




Introduction
In Australia, as globally, there are persistent challenges in maldistribution of health workforce1-4. While some metropolitan areas have an oversupply, rural regions consistently struggle with severe staff shortages, especially skilled and experienced staff5,6. This type of working environment exposes rural health professionals to the risk of professional isolation, increased stress and burnout, reducing their job satisfaction and increasing the likelihood that they leave their rural health role7-12. Excessive workloads lead to exhaustion and adversely impact work performance5,13,14. Although predictable, the high and rapid turnover in rural areas has crucially increased the cost of primary care and undermines stable, high-quality community healthcare services in rural communities11,15-18.
It is well known that rural health professionals have reduced access to continuing professional development (CPD) and often face additional time commitment, financial burden and logistical challenges when pursuing CPD compared to health professionals in cities19,20. However, CPD is crucial for health professionals, as it helps maintain and enhance professional knowledge, expertise and competence, and serves as an essential pathway to develop required personal and professional qualities throughout professional lives21. According to Cosgrave et al, beyond professional development opportunities, the quality of workplace relationships also significantly impacts job satisfaction among rural health professionals22. They face challenges in exchanging information and receiving peer support compared to urban health professionals due to the dispersed and small-scale nature of rural health practice. An earlier study demonstrated that helping rural GPs build support networks led to them seeking peer assistance for personal and professional challenges, reducing professional isolation and the number of GPs considering leaving rural practice in the short- and medium term23.
Digital technology is a highly promising strategy for improving rural health care24-28. During the COVID-19 pandemic, digital technologies demonstrated great potential globally to break through geographical barriers, infection risks and time constraints, providing more possibilities for real-time updates, communication, healthcare services and education29,30. This highlighted the potential of digital technology to provide greater support and resilience for vulnerable and isolated groups30. This is evident not only in telehealth services for rural patients but also in offering continual updates, information and educational support for rural health professionals29,31-33. Current digital tools have changed the context of supporting rural health professionals34. Education, training and CPD can be delivered through webinars, virtual simulation training, online modules, professional forums and online resource databases. This decreases the costs and obstacles to accessing expertise for rural health professionals35-41.
Digital platforms facilitate the flow of knowledge42,43 and allow health professionals from diverse backgrounds to freely join online professional communities based on shared interests, and engage in meaningful exchange and collaboration not constrained by distance and professional status44,45. However, concerns remain about the lack of social interaction in online learning and disparate levels of digital literacy38,46, which exacerbates disparities in digital divide and access to digital resources, despite higher needs in rural areas47. Limited access to digital technology and poorer internet connectivity impact critical communication and information channels, impacting staff capability to perform their jobs30,48. Additionally, professionals face the challenge of filtering and evaluating online information due to the abundance of resources, with varying accuracy, currency and credibility38,49. Also, online resources are not often tailored to the rural health setting or rural health professional50.
Given these barriers, targeted support and information tailored to their unique needs is essential. However, research on the experience and usage of digital platforms by rural health professionals remains limited. A deeper understanding of diverse users' needs may help identify strengths and weaknesses in existing features and provide empirical evidence for continual platform optimisation and improvement.
This study aimed to investigate rural health professionals’ usage patterns and experiences with a digital support platform, identifying factors associated with usage and likelihood of recommending it to colleagues. It also aimed to gain a deeper understanding of how an online platform can better support rural health professionals to address existing gaps and guide future improvements.
Methods
Rural Health Pro
Rural Health Pro is a social enterprise of RDN – The Charity for Health Access. RDN is a health and social care access charity group established in 1988 that develops and manages social enterprises centred on achieving the vision of ‘health and social care access for all’51. To better support rural health professionals, RDN has embraced digital innovation, with Rural Health Pro emerging as a key initiative in this effort.
This digital platform, available to health professionals throughout Australia and beyond, offers free membership, with news, resources, discussions, jobs, training resources, funding opportunities and digital events51. Users can browse tailored rural health content and follow people, organisations, topics and groups based on their availability, location, profession, needs and interests. Further customisable email and mobile alerts help keep members informed. The platform filters content by location, profession and other relevant parameters. The Rural Health Pro mobile app makes content accessible when and where rural health professionals need it, which is especially important for those on the move around their community or hospital.
The main features of the Rural Health Pro platform include:
-
professional development and learning:
- live webinars, conferences and events
- a rural health training calendar that aggregates education and training opportunities from various organisations
- an expanding library of resources from industry organisations
- on-demand videos including training, webinars and interviews with rural health professionals
-
community and networking:
- Rural Health Pro special interest groups, which aim to bring people together with shared interests, such as in chronic disease or Aboriginal and Torres Strait Islander health. Users can personalise their feeds by following other members and topics, and joining groups of interest
- discussion boards on various featured and trending topics (eg type 2 diabetes and Aboriginal and Torres Strait Islander health)
-
career and support opportunities:
- information on current grants, scholarships and funding opportunities from universities, organisations and government departments that promote rural health
- rural vacancies for doctors, nurses, midwives and allied health practitioners.
Rural Health Pro aims to provide a networking platform for health professionals and organisations committed to improving rural health, enabling them to have more opportunities to connect, share experiences and exchange expertise. In addition to curating targeted training, educational resources, employment opportunities and financial support, the platform facilitates group discussions, bringing together professionals with shared interests to encourage dialogue and mutual support. This aims to expand their personal and professional networks and enhance their capabilities in rural daily work and life51.
Google Analytics backend data from Rural Health Pro from 2022 to 2023 shows 16,467 users accessed the platform, with 44,408 unique page views and an average 4-minute session duration in 2022. In 2023, 9566 users accessed the platform, with 26,233 unique page views and an average 5-minute session duration. In 2025, the platform backend data shows that Fridays are the most active days, with peak activity in the early afternoon. The top three hourly activity periods are around 1 pm, 11 am and 2 pm, suggesting users may access the platform shortly after receiving the weekly newsletter on Fridays.
Rural Health Pro’s video hosting platform received 2990 views from 925 unique viewers between 5 November 2020 and 31 December 2023. The average viewing duration was around 44% of the video length.
 Figure 1: Rural Health Pro web home page screenshot.
Figure 1: Rural Health Pro web home page screenshot.
 Figure 2: Rural Health Pro mobile application home page screenshot.
Figure 2: Rural Health Pro mobile application home page screenshot.
Data source
The data for this study were obtained from three cross-sectional online surveys conducted by RDN in 2020/2021, 2021/2022 and 2023. Each year, RDN distributes online surveys to registered members on the Rural Health Pro platform to evaluate its functionality, content, usage and impact. Health professionals can register to become Rural Health Pro members through the Rural Health Pro home page. By providing their contact details (eg email address, phone number, name), users can set up a Rural Health Pro account and gain access to the platform.
The online research survey link was posted on the Rural Health Pro home page, promoted through social media and the weekly newsletter to up to 6353 members. Between 2020 and 2023, the online survey link was distributed along with a participant information sheet and consent form embedded in the survey. In addition to the emails, the survey was promoted on the Rural Health Pro website and through social media. The surveys remained open for up to 2 months, with voluntary participation encouraged. Due to the lack of unique identification numbers, some members may have completed the survey multiple times as separate respondents, since it is an annual survey sent to all users. After excluding missing data for selected outcome variables, 186 responses were included for analysis in this study.
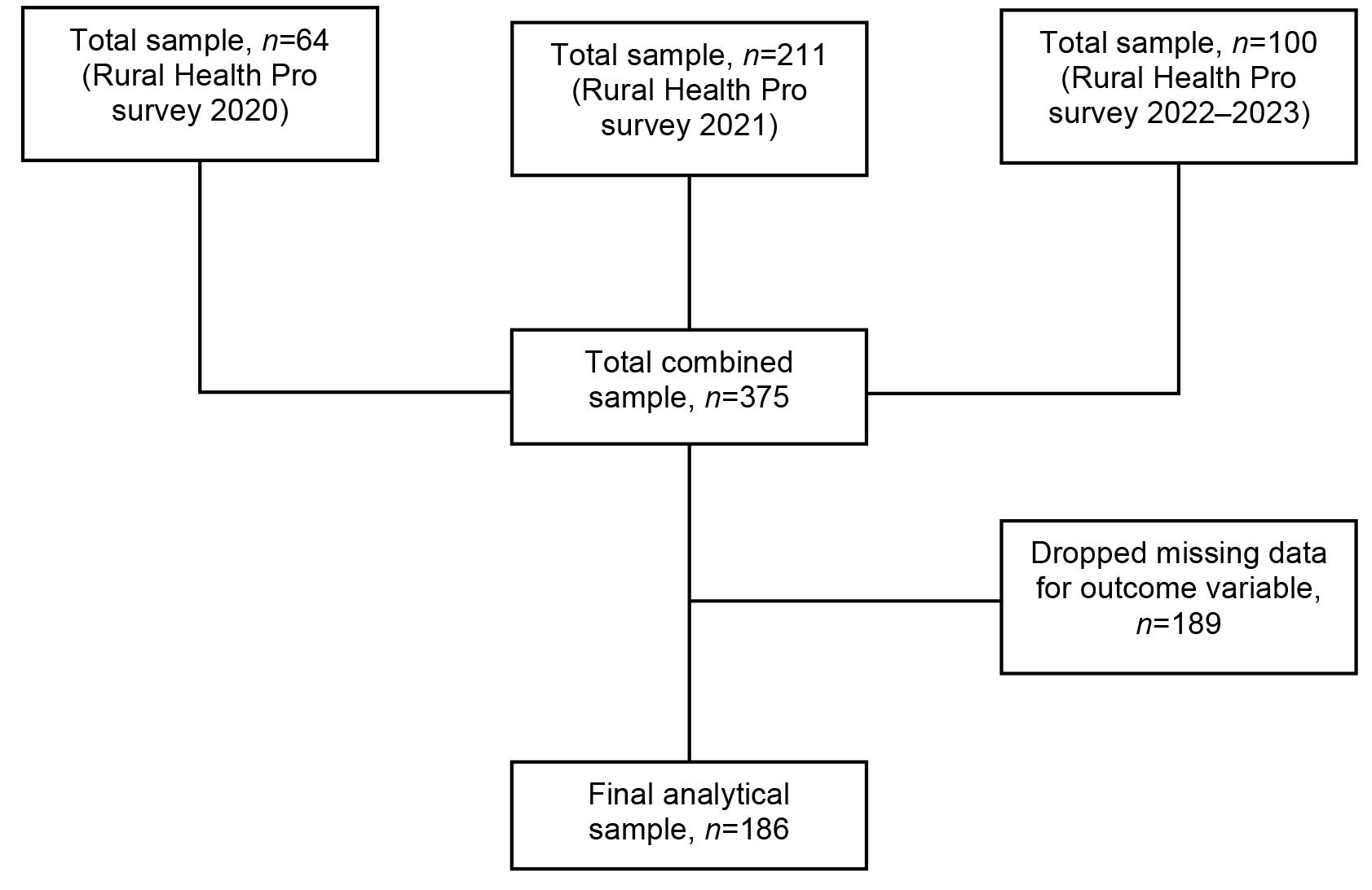 Figure 3: Selection process of the analytical sample.
Figure 3: Selection process of the analytical sample.
Measures
Outcome measures
This study considered usage frequency and health professionals’ likelihood of recommending Rural Health Pro as the two outcome variables.
Rural Health Pro usage frequency
Health professionals’ usage of Rural Health Pro was selected as the first outcome variable in this study. Respondents were asked, ‘On average, how often do you log into Rural Health Pro?’, with answer options ranging from ‘twice or more per week’, ‘twice or more each week’, ‘approximately twice per month’, ‘monthly’, ‘approximately every two months’, ‘approximately every three months’, to ‘once only per year.’ For analytical purposes, a binary variable, ‘usage frequency’, was created from these responses. Those who selected ‘twice or more per week’, ‘twice or more each week’, ‘approximately twice per month’ or ‘monthly’ were classified as frequent users (coded as 1), while those who chose ‘approximately every two months’, ‘approximately every three months’ or ‘once only per year’ were classified as non-frequent users (coded as 0).
Likelihood of recommending Rural Health Pro
The net promoter score (NPS) was chosen as the second outcome variable to assess health professionals' likelihood of recommending Rural Health Pro to colleagues and to infer participants’ experiences and satisfaction with Rural Health Pro. NPS was frequently utilised to assess patients' experiences with health care and the satisfaction of and likelihood of recommending various interventions and programs52-57. In this study, participants responded to the question, ‘How likely are you to recommend Rural Health Pro to a colleague?’, rated on a 10-point Likert scale, where 0 indicated ‘very unlikely’ and 10 indicated ‘highly likely’. For analytical purpose, in this study, we categorised the responses into three groups: ‘detractor’ (scores 0–6), ‘passive’ (scores 7 and 8) and ‘promoter’ (scores 9 and 10). For analytical purposes, a binary variable called ‘likelihood of recommendation’ was created from these categories. Participants classified as ‘detractor’ were coded as 0, while those classified as ‘passive’ and ‘promoter’ were both labelled as ‘promoter’ (coded as 1).
Independent measures
Rural Health Pro usage pattern
Rural Health Pro usage patterns were also measured through content and device access. Participants were asked which content they accessed, responding to the question, ‘In an average month, which of the following areas do you access on Rural Health Pro?’ Multiple content options could be selected. The following eight content areas were included in this study: webinars, training calendars, discussion boards, special interest groups, resource library, on-demand videos, jobs, and grants and funding. For research purposes, these content areas were categorised into three sections, professional development and learning (webinars, training calendar, resource library and on-demand videos), community and networking (discussion boards and special interest groups) and career and support opportunities (jobs, grants and funding).
Participants who had not accessed any content in a section were labelled as ‘no’ and coded as 0. Those who accessed at least one content item in a section were labelled as ‘yes’ and coded as 1. Additionally, participants were asked what type of device they used to access Rural Health Pro. The responses were categorised as ‘desktop’, ‘handheld device’ (including mobile phone browser, Rural Health Pro App and tablet or iPad), or ‘both’ (both desktop and handheld devices).
Sociodemographic characteristics
In this study, the following variables were included as potential covariates related to Rural Health Pro usage frequency and likelihood of recommendation.
Gender
Gender variables were female, male or non-binary.
Age
Age variables were the age groups of 18–39 years, 40–59 years and over 60 years.
Type of health profession
Variables for type of health profession were allied health (eg Aboriginal Health Worker, speech pathologist, pharmacy), medical (eg GP and nurse), non-medical (eg researcher, health administrator, practice manager) and student.
Education
Education variables were certificate or less (eg HSC, Certificate III), undergraduate (eg bachelor, diploma) and postgraduate (eg Master's degree, graduate certificate/diploma, medical doctor, PhD)
Self-reported capability
The study assessed self-reported capability using the question, ‘Acknowledging that on different days we all feel more or less on top of our working and personal lives, over the last 4 weeks, how would you describe your overall level of capability in fulfilling your healthcare role?’ Participants rated their capability on a 10-point Likert scale ranging from 0 (‘not capable’) to 10 (‘fully capable’). For analysis purposes, a new variable called 'self-reported capability' was created from the responses. Scores from 0 to 5 were categorised as 'less capable' (coded as 1), while scores from 6 to 10 were classified as 'more capable' (coded as 2).
Statistical analyses
First, descriptive statistics were used to summarise the health professionals’ sociodemographic characteristics, usage patterns, usage frequency and the likelihood of recommending Rural Health Pro. Following this, bivariate analyses were conducted to examine the variables and their distributions across the outcome variables (Rural Health Pro usage frequency and the likelihood of recommending Rural Health Pro). We conducted logistic models to identify the determinants of each outcome variable. Variables that yielded p<0.05 in the bivariate analysis were included in each adjusted model. The results of the logistic regression analyses are presented as odds ratios, accompanied by the corresponding 95% confidence intervals (CIs) and p-values.
Several diagnostic tests were carried out to assess the assumptions of the logistic model, including McFadden’s R2 and the Hosmer–Lemeshow test to evaluate model performance, as well as variance inflation factor (VIF) statistics to identify multicollinearity among predictor variables. The significance level was set at 0.05. All analyses were conducted using the Statistical Package for the Social Sciences v29.0.2.0 (IBM Corp; https://www.ibm.com/products/spss-statistics).
Ethics approval
Ethics approval was received from the Deakin University Health Ethics Advisory Group (HEAG-H 195_2020: Evaluating Rural Health Pro – A web platform to support rural health professionals).
Results
Sociodemographic characteristics of respondents
Table 1 shows the demographic characteristics of the Rural Health Pro survey participants. The study included a total of 186 health professionals, with over 71% (132/186) being female. Half of the participants were in the age range of 40–59 years (50%, 93/186), followed by 32.3% (60/186) aged between 18 and 39 years and 17.7% (33/186) aged over 60 years. Most participants were medical professionals (31.7%, 59/186), followed by allied health (30.1%, 56/186), non-medical professionals (29.0%, 54/186) and students (9.1%, 17/186). Over half of the participants had completed postgraduate education (56.5%, 105/186), while 37.1% (69/186) had undergraduate education. Only 6.5% (12/186) of participants held certificates, high school or below. Among the 173 participants (93%, 173/186) who self-reported their capability, 79.8% (138/173) felt they had high capability in fulfilling their healthcare role. The professional development and learning section is the most commonly accessed content on Rural Health Pro (73.7%, 137/186). Additionally, the community and networking section is of significant interest (43.0%, 80/186), followed by the career and support opportunities section (39.0%, 64/164). Regarding device usage, 86.0% (160/186) of participants provided information about their access device. The majority used desktop devices (58.8%, 94/160), followed by handheld devices (22.5%, 36/160, including mobile phones, tablets and the Rural Health Pro application), with 18.8% (30/160) using both types of device.
Table 1: Demographic characteristics of Rural Pro survey respondents (N=186)
| Characteristic | n | % | |
|---|---|---|---|
| Gender | Female | 132 | 71.0 |
| Male |
53 |
28.5 | |
| Non-binary |
1 |
0.5 | |
| Age (years) | 18–39 | 60 | 32.3 |
| 40–59 |
93 |
50.0 | |
| ≥60 |
33 |
17.7 | |
| Profession | Medical | 59 | 31.7 |
| Allied health |
56 |
30.1 | |
| Non-medical roles |
54 |
29.0 | |
| Student |
17 |
9.1 | |
| Education | Postgraduate | 105 | 56.5 |
| Undergraduate |
69 |
37.1 | |
| Certificate, high school or less |
12 |
6.5 | |
| Self-reported capability | Low capability | 35 | 18.8 |
| High capability |
138 |
74.2 | |
| Missing |
13 |
7.0 | |
| Accessed professional development and learning | No | 49 | 26.3 |
| Yes |
137 |
73.7 | |
| Accessed community and networking | No | 106 | 57.0 |
| Yes |
80 |
43.0 | |
| Accessed career and support opportunity | No | 104 | 55.9 |
| Yes |
60 |
32.3 | |
| Missing |
22 |
11.8 | |
| Access device | Desktop | 94 | 50.5 |
| Handheld device |
36 |
19.4 | |
| Both |
30 |
16.1 | |
| Missing |
26 |
14.0 |
Rural Health Pro usage pattern and likelihood of recommendation
As shown in Table 2, the majority frequently log in to use Rural Health Pro (60.2%, 112/186) and a significant number of health professionals (71%, 132/186) reported a likelihood of recommending Rural Health Pro to their colleagues, which infers a positive experience with the platform.
The results of bivariate analysis (Table 3) show that factors such as age (p=0.007), access to the professional development and learning section (p<0.001), access to the community and networking section (p<0.001), and access to the career and support opportunity section (p=0.005) were found to be significantly associated with health professionals' frequency of using Rural Health Pro. Based on the multivariate analysis (Table 3), model 1 shows that health professionals aged 40–59 years (odds ratio (OR): 2.360, 95%CI: 1.060–5.256), accessed the professional development and learning section (OR: 3.973, 95%CI: 1.802–8.757), the career and support opportunity section (OR: 2.258, 95%CI: 1.043–4.886) and the community and networking section (OR: 3.867, 95%CI: 1.810–8.264) were significantly more likely to report frequent usage of Rural Health Pro.
Table 4 shows the bivariate and multivariate analysis between several factors, including usage of Rural Health Pro and health professionals' likelihood of recommending Rural Health Pro. In the bivariate analysis, the following factors were found to be significantly associated: age (p=0.002), education (p=0.045), self-reported capability (p<0.001), access to the professional development and learning section (p<0.001), access to the career and support opportunity section (p<0.001) and usage frequency (p<0.001).
Compared to model 1, no significant association was found between accessing the community and networking section, age and health professionals’ likelihood of recommending Rural Health Pro to their colleagues in model 2. Those who accessed the professional development and learning section (OR: 3.188, 95%CI: 1.157–8.788) or the career and support opportunity section (OR: 3.013, 95%CI: 1.032–8.795) were found to be more disposed to recommending Rural Health Pro to their colleagues. Additionally, model 2 showed that health professionals who reported higher self-perceived capability were 11.382 times more likely to express a desire to recommend Rural Health Pro to their colleagues (95%CI: 3.418–37.903) compared to those who reported lower capability levels. Health professionals who used Rural Health Pro more frequently were 6.904 times more likely to recommend it to their colleagues than those who used it less frequently (95%CI: 2.507–19.013).
Moreover, the findings revealed that health professionals with an undergraduate education level were more likely to recommend Rural Health Pro to their colleagues compared to those with a postgraduate education level (OR: 4.054, 95%CI: 1.233–13.324).
The McFadden’s R2 values of both models indicated good model fit (model 1: R2=0.189; model 2: R2=0.378), supported by the non-significant Hosmer–Lemeshow goodness-of-fit statistics (model 1: p=0.135; model 2: p=0.616). The VIF test yielded mean values of 1.014 and 1.064, confirming the absence of multicollinearity in both models.
Table 2: Usage and likelihood of recommendation of Rural Health Pro (N=186)
| Characteristic | Variable | n | % |
|---|---|---|---|
| Usage frequency | Non-frequent user | 74 | 39.8 |
| Frequent user |
112 |
60.2 | |
| Likelihood of recommendation | Detractor | 54 | 29.0 |
| Promoter |
132 |
71.0 |
Table 3: Model 1: Factors associated with Rural Health Pro usage, including both bivariate and multivariate estimates
| Characteristic | Variables | Non-frequent user (%) | Frequent user (%) | χ2 (p-value) | OR | 95%CI | VIF |
|---|---|---|---|---|---|---|---|
| Gender | Female | 58 (43.9) | 74 (56.1) | 3.649 (0.161) | – | – | |
| Male |
16 (30.2) |
37 (69.8) | |||||
| Non-binary |
0 (0.0) |
1 (100.0) | |||||
| Age (years) | 18–39 | 28 (46.7) | 32 (53.3) | 10.034 (0.007) | Reference | Reference | 1.009 |
| 40–59 |
27 (29.0) |
66 (71.0) | 2.360** | 1.060–5.256 | |||
| ≥60 |
19 (57.6) |
14 (42.4) | 0.881 | 0.322–2.412 | |||
| Profession | Medical | 29 (49.2) | 30 (50.8) | 4.690 (0.052) | – | – | – |
| Allied health |
22 (39.3) |
34 (60.7) | |||||
| Non-medical |
14 (25.9) |
40 (74.1) | |||||
| Student |
9 (52.9) |
8 (47.1) | |||||
| Education | Postgraduate | 44 (41.9) | 61 (58.1) | 3.119 (0.210) | – | – | |
| Undergraduate |
23 (33.3) |
46 (66.7) | |||||
| Less than certificate |
7 (58.3) |
5 (41.7) | |||||
| Self-reported capability | Low | 17 (48.6) | 18 (51.4) | 2.263 (0.132) | – | – | – |
| High |
48 (34.8) |
90 (65.2) | |||||
| Access device type | Desktop | 41 (43.6) | 53 (56.4) | 1.114 (0.573) | – | – | – |
| Handheld |
16 (44.4) |
20 (55.6) | |||||
| Both |
10 (33.3) |
20 (66.7) | |||||
| Accessed professional development | No | 33 (67.3) | 16 (32.7) | 21.095 (<0.001) | Reference | Reference | 1.006 |
| Yes |
41 (29.9) |
96 (70.1) | 3.973*** | 1.802–8.757 | |||
| Accessed community and networking | No | 56 (52.8) | 50 (47.2) | 17.507 (<0.001) | Reference | Reference | 1.022 |
| Yes |
18 (22.5) |
62 (77.5) | 3.867*** | 1.810–8.264 | |||
| Accessed career and support opportunities | No | 53 (51.0) | 51 (49.0) | 7.963 (0.005) | Reference | Reference | 1.017 |
| Yes |
17 (28.3) |
43 (71.7) | 2.258* | 1.043–4.886 | |||
| Model statistics | McFadden’s R2 (%) | – | – | ||||
| Hosmer–Lemeshow test (p-value) |
– |
– | 11.087 (0.135) | ||||
| Mean VIF |
– |
– | 1.014 |
*p<0.05, **p<0.01, ***p<0.001
CI, confidence interval. OR, odds ratio. VIF, variance inflation factor.
Table 4: Model 2: Factors associated with Rural Health Pro likelihood of recommendations, including both bivariate and multivariate estimates
| Characteristic | Variables | Detractor (%) | Promoter (%) | χ2 (p-value) | Multivariate estimates | ||
|---|---|---|---|---|---|---|---|
|
OR |
95%CI |
VIF | |||||
| Gender | Male | 14 (30.3) | 39 (69.7) | 0.689 (0.709) | – | – | – |
| Female |
40 (26.4) |
92 (73.6) | |||||
| Non-binary |
0 (0.0) |
1 (100.0) | |||||
| Age (years) | 18–39 | 21 (35.0) | 39 (65.0) | 12.317 (0.002) | Reference | Reference | 1.046 |
| 40–59 |
17 (18.3) |
76 (81.7) | 2.761 | 0.893–8.534 | |||
| ≥60 |
16 (48.5) |
17 (51.5) | 1.211 | 0.336–4.365 | |||
| Profession | Medical | 22 (37.3) | 37 (62.7) | 4.898 (0.179) | – | – | – |
| Allied health |
17 (30.4) |
39 (69.6) | |||||
| Non-medical |
10 (18.5) |
44 (81.5) | |||||
| Student |
5 (29.4) |
12 (70.6) | |||||
| Education | Postgraduate | 38 (36.2) | 67 (63.8) | 6.185 (0.045) | Reference | Reference | 1.066 |
| Undergraduate |
13 (18.8) |
56 (81.2) | 4.054* | 1.233–13.324 | |||
| Less than certificate |
3 (25.0) |
9 (75.0) | 3.870 | 0.660–22.677 | |||
| Self-reported capability | Low | 21 (60.0) | 14 (40.0) | 20.650 (<0.001) | Reference | Reference | 1.105 |
| High |
29 (21.0) |
109 (79.0) | 11.382*** | 3.418–37.903 | |||
| Access device type | Desktop | 24 (25.5) | 70 (74.5) | 4.558 (0.102) | – | – | – |
| Handheld |
15 (41.7) |
21 (58.3) | |||||
| Both |
6 (20.0) |
24 (80.0) | |||||
| Accessed professional development | No | 25 (51.0) | 24 (49.0) | 15.611 (<0.001) | Reference | Reference | 1.065 |
| Yes |
29 (21.2) |
108 (78.8) | 3.188*** | 1.157–8.788 | |||
| Accessed community and networking | No | 36 (34.0) | 70 (66.0) | 2.907 (0.088) | – | – | – |
| Yes |
18 (22.5) |
62 (77.5) | |||||
| Accessed career and support opportunities | No | 40 (38.5) | 64 (61.5) | 11.605 (<0.001) | Reference | Reference | 1.027 |
| Yes |
8 (13.3) |
52 (86.7) | 3.013*** | 1.032–8.795 | |||
| Usage | Non-frequent | 39 (52.7) | 35 (47.3) | 33.419 (<0.001) | Reference | Reference | 1.077 |
| Frequent |
15 (13.4) |
97 (86.6) | 6.904*** | 2.507–19.013 | |||
| Model statistics | McFadden’s R2 (%) | – | – | 0.378 | |||
| Hosmer–Lemeshow test (p-value) |
– |
– | 6.279 (0.616) | ||||
| Mean VIF |
– |
– | 1.064 | ||||
*p<0.05, **p<0.01, ***p<0.001
CI, confidence interval. OR, odds ratio. VIF, variance inflation factor.
Discussion
Our study examined the usage and likelihood of recommending the Rural Health Pro to other rural health professionals and identified factors predicting these patterns. The results showed that 60.2% of respondents frequently used the platform, and 71% were likely to recommend it to their colleagues. Age, access to professional development and learning, career and support opportunities and community and networking content were found to be significantly associated with higher use of the platform in the multivariate model. Education level, access to professional development and learning, career and support opportunities, content and self-reported higher capability were factors significantly associated with a higher likelihood of recommending the platform.
There is also a significant association between health professionals’ usage and their likelihood to recommend the Rural Health Pro to their colleagues. This may suggest that compared to less frequent health professional users, high-frequency users tend to explore and engage with the platform's content and features more deeply. Davis defined perceived usefulness as ‘the degree to which a person believes that using a particular system would enhance his or her job performance’58. High-frequency users of Rural Health Pro may experience significant usefulness during their interactions with the platform and derive benefits in their daily work. Consequently, they are more inclined to recommend the platform to their colleagues.
Health professional characteristics
Age
Previous research indicated that younger rural health professionals generally prefer online educational resources more than their older colleagues20. Our study showed that health professionals aged 40–59 years used Rural Health Pro with higher frequency than other age groups. Young people frequently pursue travel opportunities, seek novel experiences, expand their professional networks or return to their hometowns for career development, which are choices that contrast with the relative stability characteristic of middle age22,59. As demonstrated in a study by Mu of Australian GPs' location decisions, younger GPs had a greater likelihood of working in rural areas compared to older GPs but also exhibited higher mobility60. Consequently, engaging with information focused on rural health may not be a priority for this younger age group, as they may focus more on exploring diverse career pathways. In contrast, middle-aged rural health professionals typically have achieved occupational and environmental ‘fitting in’, having established stronger self-identification within their local communities or have their sense of belonging (eg marriage and children at home)5,22,61. This stability may translate into a greater inclination to explore local professional resources. Rural Health Pro, with its focus on rural health, may appear to align more closely with the needs of these middle-aged professionals who have established career goals in rural areas, supporting their ongoing professional development and daily clinical practice.
A study by Cosgrave et al demonstrated that rural health professionals often develop intentions to leave their positions early in their careers, particularly during the initial and ongoing adaptation phases (typically within 12–18 months)22. This tendency may be established even earlier among inexperienced, non-local young health professionals who face higher professional challenges. To address this concern, the platform could implement a 'before stage' section that provides pre-employment information about the local social environment and lifestyle in rural areas. This resource would benefit both incoming health professionals and those preparing for onboarding, to enhance their personal satisfaction and provide a sense of belonging while facilitating a smoother transition through ‘fitting in’ community support62-64.
Education
Our study also found that health professionals with undergraduate degrees were more likely to recommend Rural Health Pro to colleagues compared to those with postgraduate qualifications. This pattern suggests that the platform's content may better align with the needs of undergraduate-level rural health professionals. Health professionals with advanced education experience typically may require more specialised academic resources to support evidence-based practice, such as peer-reviewed literature, pharmaceutical databases and online textbooks65. This finding highlights platform users' diverse educational backgrounds and varying informational needs. Future platform development should consider implementing a tiered content structure that accommodates different levels of resources to better serve rural health professionals’ diverse needs.
Capability
Our results showed there is no significant difference in the usage of Rural Health Pro between health professionals who self-reported as more capable and those who reported as less capable. However, there is a significant association between health professionals’ self-reported capability and the likelihood they will recommend the platforms to their colleagues. The study showed that 74.2% of those who referred Rural Health Pro to peers identified themselves as having 'high capability ' rather than 'low capability'. This may suggest that health professionals who self-reported as being more capable are more likely to find the content they need or that supports them, as well as to recognise the benefits and values it brings during their browsing of Rural Health Pro. They may be more adept at transforming these resources into personal knowledge or applying them to their daily work and life, which, in turn, leads to higher levels of recognition and satisfaction with the platform. Their higher willingness to recommend Rural Health Pro to colleagues could also reflect the professional maturity of more capable health professionals, as they transition from not only focusing on developing their own skills but also to ‘mentoring’ their colleagues. The capability approach, developed by Amartya Sen, conceptualises an individual's potential to achieve enhanced wellbeing and quality of life66. Within this framework, capability is defined as the ability to function effectively in complex, unfamiliar environments. This theoretical lens helps explain how, even in geographically disadvantaged rural settings with limited professional development opportunities, health professionals with high capability may actively seek out and effectively grasp resources (eg Rural Health Pro) for self-improvement, leading to more positive outcomes. This dynamic demonstrates that health professionals with higher capability may be better positioned to create a virtuous cycle between self-enhancement and platform satisfaction.
Content access
Professional development
Our study found access to professional development content on Rural Health Pro as a key factor motivating rural health professionals to frequently use the platform and more likely to recommend it to their colleagues. This finding aligns with existing research demonstrating that rural health professionals highly value CPD and exhibit strong learning motivation20,67. Our finding indicates that online training/education emerges as a practical solution to CPD access challenges for rural health professionals, offering flexibility and accessibility.
We hypothesise that the calendar-based presentation on Rural Health Pro is a significant factor in driving frequent visits and referrals. This feature enables health professionals to strategically plan their training programs and upcoming events by considering their individual schedules, areas of interest and preferred engagement modes (online/offline, geographic location). As Milligan and Littlejohn demonstrate68, scheduling tools provide valuable support for learners developing time management skills, thereby enhancing their overall learning experience. The Rural Health Pro online resources library offers health professionals the flexibility to manage their learning time according to their own schedule rather than fixed online courses; they can select from diverse course content and reinforce understanding through repeated learning. A study by Maloney et al, examining health professional learners' engagement with the online repository Physeek69, found that learners identified online repositories as their most efficient and preferred method for accessing expertise. Compared to mainstream search engines like Google, specialised digital platforms like Rural Health Pro significantly reduce the time spent filtering through redundant information, enabling users to efficiently acquire targeted knowledge and skills. Furthermore, when users can verify the credibility of resource origins (such as authoritative academic institutions, universities or evidence-based medical resources), their confidence in utilising these materials substantially increases69. Access costs emerge as another critical factor in providing resource support to rural health professionals. Research demonstrates that free access to health information and resources is associated with significantly higher utilisation rates70. This emphasis on reducing access barriers holds particular relevance in the context of already resource-constrained rural healthcare settings. Additionally, Rural Health Pro integrates rural health resources in various formats (eg video and text), which may reduce access barriers for rural health professionals with limited internet connectivity or time (eg choose the best suited to their current broadband conditions). The potential of this flexible, multi-format approach can be explored further in the future.
Community and networking
While in-person CPD events serve to enhance rural health professionals’ abilities, they also play a crucial role in helping health professionals establish regional professional networks, thereby reducing professional isolation and fostering a sense of belonging71. Consequently, when implementing online-based training, it becomes important to facilitate the development and engagement of vigorous community of practice. Our study revealed a significant positive association between access to the community and networking section and frequency of Rural Health Pro usage, potentially indicating users' desire to shape new professional connections through active engagement. However, this social engagement did not translate into increased platform recommendations among their colleagues, suggesting that the quality of interactions and social experiences within the current community may not yet meet health professionals' expectations.
A virtual community of practice is an internet-based platform that connects individuals sharing common interests or professional passions, facilitating both synchronous and asynchronous knowledge exchange72. Our study results suggest challenges in maintaining sustained engagement within the Rural Health Pro special interest groups and discussion boards. According to Jiménez-Zarco et al, virtual community of practice user satisfaction stems from two primary factors: the community's effectiveness and users' perceived usefulness73. While high access rates to the special interest groups and discussion boards indicate strong interest and expectations for online communication among rural health professionals, learner engagement can be significantly impaired by ineffective communication support (such as poor information quality, comprehension difficulties or lack of response) or barriers to initiating dialogue (including varying learning preferences, platform limitations and time constraints)68.
Agrawal and Joshi emphasised that a robust identification within a community of practice and active member engagement are crucial elements for successful community of practice operation74. To maintain the virtual community of practice’s continued vitality, the real challenge is to encourage members to voluntarily and continually help one another through ongoing knowledge-sharing, fostering the development of a virtuous cycle of mutual support and symbiosis73. To achieve this goal, having a sponsor to endorse the virtual community of practice, followed by a leader to drive the community, could be a strong starting point. Implementing specific facilitation roles may further motivate community members to collaborate actively. These might include appointing a facilitator by the originators of the community or nurturing spontaneously arising facilitators within the community75,76.
Career support and opportunity
Our study found that access to the career support and opportunity section is positively associated with higher use frequency and likelihood of recommending Rural Health Pro. The platform streamlines access to current funding and grants opportunities and job vacancies, providing users with an integrated interface for navigating and redirecting. This consolidation of financial opportunity addresses a critical need, as previous research indicates rural health professionals are 190% more likely than urban health professionals to prioritise financial assistance in their initial practice decisions77. As a tangible extrinsic reward, financial support may not directly enhance job satisfaction, though its absence can contribute to decreased satisfaction78. While providing financial and economic incentives to rural health professionals remains the most frequently mentioned retention strategy2,63,77,79,80, definitive evidence of its long-term retention impact remains limited63. Our findings demonstrate users’ feedback on the career support and opportunity section has been relatively positive. This may be because Rural Health Pro enhances accessibility to financial support information by merging available opportunities and directs them to the application form. The platform's role as an intermediary appears to effectively bridge the gap between rural health professionals and available financial support and career opportunities. However, future studies warrant examination of the applicants’ demographic characteristics, application patterns and behaviours, application success rate and the concrete impact of information access on recruitment and retention outcomes, as it may provide valuable insights into the platform's effectiveness and its support on rural health workforce development.
Limitations and future direction
This study has several limitations. First, the absence of unique identifiers prevented linking respondents and survey completion times, resulting in a cross-sectional rather than longitudinal analysis. This limitation also raised the possibility of multiple survey submissions by individual Rural Health Pro users, as this survey was distributed annually to all users over 3 years. Second, the high amount of missing data may have led to results that inadequately represent the broader views of rural health professionals (Rural Health Pro users), introducing selectivity bias and affecting our study's external validity. Third, the surveys were distributed by RDN, which manages and maintains Rural Health Pro, which may have triggered social desirability bias and influenced participants' responses. However, anonymity may have mitigated potential bias. Last, while the definition of capability was provided in the survey, varying interpretations of the term based on individual experiences and understanding may have introduced bias.
Future research could focus on more comprehensive evaluation of platform content quality and interactive design. Additionally, exploring the impact of cultural factors on digital platform usage and analysing the direct relationship between digital platform use and rural health workforce retention would be valuable areas of investigation.
Conclusion
The strength of Rural Health Pro lies in its inclusion of a wide variety of rural health information and resources, providing rural health professionals with faster and more convenient access while offering enhanced support and connection opportunities. Our findings emphasise the need for more diverse and comprehensive content to support health professionals of varying ages and educational backgrounds, as well as appropriate encouragement for virtual community of practice. Notably, the curated information and networking opportunities managed by a trusted organisation through the platform are what artificial intelligence systems cannot fully replicate at present.
Funding
Professor Alexandra Martiniuk was salary-funded by a National Health and Medical Research Council (NHMRC) Investigator Grant, and Dr MD Islam’s salary was supported by Professor Martiniuk's NHMRC grant. Yiwen Wang was supported by the University of Sydney International Stipend Scholarship and University of Sydney Tuition Fee Scholarship. Rural Health Pro is funded by RDN. There are no specific grants from funding agencies in the public, commercial or not-for-profit sectors for this program or research.
Conflicts of interest
The authors declare no conflicts of interest.
AI disclosure statement
The authors did not use any artificial intelligence tools to formulate hypothesis, design, conduct experiments, draft part of the original manuscript, summarise, paraphrase or significantly revise the manuscript. During the revision process to address the reviewers comments, the authors did use the AI agent in Google Analytics to identify the most common day of the week and time-of-day data.