems. Incorporating behavioral and mental health training resulted in innovative interdisciplinary collaboration.
Between 20 and 30 PNPs apply to the fellowship from graduate primary care programs across the US in response to internet advertisements, targeted conference presentations and program director professional networking. Ideal candidates demonstrate interest caring for underserved pediatric populations, and a strong desire to enhance education and competency – especially in behavioral and mental health. They complete certification and credentialing requirements, which can take approximately 90 days, and enrollment in the program follows a typical academic cycle. Weekly schedules include 2 days in the primary care setting (termed ‘continuity clinic’) with a primary mentor (Fig1). One week day is dedicated to didactic learning, reflective and wellbeing practices and/or an evidence-based practice project. Specialty rotations include nurse practitioner mentor-guided learning in school-based health centers, inpatient services such as the well-baby nursery, neonatal intensive care unit, pre-surgery areas and orthopedics, allowing exposure and understanding of patient and family experiences.
The PNP primary care fellowship also has been financially viable with billed income equaling close to 100% of fellow salary, documenting sustainability22. Pediatric nurse practitioners are responsible for providing care for a full panel of patients on a graduated scale. Management of the program and time for education offered by providers employed by the hospital are not listed in the program costs.
Between July 2017 and October 2024, 10 graduates completed the PNP primary care fellowship program and eight (80%) remain engaged in clinical care in rural or medically underserved communities. The program originally hired two PNPs per year, but the COVID-19 pandemic resulted in the resignation of one fellow in 2019, a hold on the program for 2020 and 2021 and only one fellow hired in 2022. A federal US Health Resource & Services Administration (HRSA) grant obtained in 2023 allowed the opportunity to host additional fellows from across the country with program expansion.
Fellows provide care in primary care clinics and collaborate in mental health care with licensed psychologists available on site. The HRSA grant supports four PNP primary care graduates annually as well as employing targeted training in our community’s highest need areas: pediatric behavioral and mental health care, and rural health. In alignment with funding priorities, we are increasing training for telehealth and utilizing unique methods of education, focused on transition to practice in rural, urban or tribal underserved populations.
Table 2: Pediatric-specific nurse practitioner competencies for assessment of the pediatric nurse practitioner primary care fellowship program
| Competency | Evaluation† examples |
|---|---|
| Clinical competency in planning and managing care |
Differential diagnosis Medications Consults and referrals |
| Assess, diagnose, treat and manage over time common medical conditions experienced by pediatric patients in primary care |
Vaccination schedule Asthma Otitis media Pharyngitis Fever of unknown origin Eczema Attention deficit hyperactivity disorder Depression Anxiety Overweight and obesity |
| Leadership |
Lead case conferences Present patient problems |
| Interprofessional team collaboration |
Safely transition patients between services and providers Maintain open, respectful communication Seek feedback from faculty and team members |
| Patient-centered care |
Communicate with patients between visits using internet-based and telephone communication Elicit patient values, cultures and beliefs Empower patients for self-care Identify, accommodate and customize care based on cognition, language, functional and cultural barriers |
| Shared decision-making |
Active listening skills Engage patients and families as care team member Share accountability with other professions, patients and communities for preventative care |
| Sustained relationships |
Devise, follow, review and adjust longitudinal care plan to meet assigned patient healthcare needs Develop and sustain respectful and trusting relationships with peer trainees, program faculty, clinic staff and other interprofessional colleagues |
† Evaluation includes many more parameters. This list is not all-inclusive.
Table 3: Educational activities included in the first quarter of the pediatric nurse practitioner primary care fellowship program
| Topic | Area of concentration |
|---|---|
|
Icebreaker/team-building exercises Orientation to institutional wellbeing program Gaining trust and giving feedback Nemours wellness program Nemours mansion and garden exploration Walk with ‘Ali’, Nemours therapy dog Attend hospital-wide orientation DISC® profile and connecting DISC to developing a culture of trust Self-directed wellness activity Interprofessional spiritual care education Communicating across cultures Managing difficult encounters |
Wellness, team-building and communication activities |
|
Introduction to antibiotic stewardship Antibiotic stewardship: bugs and drugs Antibiotic stewardship: pediatric dosing pharmacokinetics Asthma care Human trafficking: raising awareness to identifying victims in the clinical settings Weekly pediatric grand rounds Trauma series: pediatric strangulation Addressing vaccine hesitancy Telehealth overview and best practices Introduction to social determinants of health Religious practices and preferences All things respiratory Bronchopulmonary dysplasia: history and current trends |
General pediatrics |
|
PNP case study planning Responding to psychologist case studies Program director rounding |
Interactive activities |
|
Introduction to evidence-based practice Quality improvement and evidence-based practice methods Research methods and example of research project Role of research nurse Nursing Research Council Collaborative Institutional Training Initiative (CITI online) Nurses’ role in recruiting and enrolling patients in research Literature critique, creating an evidence table Group discussion, individual project planning |
Evidence based practice and research |
| Library services, request and search for evidence in the library | Library services |
|
Gender-affirming care in the ambulatory setting Creating an adaptive care environment for vaccinations in children with autism Creating a hyperbilirubinemia pathway in the ED: A QI project example |
Examples of previous projects in ambulatory care Quality improvement projects and clinical pathways |
PNP, pediatric nurse practitioner. QI, quality improvement.
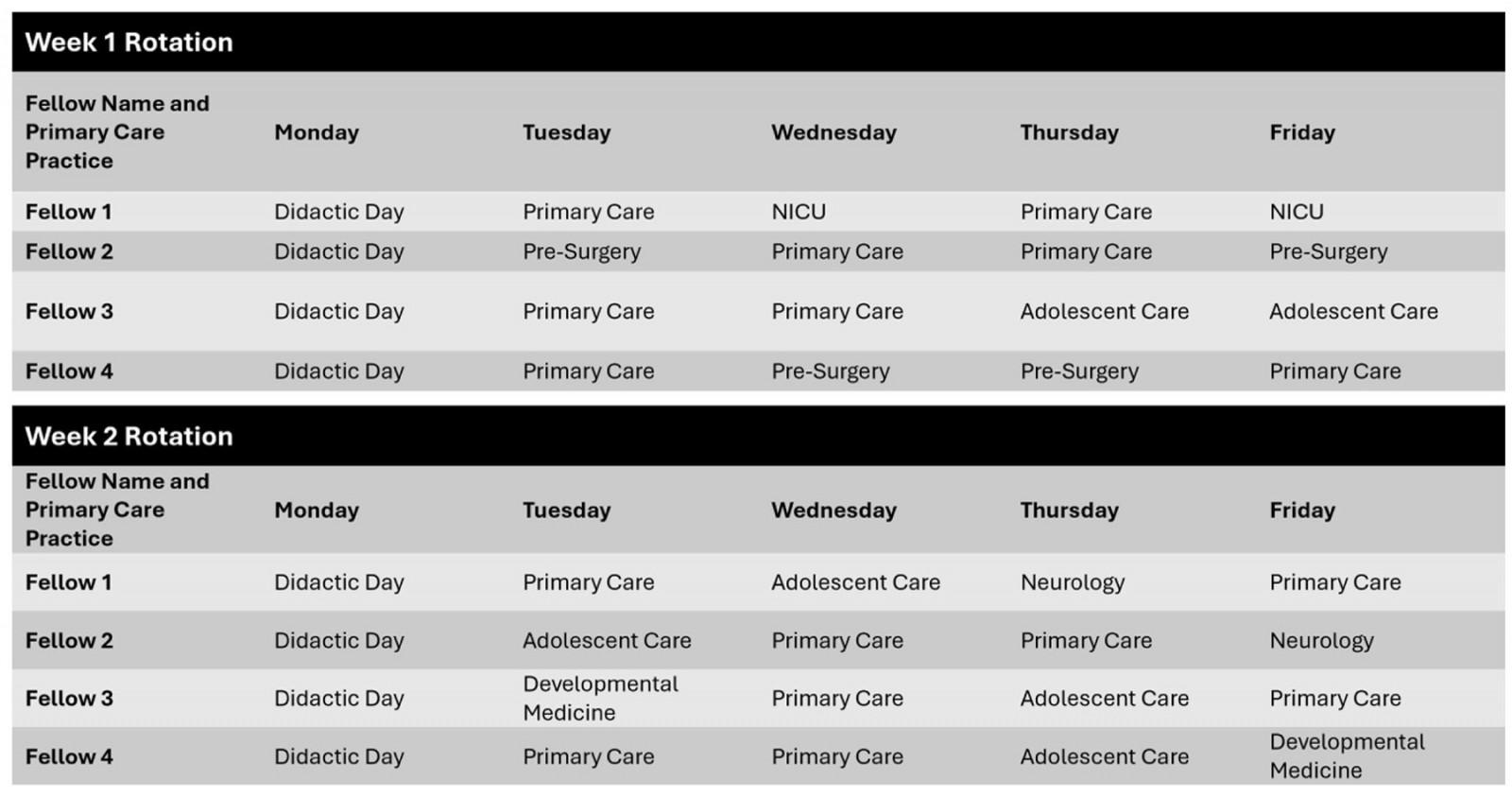 Figure 1: Example of the pediatric nurse practitioner primary care fellowship clinical rotation schedule.
Figure 1: Example of the pediatric nurse practitioner primary care fellowship clinical rotation schedule.
Supportive structures
Community partnerships
As the hospital is not in a university setting, there are collaborative relationships with local universities to incorporate extensive pediatric behavioral and mental health training and additional education not available in the pediatric hospital setting. Linking with a federally qualified health center located in a Healthcare Provider Shortage Area allows fellows to care for vulnerable and high-risk patients and families.
Mental health training
Behavioral and mental health services training provided by a psychologist partner offers fellows in-depth and extensive didactic including diagnosis, evaluation, screening tools and treatment, along with simulation experiences. A psychiatric mental health nurse practitioner adds education in pharmacological management of behavioral and mental health problems. Continuing education, collaboration and shadow opportunities with psychologists in primary care offices offer experiential education, especially noting that mental health and behavioral health care for providers is not consistent in US academic programs and nurse practitioner students are not always offered this experience clinically. With this education and clinical experience, nurse practitioners can now obtain additional credentials documenting training and competency29.
Wellbeing
The partner psychologist offers support in an objective environment, allowing fellows to voice concerns and issues they may be uncomfortable relaying to organizational leaders. However, it is essential that fellows initiate and maintain relationships with preceptors, the program director and other program liaisons. Previous experience as pediatric nurses prepared fellows with established skills to build successful patient and family relationships. In addition to regular meetings with the program psychologist, fellows meet regularly with the program director and develop friendships among their cohort. The fellows benefit from hospital-based wellbeing activities to support resilience and retention28.
Training in rural health and underserved populations
Rural health provision requires nurse practitioners to be independent, acknowledge emergent issues and manage challenging situations in primary care. Addressing specialty problems and stabilizing patients while awaiting appointments or transportation to higher levels of care is imperative. Management of behavioral and mental health problems can be accomplished by well-trained PNPs29. Education regarding social determinants of health allows nurse practitioners to address issues beyond the health needs of their patients. Nurse practitioners who live and work in their communities understand the challenges patients and their families face on a day-to-day basis3.
Additional benefits of working in US underserved and rural areas, to include Healthcare Provider Shortage Areas and a federally qualified health center, include working in a desirable location to live, tuition loan repayment, opportunity to independently manage a panel of patients and to gain specialty and complex patient experiences3. The PNP primary care fellowship incorporates clinical training in these sites but also didactic information about the rewards of choosing a career in a rural or underserved area.
Lessons learned
Program evaluation
Program aims to include documentation of PNP confidence and competence as program outcomes is an important goal, but meaningful analysis of data with small numbers of participants is challenging. Programmatic evaluation for this fellowship began in 2017 and currently occurs with fellows’ documentation of self-competency, confidence and employment status. Ten fellows have completed the program, and initial data indicate increased confidence and competency, especially in mental health care. Figure 2 includes data for these measures.
Long-term program evaluation includes tracking fellows who practice primary care in rural communities for 5 years post-training. Between July 2017 and October 2024, of the 10 graduates, eight (80%) remain engaged in clinical care in rural or medically underserved communities. Data are currently being collected through an institutional review board-approved interprofessional research project regarding clinical training with engaged psychologists.
Monitoring provider quality and success in line with patient outcomes and satisfaction, including quantitative information such as number of referrals and/or diagnostic testing with comparisons to providers who did not attend a PNP primary care fellowship, is ongoing. Other potential avenues for assessing training outcomes could compare compliance with pediatric primary standards of care among PNP primary care fellowship trainees, but any meaningful comparisons will be difficult until adequate numbers of trainees are achieved.
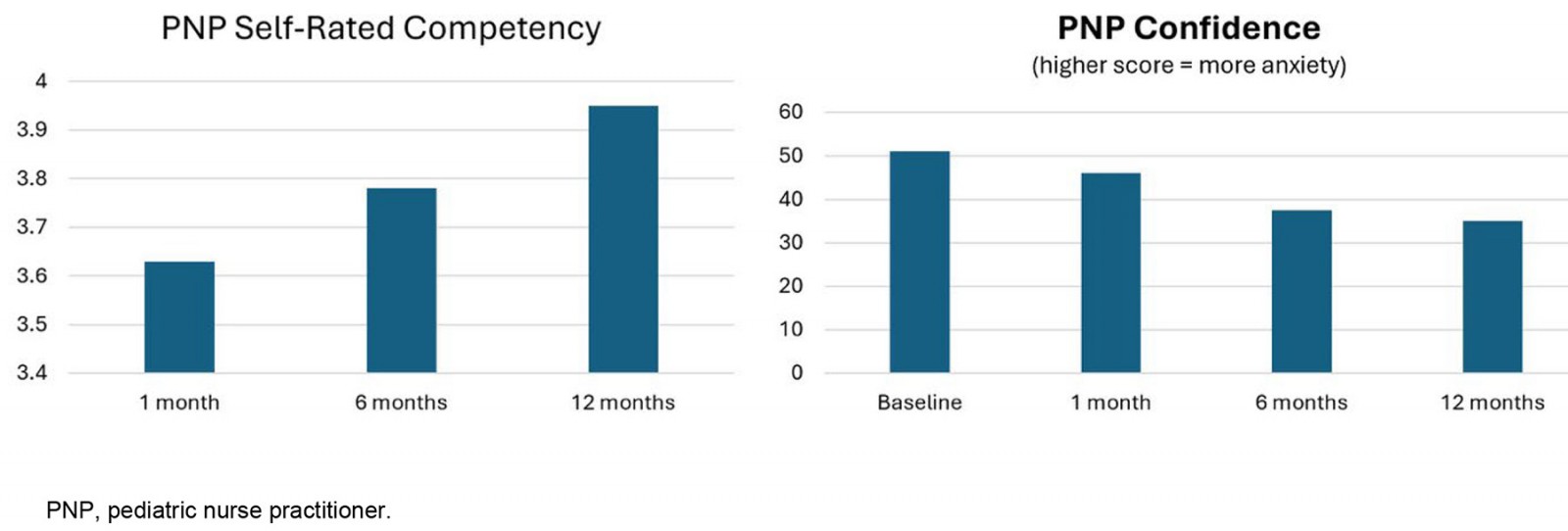 Figure 2: Initial data supporting the pediatric nurse practitioner primary care fellowship.
Figure 2: Initial data supporting the pediatric nurse practitioner primary care fellowship.
Organizational commitment
Developing and maintaining a PNP primary care fellowship involves a multitude of support services and institutional financial commitment for program director salary support, time for leaders to create curriculum, and administrative time to manage educational and clinical schedules and collaborative efforts between facilities. When this program launched in 2017, it demonstrated financial stability as fellows generated revenue through patient encounters, and now the HRSA grant allows further curriculum expansion and administrative support. The grant allowed us to create community partnerships with universities to provide simulated mental health trainings and with health systems, allowing for hands-on training for higher risk social needs populations. We have engaged a nurse scientist and evidence-based practice specialist within our organization to consult on data collection for quality improvement and research activities, and support outcome evaluation.
Challenges
Barriers to program implementation have included competing educational needs from other disciplines (ie residents, students), and lack of space and support staff for fellows within primary care settings. This PNP primary care fellowship advanced practice providers to offer lectures and host fellows in specialty practice; however, the cost of mentors’ non-clinical time is not counted but balanced by the opportunity to achieve professional and scholarly goals. Preceptors, office managers and staff are expected to maintain patient volumes, making ongoing engagement with a fellow challenging.
Growth opportunities
Next steps include ongoing refinement of the program curriculum based on feedback and nurse practitioner learning and community needs. Over time, through use of quantitative metrics, we hope to find statistically significant results in program outcomes, which include confidence and competency. Monitoring the financial sustainability of our program, including administrative support, is essential. Following fellow career paths and evaluating their retention in rural and underserved areas is another goal. Additionally, PNP primary care fellowship mentors have a unique role, and despite rewards including professional accomplishment, and potential clinical advancement, there is very little data regarding their roles in supporting transition to practice. Developing research around the evaluation and support of mentors associated with PNP primary care fellowship positive outcomes is a must, along with supporting their wellbeing and satisfaction.
Summary
Nurse practitioner fellowship programs continue to gain momentum in the US, but in pediatrics remain primarily within inpatient services and settings4. To provide a successful pipeline for transition to practice within this children’s hospital system, a PNP primary care fellowship program was initiated in 2017, training four fellows annually since 2023.
Initial data that informs program content, successful clinical experiences, satisfaction and wellbeing among attendees, and quality measures that document successful pediatric patient outcomes, is encouraging but ongoing. Transition-to-practice programs offer confidence for new nurse practitioners and can be key for those interested in providing comprehensive care for vulnerable populations in rural areas.
Acknowledgements
The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement by, the HRSA of the US Department of Health and Human Services, or the US Government. For more information, please visit HRSA.gov.
Funding
The fellowship program described in this article is supported by the HRSA of the US Department of Health and Human Services as part of an award totaling US$2,468,000.00 over 4 years with 70% supporting fellow salaries and benefits. The majority of program management is financed with non-governmental sources.
Conflicts of interest
The authors have no conflicts of interest to disclose.