


Introduction
Musculoskeletal and lifestyle-related health conditions often co-occur, which may place major physical and psychological burdens on individuals and may have negative socioeconomic implications in society1-4. The health-related quality of life of individuals may be affected through chronic pain and functional limitations, which may impact on the ability to participate in both occupation and leisure-related activities1,5,6. Lower productivity or the inability to work and the high costs associated with standard healthcare practices add to the socioeconomic burden of these conditions7,8. A high prevalence of comorbid musculoskeletal and lifestyle-related health conditions have been reported in populations in low- and middle-income countries (LMICs)4. For example, a study conducted in an under-resourced community in South Africa reported that comorbidities such as hypertension were commonly reported alongside musculoskeletal conditions such as arthritis9. Risk factors such as reduced physical activity levels have also been reported to be higher in under-resourced communities10.
Education, exercise prescription, targeted rehabilitation, and addressing risk factors form the cornerstone of prevention and treatment of many musculoskeletal and lifestyle-related health conditions11-13. The prevention and treatment of these conditions may involve long-term commitments to lifestyle modifications including physical activity management, a healthy diet, and avoiding smoking3,12,14,15. Optimal pain management, psychological support, and the facilitation of a full return to function including work following musculoskeletal conditions may be a lengthy process and relies on continuity of care16. These interventions often require visits to in-person facilities such as going to physiotherapy practices for lower back pain or attending training sessions at a gym to help manage type 2 diabetes16,17. This may be particularly challenging for individuals living in rural and under-resourced communities in LMICs where access to high-quality in-person health care and healthy lifestyle supportive services and facilities may be limited or unattainable18. This may be due to a combination of geographical inaccessibility, insufficient infrastructure, and resources (eg lack of health practitioner clinics and healthy food stores), along with financial constraints limiting the ability to afford high-quality services and healthier lifestyle options (eg gym memberships)10.
Although in-person health care at established facilities remains the gold standard of management, alternative options should be considered to assist with the prevention and treatment of musculoskeletal and lifestyle-related health conditions in rural communities in LMICs19. Digital health platforms and community-based interventions may need to be considered as an alternative20,21. Digital interventions may include telehealth (eg online consultations with health practitioners such as a general medical practitioner), telerehabilitation (eg online individualised rehabilitation programs offered by a physiotherapist), pre-recorded or live exercise videos, web-based or mobile app education strategies, and telephone calls or text messages for monitoring purposes22-24. Systematic reviews have provided support for the effectiveness of digital health care in the management of musculoskeletal conditions with regards to pain, quality of life, and functional capacity in general populations24,25. Conversely, barriers such as lack of wi-fi coverage, inadequate access to digital devices, and low digital literacy may inhibit successful implementation of digital health methods26. Community-based interventions may include training local health practitioners, parents, or volunteers to provide certain services that would otherwise be inaccessible, the distribution of educational materials within communities, message delivery via peers, and hosting educational workshops, among other strategies21. In support of the efficacy of community-based health interventions, a systematic review conducted in urban areas, mostly in high income countries, found that at least one lifestyle-related health outcome improved in most studies27. Further research is needed to explore what digital or community-based health care interventions may be implemented for the management of musculoskeletal and/or lifestyle-related health conditions in rural communities lacking access to sufficient, regular, and high-quality health care and healthy lifestyle supportive services and facilities.
A preliminary search of MEDLINE, the Cochrane Database of Systematic Reviews and JBI Evidence Synthesis was conducted, and no current or underway systematic reviews or scoping reviews were identified. Related reviews (eg investigating the efficacy of digital interventions for musculoskeletal conditions in general populations) have been performed24,25. However, no past reviews have focused specifically on digital and community-based health interventions using exercise and education for the management of these conditions with specific consideration of the socioeconomic, geographic, infrastructure-related, resource-related, and other factors relevant to rural communities in LMICs. The barriers, facilitators, feasibility, and impact of implementation of these interventions may differ in these settings compared to those reported in well-resourced high-income countries. For example, inadequate wi-fi coverage may mean that digital interventions would be ineffective in under-resourced communities.
Aims and objectives
The review therefore aimed to identify and describe the use of digital and/or community-based health interventions for exercise and education in the management of musculoskeletal and/or lifestyle-related health conditions in rural communities in LMICs. The secondary objective involved exploring the impact, feasibility, barriers, and facilitators of these interventions in the management of musculoskeletal and/or lifestyle-related health conditions in these communities.
Methods
Inclusion criteria
Participants
Studies involving participants aged over 18 years, of any sex and occupation, were included.
Concept
Any studies investigating digital and/or community-based health interventions implemented in the prevention, treatment, and management of musculoskeletal or lifestyle-related health conditions through education or exercise (including rehabilitation) were considered. Studies describing the development without implementation of such interventions were excluded. Studies where the primary diagnosis did not include a musculoskeletal condition or a lifestyle-related health condition were excluded. Studies focused on prevention only in a healthy population without any clear risk factors were excluded. Educational interventions targeting medication compliance or pharmacological strategies only were also excluded.
Context
Rural settings in LMICs, including upper middle-income countries, were considered. The classifications as defined by the World Bank was utilised28. Any communities in rural regions in LMICs were considered. The definition of ‘rural’ may differ based on different regions and local policies29,30. For the present review, study locations specified as rural by the involved researchers or, where unspecified, based on geographic coordinates indicating separation from urban regions, were considered as rural regions29,30. Any studies conducted in LMICs combined with high-income countries where the results could not easily be extrapolated were excluded. Any studies conducted in rural and urban regions where the results for rural regions could not be extrapolated were excluded. Studies that failed to specify the location of the research were also excluded.
Types of sources
Any experimental trials, cohort, case-control studies, case series, case studies, cross-sectional observational (retrospective and prospective) designs and qualitative studies published in the past 20 years were considered. The review was limited to research published in the past two decades due to the rapid rate of technological advances impacting healthcare systems and services. Literature reviews (narrative, scoping, or systematic), single-case studies, editorials and opinion pieces were excluded. Any studies where the full text could not be obtained or that were unavailable in English or Afrikaans were excluded.
The scoping review was conducted in accordance with the JBI methodology for scoping reviews with consideration of the guidelines by PRISMA for scoping reviews31,32. The full protocol is registered on the Open Science Framework database33,34.
Search strategy
A three-step search strategy was used. The first step involved an initial search of PubMed to identify articles on the topic and to assist with the development of a search strategy. The full search strategy was developed, including adjustments to the key terms, MeSH terms and Boolean operators as applicable to each database under guidance of a senior librarian at the Bongani Mayosi Health Sciences Library at the University of Cape Town. The following databases were included in the search of the literature: PubMed (MEDLINE), Scopus, Web of Science including SciELO, and EBSCOhost (with CINAHL, Africa Wide, Health Source and MEDLINE selected). To identify any further articles of relevance, the reference lists of included articles were searched. A grey literature search using Google Scholar to identify any further articles was also conducted. The search strategy for PubMed is available in Supplementary table 1.
Study/source of evidence selection
All articles identified during the search were combined and uploaded to Rayyan (Rayyan; https://new.rayyan.ai)35. This automated software has been recommended for use during scoping reviews, particularly for duplicate identification and screening purposes36. All duplicates were removed using this software. The titles and abstracts were screened by two independent reviewers (GG, TB) using blinding to determine if the eligibility criteria for assessment were met. Attempts were then made to retrieve the full texts of these studies. Full texts of available studies were evaluated against the inclusion criteria by two independent reviewers (GG, TB) using blinding. Reasons for exclusion were recorded. Any disagreements that arose between the reviewers at each stage of the selection process were resolved through discussion. No third-party consultations were needed.
Data extraction
Data were extracted from all articles using a self-developed data extraction tool based on the JBI template for data extraction37. The initial draft of the data extraction tool was modified and revised during the process of extracting data from each included evidence source (Supplementary table 2). The following data were captured to identify each article: authors, year of publication, and title. Study descriptors including the study design, sample size, and participant characteristic, geographic region, and socioeconomic status were extracted. Digital and community-based health methods used for exercise and/or education were described along with which musculoskeletal or lifestyle-related health conditions targeted. Where available, the impact of the method, any barriers or facilitators encountered during implementation, and any additional information regarding the feasibility of implementation were extracted.
Study selection
The initial electronic search of the four databases produced 1586 studies. Grey literature searches produced 11 additional studies. After removal of duplicates, 1323 studies remained. There was 91.0% agreement among reviewers at title screening level, with all conflicts resolved through discussion. Following title and abstract screening, 153 articles were identified for full-text review. The reviewers were 98.0% aligned at full-text screening level, with all conflicts resolved through discussion. Nineteen studies meeting the eligibility criteria were included in the review, two of which were identified by grey literature searches. The full search is presented in a PRISMA-Scoping Review (PRISMA-ScR) flowchart31 (Fig1).
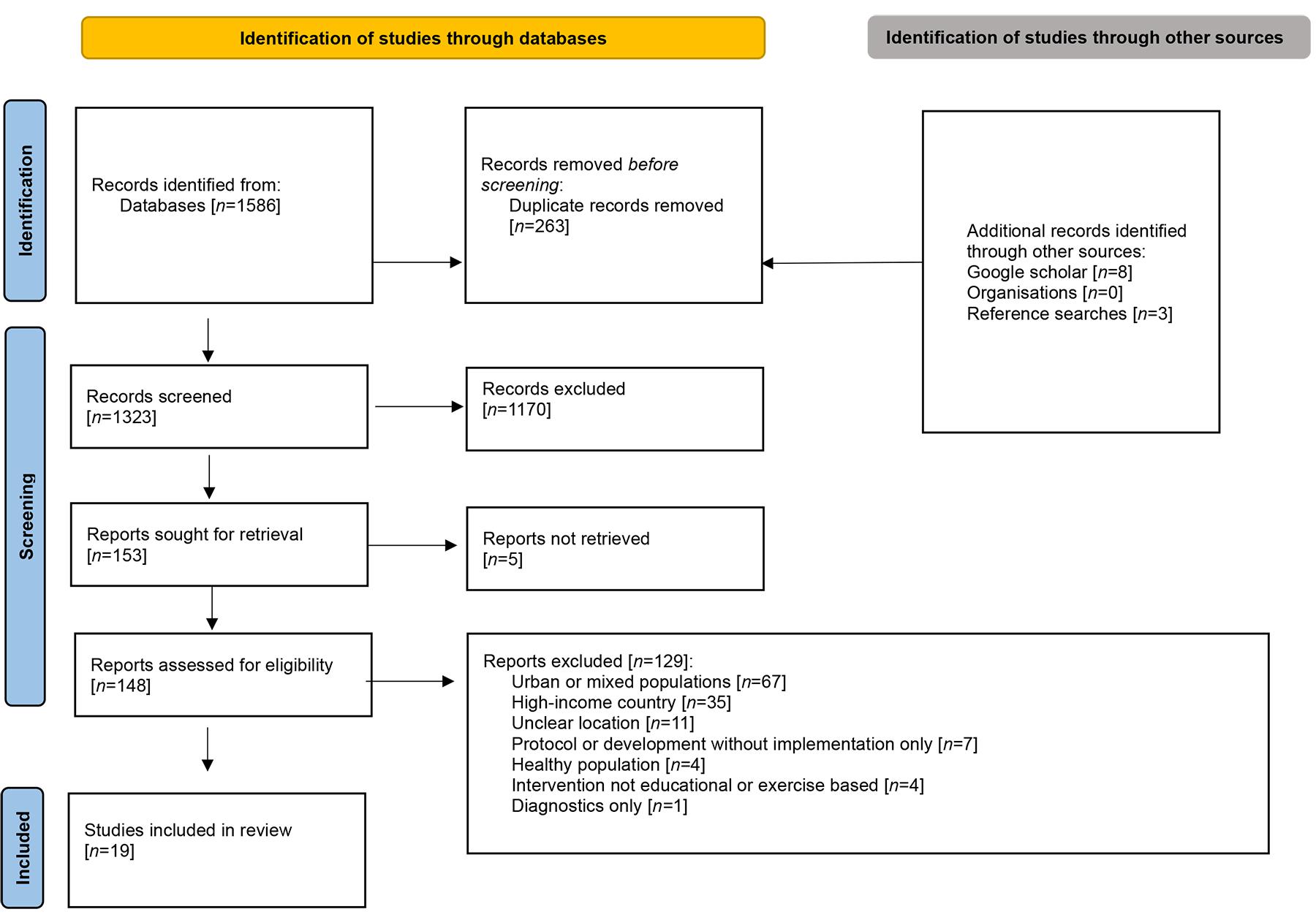 Figure 1: PRISMA-ScR flow chart for screened articles.
Figure 1: PRISMA-ScR flow chart for screened articles.
Results
Overview of included studies’ characteristics
The final 19 studies involved a range of study designs including randomised controlled trial (RCT) (n=8), quasi-experimental pre-test–post-test intervention (n=6), mixed-methods (n=3), qualitative (n=1) and observational (n=1) study designs38-56. Three of the reports evaluated different components related to a three-arm RCT study50,51,53. The number of participants included ranged from 30 to 11,454 participants across studies.
Most of the studies were conducted in Asia, including seven studies in Bangladesh, five in India, three in China, as well as studies in the Philippines (n=1), Pakistan and Sri Lanka (n=1) and Vietnam (n=1)38-42,44-46,48-56. Two of these studies involved multiple Asian countries44,55. The only studies involving other regions included one study conducted in Nigeria, Africa and another in Brazil, South America43,47. All studies were conducted in rural regions, with one study by Harshitha et al (2022) comparing a rural and urban group (the rural data were extracted for the review)42. Most of the countries where studies were conducted are classified as LMICs (n=15), with the remaining two in China classified as relating to an upper middle-income country, based on World Bank classifications28. Most studies (n=17) targeted lifestyle-related health conditions, with only two focusing on musculoskeletal conditions (namely chronic lower back pain and arthritis-related illness). The most common conditions targeted by interventions in studies were diabetes and pre-diabetes (n=10), followed by hypertension (n=6), cardiovascular disease (n=2), and cerebrovascular accidents (n=1), with some studies targeting multiple conditions. Study interventions periods and follow-up periods ranged from 6 weeks to 48 months. The details of each study are shown in Appendix I, Appendix II and Appendix III.
Types of interventions for lifestyle-related health conditions
Sixteen studies with interventions to manage lifestyle-related diseases involved community-based components38,39,41,42,44-53,55,56, half of which also included digital health components. One study targeting diabetes involved only a digital intervention40.
The interventions all involved a health education component38-42,44-53,55,56. Topics mainly covered lifestyle education such as dietary advice regarding sufficient fruit and vegetable intake, limiting salt intake, and other unhealthy food choices, performing sufficient levels of physical activity, and avoiding smoking and other forms of substance abuse38,45,48-50,52. Disease specific health education was also included in three studies41,46,50.
Methods to deliver education included home visits39,44,45,47,55, one-on-one patient sessions in various community and health facilities38,48,49,53, group education sessions or seminars38,41,46,52, support groups49, and motivational sessions39. Some interventions included the arts, for example theatre productions and puppet shows49,50. One study also included cooking and yoga demonstrations in communities38. Printed educational materials including booklets, pamphlets, and posters were distributed as part of seven studies38,39,41,42,45,46,52. Five studies mentioned that advice was individualised based on identified risk factors38-40,48,52. A mass media campaign including broadcasting was reported in one study52.
In addition to education, six studies included screening and monitoring of blood pressure, blood glucose, or other health parameters39,41,44,47,49,52. Training workshops for doctors, community health workers (CHWs), or both were also reported in six studies41,44,47,49,55,56. A local diabetes care centre was established as part of one study49.
Digital interventions included mostly m-health in the form of mobile voice and text messages to patients45,50,53,56, smartphone apps for use by health practitioners48,55,56, with educational videos for patients based on individualised risk factors48, as well as phone calls46. One study reported the development of a website for local doctors to guide patient management and to generate individualised advice to patients based on risk factors40.
Nine of the interventions mentioned CHWs delivering various components such as screening and education38,41,44,45,47-49,52,55. Other studies mentioned the use of locally trained facilitators53, doctors56, unspecified non-healthcare staff46, nursing students, and community nurses39.
Impact of lifestyle-related health interventions on individuals and communities
Based on various objective and subjective parameters, a positive impact was reported in rural communities following lifestyle-related health interventions in all studies. Two studies reported a reduction in the prevalence of lifestyle-related health conditions. namely diabetes53, hypertension, and obesity46. Ten studies reported improvements in blood pressure measurements38,39,41,44-47,52,55,56, three studies reported improved blood glucose levels38,48,53, two studies reported improvements in body weight measurements38,45, and one study noted lowered urinary salinity45. Lower mortality rates were reported in two studies44,56, along with lower recurrences of cerebrovascular accidents and fewer hospitalisations in one of these studies56. Improvements in self-reported lifestyle behaviours were reported in six studies40,41,45,46,50,52, and better medication adherence was reported in four studies39,44,55,56. Improved health literacy with improved knowledge scores was reported in four studies38-40,42. Three studies reported better quality-of-life scores44,45,56. One study reported improved performance in function measured through the ‘timed up and go test’ for patients who had experienced cerebrovascular accidents56.
The potential value of training locals and CHWs was mentioned by two research groups – the training may have resulted in enhanced skills and assisted with the creation of local employment44,49. Four studies also mentioned a possible reduction in healthcare costs with the interventions implemented47,49,51,56. Two studies reported that locals started growing their own vegetables to help support healthier dietary choices, with one mentioning that local stores also stocked healthier options due to the intervention49,51. However, formal objective assessments were not described to substantiate the abovementioned findings in all except a study by Morrison et al (2019), which utilised group interviews and focus groups among participants51.
Type and impact of interventions for musculoskeletal health conditions
Only two studies investigated the use of community-based and/or digital interventions for musculoskeletal health conditions in rural communities43,54. A study by Rana et al (2010) involved health education provided through small groups and home visits, printed handouts, videos, and theatre productions for the management of arthritis-related illness54. Significant improvements in self-rated health and reduction in arthritis-related illness were reported in participants who were compliant with the intervention, compared to those who were not54. A study by Ibrahim et al (2018) involved a pilot RCT for the management of chronic lower back pain through exercise prescription only, education only, or exercise prescription and education respectively, provided by physiotherapists within the community43. All groups demonstrated improvements in pain and function, with the greatest improvements observed in the group receiving both exercise and education43.
Barriers to implementation of interventions
Only a few studies investigated barriers related to the implementation of interventions, and these mostly related to digital health components40,45,50. For mobile messages, one study reported a reluctance by individuals to share mobile numbers, which limited sign-ups, and changing mobile numbers following sign-up as barriers to sending messages50. For those who signed up, participants reported not listening to the messages due to a lack of interest, being too busy, not recognising the voice used, and assumptions that the messages were advertisements, unsolicited, or scams50. A study by Jahan et al (2020) reported that mobile messages may have been too short and generalised for some participants, although no formal assessment for obtaining participant input regarding this was reported45. Technological faults limiting the ability to deliver mobile messages50 and disruptions in internet and electricity supply limiting access to a website health aid were also reported40. Lack of personalisation and over-standardisation were raised as concerns by some participants being managed with doctors using a web-based aid40.
Social and environmental challenges involving disease-related stigmas and gender norms (eg restrictions on the movement of females) were reported as barriers to the ability to follow guidelines recommended during health interventions50,51. Insufficient funds to travel to facilities or pay for healthcare services needed were also mentioned by participants as a potential barrier to complying with suggestions made as part of the intervention51.
Facilitators to implementation of interventions
Community engagement during development and/or implementation of interventions was mentioned by participants and researchers as a potential facilitator for the applicability and uptake of interventions38,39,49,53. This may have allowed for the use of more context-specific strategies, for example creating spaces for exercise, promoting access to healthier food based on community needs, and providing recipes for healthier food that were considered acceptable within the community38,53.
Group discussions, engagement, and social support were also mentioned as valuable for the transfer of information and increasing the likelihood of following advice provided38,51. Community awareness regarding health conditions and healthier choices were also described as helpful since this allowed participants to feel more comfortable to follow advice51. The relevance and repetition of information provided during education were also mentioned as potential facilitators for the uptake of interventions50,51. Participants in one study indicated a preference of information provided by a doctor compared to other individuals during mobile messages50. Demonstrations such as in-person yoga sessions were also described as helpful to increase the chance of following the advice provided38.
Two articles mentioned that cost savings related to the use of a group intervention and the use of a simplified approach to management may have facilitated the feasibility of the interventions41,55. Mohan et al (2012) mentioned that facilities could be developed due to private donations49.
Discussion
Value of community-based and/or digital health interventions in rural communities
The studies included in the review reported positive impacts on various lifestyle-related health conditions and two musculoskeletal conditions through community-based and/or digital health intervention in rural communities in LMICs. These included reduced disease incidence and severity, improved lifestyle choices, better health literacy, improved function, and better quality of life43,45,51-53. The improvements observed in these rural under-resourced settings are in line with research of digital interventions and community-based interventions respectively for musculoskeletal and lifestyle-related health conditions in varied, urban, and high-income settings25,27,57,58. This positive trend is encouraging, although interventions for rural settings in LMICs would need to be modified based on community-specific needs and availability of resources59.
Feasibility of community-based and/or digital health interventions in rural communities
Almost all the interventions in the reviewed studies were multimodal and community-based, with just under half including digital components38,39,41-56. The use of multimodal interventions may be important to help address the multifactorial causes underlying lifestyle-related and musculoskeletal health conditions60,61. Conversely, funding and resource constraints in rural communities in LMICs need to be considered in the development and implementation of interventions to ensure feasibility and appropriateness62. It was unclear from most reviewed studies if attempts were made to address possible barriers to the uptake of interventions during development. Nonetheless, some studies identified that the use of group education and screening, arrangement of transport to larger health facilities in groups, and the development of household vegetable gardens were among the potentially helpful strategies identified and implemented 38,43-46,49,51-53,55. In support of the cost-effectiveness and value of a group-based approach, an RCT demonstrated that group education for diabetes was as effective as individual education, with improvements in glycaemic control, quality of life, and BMI among other health outcomes reported in both groups63. Conversely, a study conducted in an under-resourced region of South Africa found that household gardening was insufficient as a source of healthier food, partially due to cultural and spatial barriers in the community involved64. Promoting access to healthy food options and creating safe spaces for exercise may require collaboration between NGOs, research bodies, and local and national governmental policies65. Innovative plans tailored to local communities, regional, and country-specific contexts are needed to address these conditions in rural under-resourced communities. One example might be the provision of healthy food options at workplaces and schools through an NGO65.
It has previously been reported that digital interventions appear to be cost-effective, may enhance access to information, help to streamline individualised patient care, and have been associated with improved health outcomes57,58,66. The present review provides support for the potential positive impact on health outcomes46,48,54-56; however, the relative contribution of different components (including community-based compared to digital) cannot be determined. Nonetheless, most of the barriers reported in the present review related to technological faults and a reluctance to engage with digital content, which may limit the applicability of digital components in rural under-resourced communities40,50. There may also be safety concerns with certain digital health interventions; for example, when utilised to promote or prescribe physical activity, an increased risk of side effects has been reported67. Digital components may therefore be more helpful as an adjunct to community-based interventions rather than in isolation in these settings. This may explain why only one study in the review utilised a digital intervention in isolation40.
The duration of interventions in reviewed studies ranged from 6 weeks to 4 years, with the repeatability and long-term impact of interventions remaining unclear. The sustainability of these interventions in rural settings should be considered in future research studies.
Critical importance of community involvement
Many studies in the present review indicated the importance of community engagement forming part of interventions, although what this entailed was not always clearly defined38,39,49,53. In general, community engagement may be helpful to ensure that interventions are culturally and socially sensitive, and appropriate for each unique setting, which may increase the likelihood of interest and acceptance within local communities59. In support of the value of community engagement, a systematic review involving 24 studies reported that community engagement utilised in under-resourced settings was associated with positive changes in access to health services, health literacy, and other health outcomes68. Similarly, a meta-analysis of 131 studies of public health interventions utilising community engagement for various chronic illnesses reported significant improvements in various health outcomes including lifestyle behaviours, self-efficacy, and social support69. Studies were grouped according to models or approaches to community engagement, including a community-independent approach, where the health-related need and response was facilitated by the community; a third-party approach, where the health need was identified by external parties who subsequently engaged with local stakeholders for the development of the intervention; and finally, a community implementation approach, where the community assisted with facilitating the intervention after development69. However, the use of different models of community engagement did not appear to have a significantly effect on the impact of the interventions69. Although the focus of these past reviews was on disadvantaged communities, most included studies were still conducted in high-income countries68,69, with the present review providing support for the feasibility and value thereof in rural settings in LMICs.
CHWs were involved in various aspects of the implementation of interventions, such as education and health monitoring, in many of the reviewed studies38,41,44,45,47-49,52,55. A systematic review investigating health interventions facilitated by CHWs provided support for both the cost-effectiveness and the efficacy of these interventions for various conditions including the mitigation of cardiovascular disease risk70. Most studies in the systematic review were conducted in under-resourced settings, although in high-income countries70, with the present review providing support for the potential value of CHWs in rural parts of LMICs. Regardless of the setting, CHWs may be best suited to assist with the administration of interventions due to their familiarity with local socioeconomic circumstances, and the ability to tailor communication and administration with the necessary linguistic, social, and cultural sensitivity required within their communities70. Consideration should also be given to the cultural competence of researchers conducting studies. This was not clearly described in reviewed studies, and should be considered in future research.
It is apparent that community involvement in various forms should be prioritised during the development and implementation of future health interventions. To assist with this, Pardoel et al (2022) developed a framework to guide the adaptation of community-based health interventions based on local cultures and contexts71. This included aspects such as beliefs regarding diet and physical activity, meaningfulness such as religious practices, family, and social structures, among others, all of which would need to be considered during the development of a health intervention targeting lifestyle-related and musculoskeletal health conditions71.
Educational content for interventions
With regards to educational content forming part of interventions, information across various health conditions in reviewed studies included dietary advice, avoiding substance abuse, and performing sufficient levels of physical activity. The importance of these lifestyle interventions are well known65, and form part of various structured guidelines such as the National Institute for Health and Clinical Excellence guidelines for the management of Type 2 Diabetes72 and the Dietary Approaches to Stop Hypertension guidelines73. Since tobacco and alcohol use, physical activity, and dietary choices are among the main modifiable risk factors across many non-communicable diseases, this should be included as a minimum in future health interventions targeting lifestyle-related health conditions65. Health literacy, including awareness of these risk factors, and recognition of signs and symptoms requiring medical care, are also needed74. A systematic review has provided moderate evidence to support the association between health literacy and diabetes knowledge, and provided some support for improved lifestyle behaviours75. Conversely, the studies were inconclusive or of insufficient quality to demonstrate a positive impact on various health outcomes overall75. Studies included in the present review provide support for the value of community-based and digital interventions in promoting health literacy in rural parts of LMICs. Increased knowledge regarding when to seek medical help is also important, since early detection allowing for earlier management may also be key in reducing the severity and complications of diabetes and hypertension76,77. The latter conditions were the most commonly targeted by interventions in reviewed studies, which may be due to the high prevalence rates of these conditions in LMICs78,79. Health literacy and educational interventions should focus on the most common conditions identified in targeted communities.
Limitations and future directions
Although many of the studies were RCT designs with large numbers of participants, other study designs were insufficient to limit the potential of confounding variables impacting results rather than the intervention implemented80. However, commonly utilised quasi-experimental designs are often the most ethical and practical approach to evaluate health outcomes and feasibility in under-resourced rural settings in potentially vulnerable populations where access to sufficient health care may be limited80. Most interventions in reviewed studies were also multifactorial, making it difficult or impossible to determine the relative contribution of different components. Quality analyses and meta-analyses were beyond the scope of the current review, since the aim was to broadly describe various factors surrounding interventions in rural settings. To provide evidence-based practice guidelines regarding the efficacy, systematic reviews and meta-analysis of specific health conditions and specific interventions, restricted to RCT designs, without limitations on the study settings, may be more appropriate. For example, systematic reviews of RCT studies provide support for digital interventions in the management of type 2 diabetes and hypertension in varied populations57,58.
The review identified only two studies involving musculoskeletal conditions, one of which was a pilot study. Therefore, there was insufficient information available to explore the value and feasibility thereof collectively in rural parts of LMICs. Future research in rural regions where physically demanding occupations are common, such as agricultural regions and small-scale fishing communities, are recommended, since the risk of musculoskeletal conditions in these settings is high81,82. Interventions specifically tailored to the occupational and socioeconomic demands of target communities should be considered. Most of the reviewed studies were conducted in certain parts of Asia, therefore the findings may be most applicable to the limited number of countries included . Future research in rural areas in a broader range of LMICs is needed. For example, only one African country was included in the review, significantly limiting the applicability of findings to this region. Future reviews should also aim to compare the impact of interventions implemented in the Global South compared to in the Global North.
Only articles available in either English or Afrikaans were included based on the language proficiency of the reviewers. This may have led to the exclusion of potentially relevant studies, which may limit the generalisability of the findings.
Conclusion
Community-based health interventions with and without digital components may have a positive impact on various health outcomes related to lifestyle-related health conditions and seem to be feasible to implement in rural regions of LMICs based on reviewed studies. The types of interventions utilised, strategies to facilitate uptake and to reduce potential barriers should be considered during the development of future interventions for rural, under-resourced settings. Plans to promote sustainability of developed interventions should also be considered. This may help to increase the likelihood of the value and feasibility in these settings. Community involvement during the development and implementation of interventions is recommended to ensure the appropriateness to local sociocultural and economic settings.
Acknowledgements
We would like to extend our heartfelt thanks to Ms Gill Morgan, who assisted with the development of the search strategy utilised in the review.
Funding
The study was performed as part of a University of Cape Town Faculty of Health Sciences postdoctoral research fellowship, with no review-specific funding received.
Conflicts of interest
There are no conflicts of interest to report.
AI disclosure statement
No generative AI or AI-assisted artificial tools were used in the conduct of this research or the preparation of this manuscript.