




Introduction
The Indonesia National Population and Family Planning Board reported that Indonesia ranks 37th in the world and second among South-east Asian nations for number of adolescent marriages and pregnancies1. WHO defines adolescents as individuals aged 10–19 years2. Even though the number of adolescent marriages has decreased worldwide, it is estimated that one-third of marriages in developing countries are of children under 18 years, most of whom are girls3. Data from several countries show that more than a quarter of girls under 15 are married. Underage girl marriage is a violation of human rights and gender-based health4. Girls who marry before the age of 18 have an increased risk of dropping out of school, social isolation, poverty, high fertility with short birth intervals, and poor mental health5. Adolescent pregnancy is also associated with an elevated maternal mortality ratio. The maternal mortality ratio is higher among childbearing adolescents than among women aged 20–24 years6. Adolescent maternal mortality is mostly due to complications during pregnancy and childbirth. Hence, adolescent pregnancy has been regarded as a major health problem in most countries, especially in developing nations, including Indonesia7.
Sychareun et al (2013) found that the health risks among pregnant adolescents are even higher in rural areas where health service discrepancies occur8. The age-related pregnancy and childbirth problems in rural areas are compounded by poor economic conditions, low educational attainment, and inadequate knowledge of reproductive health8,9. Mesuji Subdistrict in Mesuji District is a rural area in Indonesia with a high rate of adolescent pregnancy. A recent report indicates that in 2017 the estimated adolescent pregnancy in Mesuji District was 30% of the total number of pregnant women10. At the Subdistrict and village levels, the rate even reached 70–80%11. Mesuji Subdistrict has the lowest public health development index among 12 districts and cities in Lampung Province. At the national level, Badan Pusat Statistik, the Indonesian National Statistics Bureau, reported that 11% of all female adolescents in Indonesia are married at the age of 10–15 years12. A recent report from the National Population and Family Planning Board reveals that the age-specific fertility rate among female adolescents aged 15–24 years is 331: of 1000 female adolescents aged 15–24 years, 33 have already given birth.
The data above underscore the need to understand the factors contributing to adolescent pregnancy in rural areas. Therefore, this study aimed to (1) uncover factors contributing to adolescent pregnancy in rural Indonesia, and (2) formulate community-based actions to address the problems. This study is significant because exposing adolescent reproductive health issues is essential for reducing maternal and neonate mortality as well as minimizing negative social and economic consequences of premarital sex and childbirth at an early age13.
Methods
Design
This research was participatory action research (PAR) conducted from June 2017 to November 2018. PAR is a method that originated from the sociology and education disciplines. This method focuses on partnerships between researchers and research participants in a collaborative effort to overcome specific problems. PAR also encourages the active participation of the community in resolving issues of concern14. PAR is more directed towards joint learning in uncovering the cause of a phenomenon or problem rather than scientific proofing15. There are three main components of PAR: participation, action and research16. These components go together in the following way: active and democratic participation of the people being observed and related stakeholders in the production of new knowledge through rigorous research that results in concrete action intended to make social change17.
Study setting
This research was conducted in two remote villages, Wiralaga 1 and 2, Mesuji Subdistrict, Mesuji District, Lampung Province, Indonesia. Geographically, these two villages are situated on the banks of Mesuji River, 29.5 km from the capital of Mesuji District on the border separating Lampung and South Sumatra provinces. The population of Wiralaga 1 was 3367 people with 846 households, and Wiralaga 2 was 3053 people with 814 households. Most of the population relied on the forest and river for their livelihood, such as logging and fishing.
Informants
Informants in this study were recruited voluntarily. They were teenagers, parents, religious leaders, community leaders, village officials, subdistrict staff, teachers, and primary health center staff. The informant criteria were: a resident of Wiralaga 1 or Wiralaga 2 and living in the research setting for at least 5 years (for all informant categories), aged 18–24 years (for teenagers), having teen children (for parents), active employment status (for village officials, subdistrict staff, teachers, and primary health center staff), teaching in schools located in Mesuji Subdistrict (for teachers), and posted at the Mesuji Subdistrict Primary Health Center (for primary health center staff). There were no criteria for the marital status of teenagers or pregnancy history of female adolescents who participated in this study.
Characteristics of informants: Most of the teenagers who participated in this study were unemployed and few were students. The religious leaders were respected male senior residents. They were responsible for leading religious ceremonies, including marriages. They relied mostly on fishing for their livelihood. Community leaders were head of village, village officials, and adat (customary law) council members. The village head and officials are formal government positions at the village level. Hence, they receive monthly remuneration from the state budget. The adat council is an informal tribal body and thus its members do not get monetary compensation. The adat council consists of senior respected residents (mostly elderly male residents). Village officials consisted of village secretaries and chairmen of the neighborhoods of both Wiralaga 1 and Wiralaga 2. The subdistrict staff were the Mesuji Subdistrict Mayor and the head of the village development division. Informants from the teacher category were senior teachers who were civil servants. The primary health center staff were midwives and medical doctors working in the Mesuji Subdistrict Primary Health Center.
Data collection and analysis
The primary data regarding factors influencing the occurrence of adolescent marriage and pregnancy were collected through focus group discussions (FGDs) (Table 1). Eligible informants were invited to attend meetings with the researchers at the subdistrict office. The first meeting was held in June 2017, attended by approximately 20 teenagers (male and female) aged 18–19 years, and 10 community leaders, including village officials and religious leaders. Subsequently, these 30 people were appointed as the local collaborators in this study. Some local collaborator functions were holding FGDs, educating the community, and advocating for local government. As well as being research partners, local collaborators were expected to function as stimulants for community behavior change related to reproductive health.
Four FGDs were held. Each FGD was conducted as a morning session, with each afternoon used for a session comprising relevant activities, as described in Table 1.
The FGDs were conducted early in the day in the subdistrict office main hall with a small number of participants. In the afternoon, the FGD discussants and additional participants attended other PAR activities at the same place. All FGDs were led by the researchers, by using semistructured discussion guidelines, and were audio-recorded and transcribed verbatim. In addition to the FGD data, the researchers took field notes based on their observations and reviewed report documents obtained from the primary health center and Mesuji Subdistrict government office.
The analysis was conducted by trained researchers from the Ministry of Health (DEE, LH, APN) and the National Population and Family Planning Board (IH). The lead author, DEE, along with APN and IH, read the textual data several times to gain an understanding of the relationship between the data and the research purposes. Codes were generated and synthesized into key factors influencing the occurrence of adolescent marriage and pregnancy in Mesuji Subdistrict. The analysis was performed inductively by condensing raw textual data into a concise format and establishing a clear relationship between research objectives and research findings generated from raw data18. The summary of the codes used is presented in Table 2.
The principal investigator (LH) then double-checked the synthesized results. The double-checking technique was intended to achieve researcher triangulation19. This study also employed multiple data sources and multiple methods triangulation20. The multiple data sources triangulation was performed by gathering data at different times. Multiple methods triangulation occurred because the researchers used more than one data-collection technique, including taking field notes, direct observation, and report document review20. A member check of synthesized analyzed data was applied to ensure the validity of the key factors identified in the data21. The emergent key factors were taken into a discussion with local collaborators to achieve agreement. The engagement of the local collaborators in the analysis is in accordance with the purpose of PAR, producing new knowledge through active and democratic participation from the people being observed16. The member checking also involved subdistrict and village government to gain feedbacks. The results were also taken into consultation with related stakeholders, including the Maternal and Child Health Directorate Ministry of Health, National Population and Family Planning Board, and National Institute of Health Research and Development. The complete stages of PAR used in this study are presented in Figure 1.
Advocacy
The advocacy was targeted to both the policy-makers and the target community. Following the advocacy methods developed by the WHO, after each meeting, the researchers prepared a summary of findings including the problems, current situation, and needs of the research participants to be presented and discussed with the Mesuji District Government. The presentations and discussions were held face to face and attended by decision-makers, including the Mesuji District Mayor, Director of Mesuji District Health Department, and Director of Mesuji District Social Department. Similar methods were applied at the Subdistrict and village levels. The involvement of the targeted policy-makers in the research process is important for gaining trust and support and is one of the effective advocacy strategies intended to make a change or create policy on an issue of concern22. The advocacy to the Mesuji Subdistrict community was conducted through the dissemination of research results and health education. The health education material was short videos showing the danger of adolescent marriage and pregnancy. Advocacy that targets the community is aimed at raising awareness and stimulating the active participation of individuals to overcome public health issues23.
Ethics approval
This study was approved by the Research Ethics Committee of the National Institute of Health Research and Development, Ministry of Health of Indonesia, under ethics approval number LB.02.01/2/KE.171/2017 and LB.02.01/2/KE.124/2018. All research informants signed informed consent indicating that they agreed to participate in the study. Previously, they were informed that the individual identities of the people involved would not be disclosed in any report or publication without their consent.
Table 1: Participatory action research meetings and aims in Mesuji District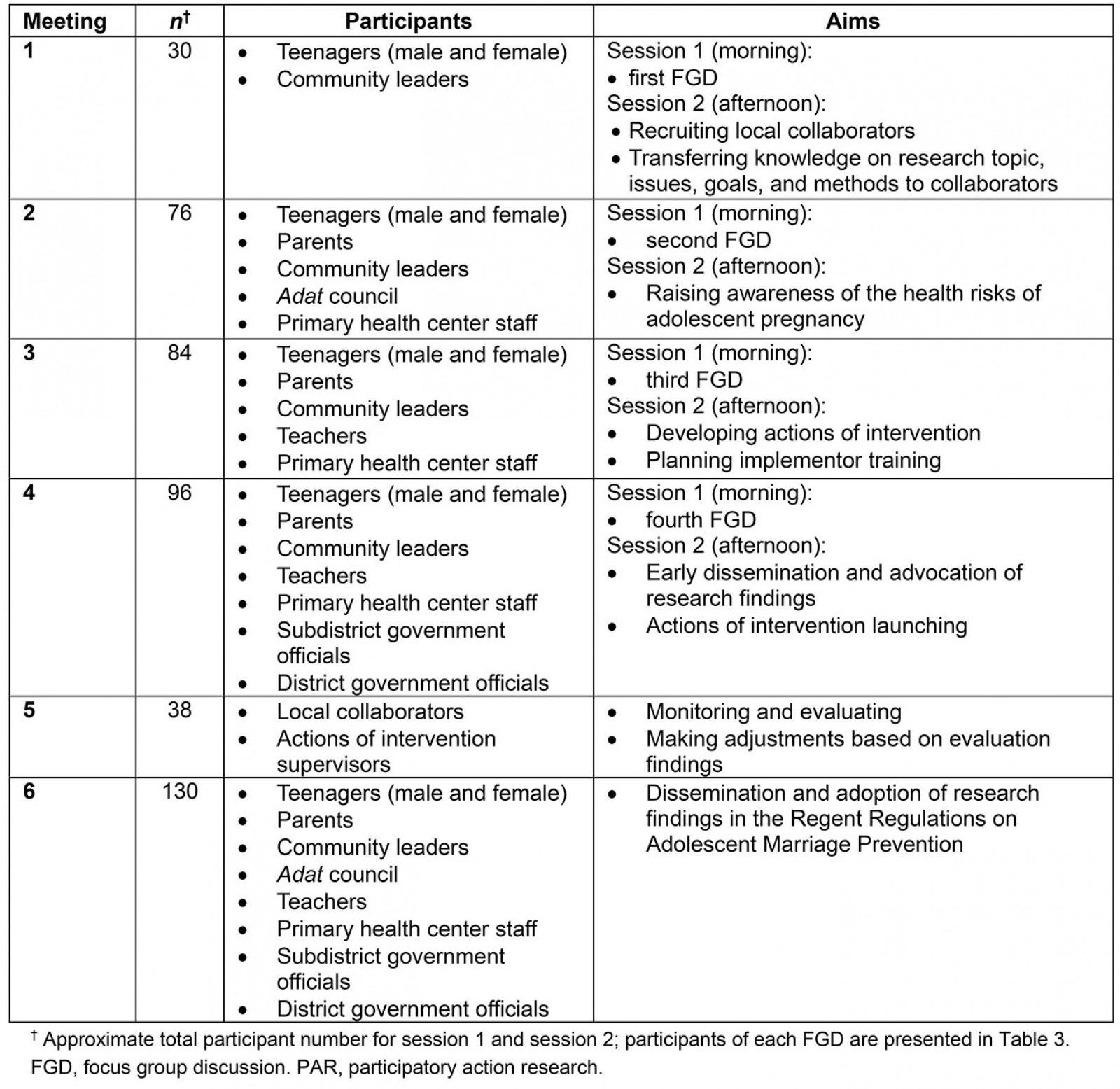
Table 2: Summary of codes and key factors influencing adolescent marriage and pregnancy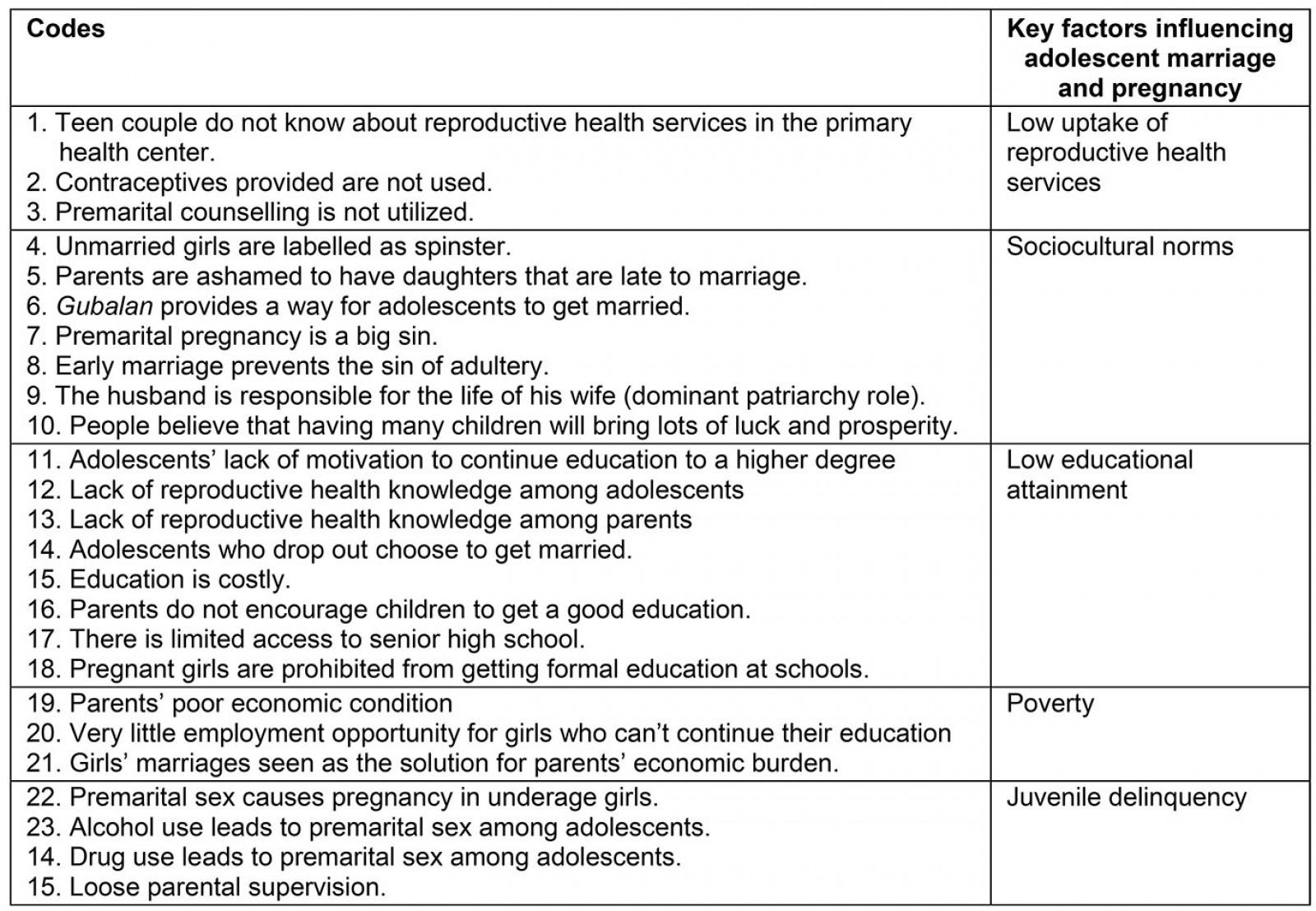
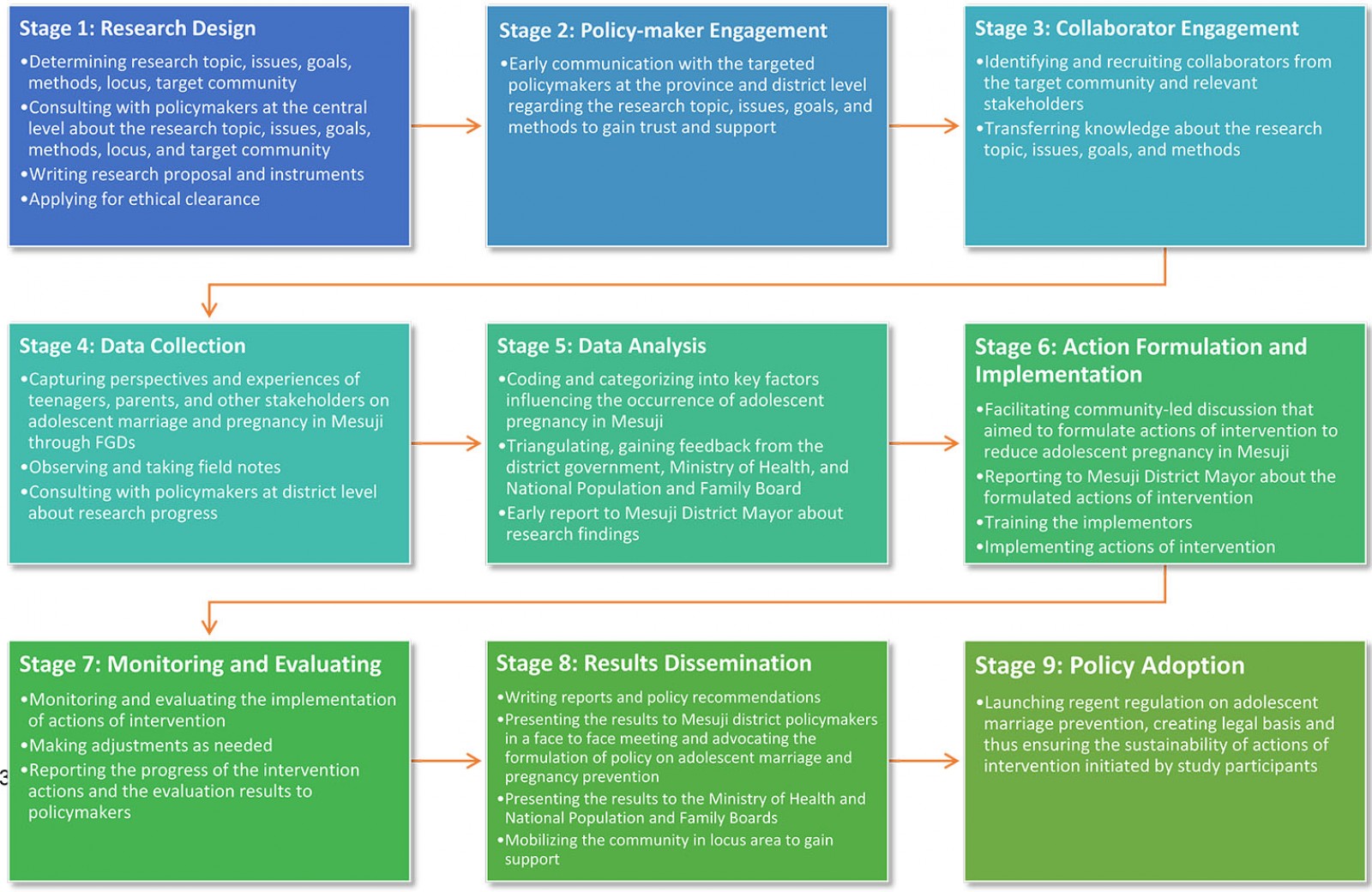 Figure 1: Research stages.
Figure 1: Research stages.
Results
As mentioned, four FGDs were held in the data-collection stage. The FGD participants are summarized in Table 3.
The analysis revealed that five key factors influenced the occurrence of adolescent marriage and pregnancy in Mesuji Subdistrict: low uptake of reproductive health services, the norms prevailing in the Mesuji community, low educational attainment, poverty, and juvenile delinquency. Each factor is elaborated below. This section also presents the results of advocacy and actions of intervention initiated by the study participants.
Low uptake of reproductive health services
The first factor affecting teen pregnancy was the low penetration of reproductive health services. Early pregnancy is likely to cause reproductive health complications in women and can lead to the death of both mothers and infants. Early pregnancy in Mesuji Subdistrict was triggered by the low uptake of reproductive health services and contraceptive use, as indicated by the following physician, who has been working in the Mesuji Subdistrict Primary Health Center for 5 years.
... contraception is provided at the primary health center. The National Agency for Family Planning also offers contraceptives. There is also advice and guidance on prospective brides, although so far, it has scarcely been used. Family planning coverage is also low. If couples or their parents want to come here, we will teach them about healthy pregnancy. Since they are married at a young age, we may advise them to delay pregnancy. (second FGD)
Social and cultural norms
In Mesuji, there is an adat regulation known as Gubalan. Gubalan is a customary mechanism to permit young couples to get married. The adat council will issue Gubalan under two conditions: first, when a couple does not have permission from the bride’s parents; second, when a young girl is pregnant before marriage.
Gubalan is a social, traditional product of the Mesuji community whose primary aim is to prevent negative stigma to the bride and her kin. Gubalan is not in violation of the law if the bride and groom are at a proper age to marry according to Indonesian regulation. However, most brides who marry through the Gubalan mechanism are underage children. This phenomenon is illustrated in the following quote from one of the male adat council members.
… If they are not allowed to marry, they will come to the Gubalan local council. We are faced with a difficult decision because often, the girl is already pregnant. So, what are we supposed to do? We do not have a choice but to marry them. (second FGD)
The social norms implemented in the Wiralaga community also promoted early marriage. Girls who marry late were stigmatized as ‘spinsters’ and ‘undesired’. Parents encouraged their daughters to marry early. It is not unusual for marriages in Mesuji to occur when girls are too young, from both a legal and a medical perspective. The phenomenon was pointed out by a female adolescent in the first FGD:
If a girl gets married late, she is called a spinster or undesirable. So, when a girl has a boyfriend already, she is generally told to get married soon. (first FGD)
After a marriage has taken place, the couple’s parents will allow their children to have children soon. This phenomenon is closely related to the belief that having more children brings prosperity. If the first childbirth occurs at a young age, it will increase the likelihood of having many descendants. One female adolescent who had experienced early marriage and pregnancy pointed out:
We are not trying to delay having children. The sooner we have children, the better because if we delay, we feel that we will have to wait any longer. Our parents are encouraging us to have a child soon. (first FGD)
Low educational attainment
There was agreement that low educational attainment was one factor that led to adolescent pregnancy. Most of the children in the study setting were educated only until they graduated from elementary or junior high schools. The following excerpt from one of the village officials (included in the community leader category in the third and fourth FGDs), who had good knowledge on the social and economic conditions of Mesuji people, illustrates this phenomenon.
Most of the kids here only graduated from elementary school or junior school at most. Parents do not encourage their kids to go to school because, for example, if the kids want a state senior high school, they need to go out to the city. We do not have a senior state high school here. Meanwhile, getting a good education in the city is costly. (third FGD)
The above quotation shows that the limited access to quality education and parents’ low economic status are reasons adolescents did not continue their education to a higher level. The available state-owned schools in Mesuji Subdistrict are an elementary and a junior high school. If adolescents wanted to attend school in a state-owned high school, they had to go to the Mesuji District center or Lampung City, the capital of Lampung Province. In addition, the regulation imposing the termination of formal school on pregnant girls increased the dropout rate. The following information from a teacher illustrates this circumstance.
There are some girls who drop out of school every year. Most of them have been due to pregnancy. School rules do not make it possible for them to continue their education. We feel bad, but what else we can do. That is the policy. Another reason is that their parents do not allow them to continue higher education. It is expensive, so it is better to work to help the parents. (third FGD)
Beliefs about the domestic roles of women was evident in the daily life of the Mesuji community. Women are believed to be destined to take care of the kitchen and the household. Hence, most of the girls in this research locus did not have the highest education level. A teacher, a discussant of the fourth FGD, elucidated this phenomenon.
Daughters are supposed to take care of what is in the kitchens, so why do they need to go to higher schools? So it is uncommon for them to get to high school or even college. (fourth FGD)
Girls who could not continue higher education eventually chose to get married. Because of their low level of education, there was no motivation for them to postpone marriage and pursue a good career as a means of self-actualization. As pointed out by one junior high school teacher in the third FGD, ‘girls who are unable to continue studying will be married. They think about what else they should do if they do not get married’.
The low level of education undoubtedly led to a lack of knowledge about the risk of adolescent pregnancy. Most of the participants agreed that there was still a lack of understanding about women’s reproductive health and the ideal age for the first pregnancy. This appeared to be the case with both the girls and the parents. They considered marriage and pregnancy to be necessary and would not cause problems even when they are young. This ignorance eventually led to a permissive attitude towards early marriage and pregnancy. The following is an excerpt from one of the community leaders in the fourth FGD.
The knowledge of our children is still lacking. Most of them do not know that young marriages can be harmful to their health. Even their parents may not know about it. So, all this time, if they are going to get married, just get married. If the age is not sufficient, just ask for a dispensation.
Poverty
Poverty is a factor that causes a wide range of social and health issues. Local informants and collaborators agreed that poverty was closely linked to the phenomenon of early pregnancy and marriage in Mesuji Subdistrict. Families with low economic capacity tended to marry their daughters as soon as possible. Married daughters were the economic responsibility of their husbands and their kin. As a result, the pressure on girls’ parents was reduced. The following quote from one of the male parents who had adolescent children depicts this circumstance.
Low-income families prefer to marry their daughters as soon as possible. The financial obligation goes to her husband when a girl is married. Parents feel this is the best way to reduce the burden on the family. (third FGD)
Economic problems influenced the understanding not only of parents but also of the daughters. They decided to marry at a young age because they could no longer pursue their education and had trouble finding jobs. The parents’ weak economic circumstances made them look for ways to survive and preserve their own lives. The lack of employment opportunities and the villages’ isolated locations, far from the capital, made marriage the most practical option. One married female adolescent illustrated this condition.
After we do not go to school, we get married. We have someone who gives a living since we are married. Seeking a job here is hard while moving to the city is costly. Companies typically search for individuals with high diplomas or experience. (second FGD)
Juvenile delinquency
The next factor arising in most FGDs was juvenile delinquency. Drugs and alcohol use and premarital sex were the types of juvenile delinquency observed in the study setting. While most families in Mesuji Subdistrict lived in poor economic conditions, the level of drug use was very high. Based on informant reports, 70–80% of teenagers used drugs and alcohol from an early age. One community leader whose occupation was a village official clarified:
... the problem with drugs is serious. We might estimate that about 70–80 percent of adolescents use drugs and alcohol. (fourth FGD)
Drugs and alcohol were not only used by adolescents; they were also used by adults. Wedding receptions having music shows commonly turned into drug and alcohol parties. Conflicts sometimes occurred between attendees, resulting in acts of violence. It was not rare for the primary health center to admit patients with trauma or even bullet wounds. Poor financial conditions have forced teenagers and parents to become indebted to several parties to fulfill their drug and alcohol needs. Accumulating debts motivated them to commit crimes, such as theft and robbery. This problem is illustrated in the following information from one primary health center staff.
If there is a wedding party, we normally get trauma patients after they have been hit. There used to be someone who was shot. The cause is typically the brawling between people who use drugs and are drunk. (fourth FGD)
Drug and alcohol use, along with insufficient parental control and non-functioning effective family functions, led teenagers to premarital sexual behavior. One village official pointed out:
The problem is that there is no good example from their parents. There is also a lack of parental control. After using drugs and alcohol, they invite their girlfriends to have sex and then get pregnant. It is natural from the teenage viewpoint. They do not feel bad about it. (fourth FGD)
The above quote shows that juvenile delinquencies in Mesuji had been socially constructed. They were no longer considered as problems. Therefore, to achieve the expected changes, it was necessary to raise awareness among the local community that juvenile delinquency and adolescent pregnancy are problems. This stage was carried out at the beginning of the study, as shown in the aforementioned method.
Intervention actions to reduce adolescent pregnancy
Local collaborators and FGD participants formulated community-based actions to reduce adolescent marriage and pregnancy rates based on the identified key factors. They agreed that there must be at least two types of action: generating income to improve family welfare, and educating adolescents about sexual health. These actions are summarized in Table 4.
Advocacy
Researchers and local collaborators advocated to the Mesuji District Government about the importance of preventing adolescent marriage and pregnancy. The advocacy received a positive response from the Mayor of Mesuji District. Although this study was qualitative and could not be generalized, under similar socioeconomic conditions, it must be recognized that early pregnancy is a threat to most Mesuji District villages and subdistricts. For this reason, the findings of this study were used as the basis for Mesuji District Regulation No. 32 of 2018 regarding adolescent marriage prevention. Furthermore, the National Population and Family Planning Board appointed Wiralaga 1 as a Family Planning Village. The main aim of this Village Program is to educate people about family planning through the use of contraceptives. By the implementing the Village Program in Wiralaga 1, the contraceptive uptake is expected to increase, and the birth rate can be controlled. Although only Wiralaga 1 was designated, the programs also included the surrounding villages in the Mesuji Subdistrict, including Wiralaga 2.
Table 3: Focus group discussion participants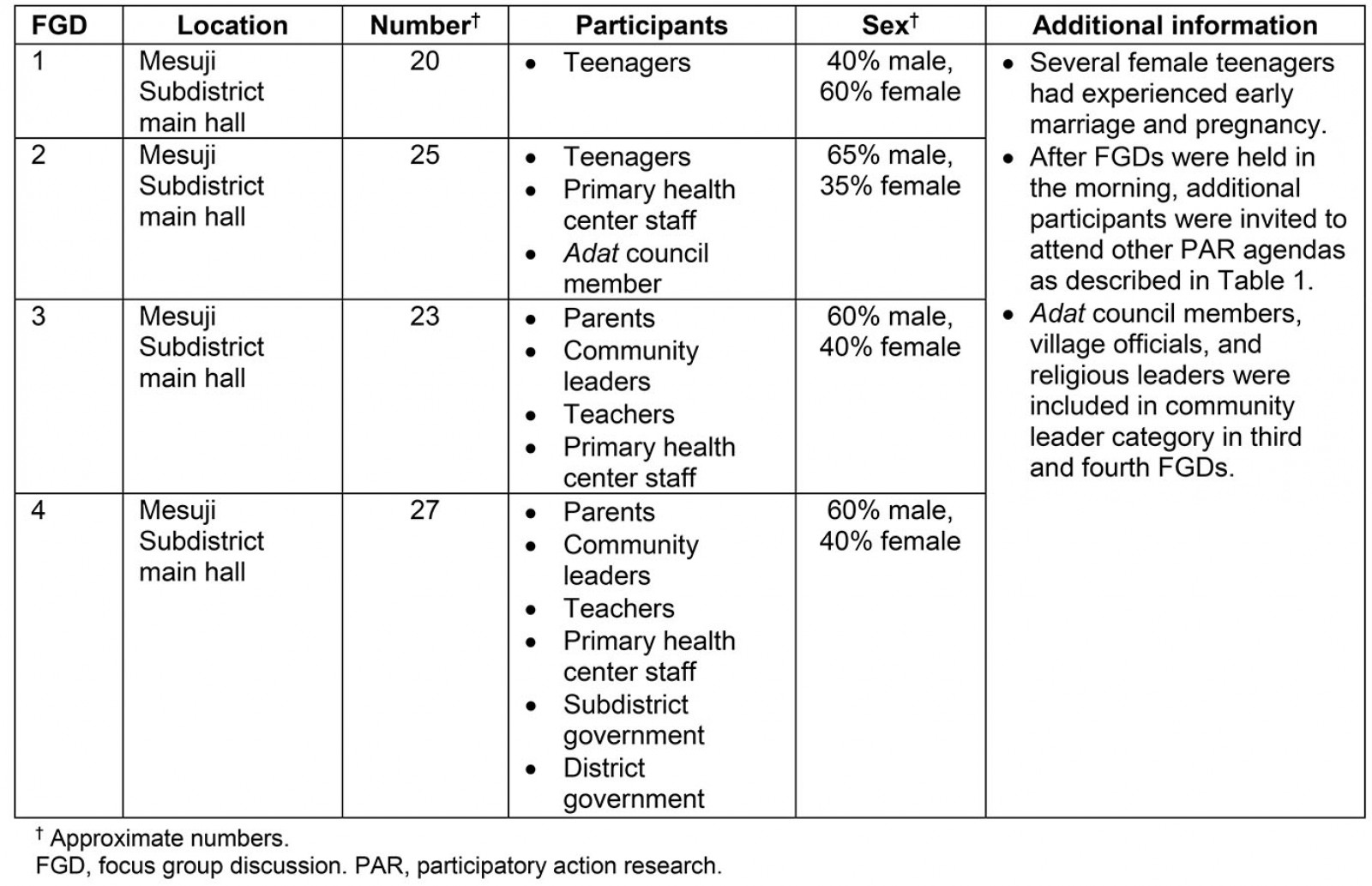
Table 4: Intervention actions for solving adolescent marriage and pregnancy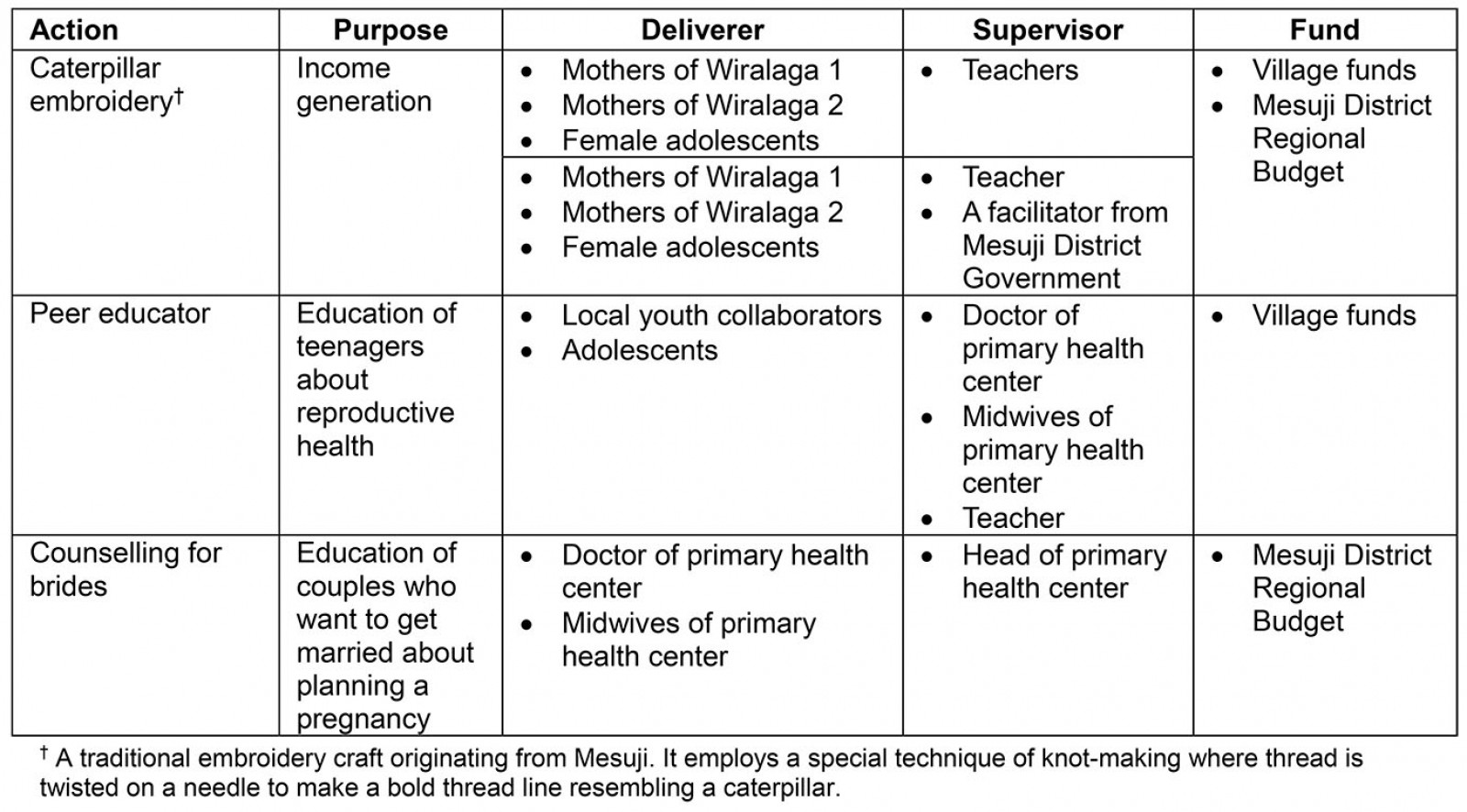
Discussion
For most developing countries, including Indonesia, adolescent pregnancy is a challenge8,24. This research has succeeded in identifying and understanding the factors contributing to adolescent pregnancy in rural Indonesia through PAR use. As shown in the conceptual model (Fig2), the determinants of adolescent pregnancy were mostly socioeconomic factors. Therefore, this research shows that social problems are revealed when an evaluation of health issues is conducted. These findings are consistent with the results of previous studies, which stated that health is influenced by various social factors, such as economic conditions, social and cultural norms, and educational attainment25,26. These results are essential because adolescents in this study setting experience significant disparities in health services and socioeconomics opportunities. Without adequate intervention derived from information by the needs and perceptions of these adolescents and the local community, the gap will continue to grow.
When social and cultural norms in urban areas develop and change quickly, they no longer apply to rural and disadvantaged areas. In these areas, social and cultural norms change very slowly and even stay the same8. The norms prevailing in society in this study considered women who chose to delay marriage to a relatively mature age as unwanted women. This perception is deeply embedded in social norms, leading to the fear that unmarried girls would have difficulty finding a partner after 20. Parents’ fear of social sanctions if daughters engaged in premarital sex, which resulted in unintended pregnancy, motivated parents to marry their daughters immediately. In societies where social and cultural norms still regard pregnancy outside marriage as taboo, this phenomenon is common. Therefore, it must be understood that for a girl in this kind of social environment, marrying at a young age is often a necessity, a taken-for-granted reality8.
Previous studies have shown that poverty is responsible for a variety of social and health problems, including teen pregnancy and parity complications in rural areas27,28. This research found that poverty was one of the main causes of girls in Wiralaga marrying and becoming pregnant at a young age. The patriarchal norms that were embraced by the Lampung ethnic group in Mesuji Subdistrict gave more responsibility to men to meet the family’s needs. As a result, girls’ marriages were seen as a means of protection from economic instability and negative stigma caused by unintended premarital pregnancy29. However, marriage is not always the best solution to poverty because the bridegroom is often unemployed or on a low income. In this situation, marriage creates new problems. A husband who is unable to meet his wife’s financial needs will be more burdened when their children are born. As a result, the family lives in poverty. Poverty is, therefore, assessed not only as a cause but also the result of adolescent marriage and pregnancy. This phenomenon was also found in other developing countries such as Lao People’s Democratic Republic and Uganda8,30.
Education as the strongest fortress against poverty, on the other hand, was a luxury for children in the Mesuji Subdistrict. Poverty, regional isolation, and limited access to good education, as well as cultural and social norms, have mutually encouraged Wiralaga’s children to drop out of school. Previous studies have consistently shown that marriage in underage girls is prevalent in remote and poor rural areas with limited access to health and educational facilities28,30-32. Specifically, low educational attainment has been associated with adolescent pregnancy33,34. This finding could suggest that adolescents with low educational backgrounds have insufficient knowledge of safe sexual behavior and the appropriate age to become pregnant30,35. The low level of education and lack of productive activities have led adolescents in Mesuji Subdistrict to juvenile delinquency. Juvenile delinquency is also suspected to be caused by the loose supervision by parents, the lack of role models30, and poor child–parent communication35. Earlier research found that juvenile delinquency is more prevalent in cities36,37. In contrast, this study discovered that juvenile delinquency also existed in rural areas. However, findings that showed juvenile delinquency as one of the contributing factors to adolescent pregnancy confirm the findings of previous studies, which indicated that juvenile delinquency and peer influence are factors that trigger an early debut of sexual intercourse and pregnancy28,30,31.
The low contraceptive use in Mesuji Subdistrict reflects Indonesia’s national condition. Indonesia’s contraceptive prevalence rate (CPR) in 2015 was 61.6012. This number is still below Indonesia’s 2015–2019 National Midterm Development Plan target of 66.0038. Hence, plenty of work is still needed to achieve the CPR target in Indonesia. Findings from previous research revealed that education level was a strong predictor for CPR39. Girls who receive more years of education tend to be more able to control birth by using contraceptives than those who have less education. In the Indonesian context, it must be understood that the government only promotes contraceptives for married couples. This policy is taken to avoid an interpretation that the Indonesian Government legalizes or encourages premarital sex. The implication of this policy is limited access to contraceptives for unmarried adolescents. One of the efforts that can be made to prevent early pregnancy is education about reproductive health by schools and staff from nearby health facilities, such as primary health centers28. Also, encouraging parents to openly discuss sexual topics would increase the probability of adolescents avoiding unsafe sexual behavior28,35. For girls who are already pregnant at a young age, this could delay the second pregnancy. Contraceptives could be used to delay pregnancy. Thus, the health risks for mothers and babies could be minimized. The low uptake of health services in Mesuji Subdistrict is typical of rural areas and is caused by an unfamiliarity with the health program and the inability to bear the expenses due to economic difficulty28,30.
The actions presented in Table 2 were the initiatives of the participants of the research. Hence, it was expected to create a sense of belonging, high commitment, and active participation from the local community. Actions generated from methodologically rigorous research and active participation from the community to achieve social change are the main components of PAR16,40. However, most PAR studies stop at the action formulation stage14,41,42. In this study, the researchers continued advocacy that targeted the local government and the community. The advocacy contents were derived from the perceptions of adolescents and the local community of Mesuji Subdistrict regarding factors contributing to early marriage and pregnancy. PAR-based advocacy is focused on grassroots empowerment and thus researchers should listen attentively and facilitate democratic cooperation rather than simply telling what should and should not be done43. Hence, PAR-based advocacy is designed to create a bottom-up instead of a top-down intervention approach. In this study, policy-makers and the target community were involved in the research process. Previous studies have indicated that this advocacy strategy is effective to encourage the formulation or change of policy regarding the issue of concern and raise awareness, as well as the active participation of the community23,43. The researchers encouraged policy-makers to use the research findings as the basis for the formulation of regional policy regarding the prevention of adolescent marriage and pregnancy, and thus produced a clear legal foundation for actions of intervention resulting from this research. By the existence of a legal basis, it is expected that the intervention program will be sustainable. Ensuring the intervention actions' sustainability is vital so that they do not stop when the study is completed. The programs initiated by the community are expected to be adopted and internalized as the local rather than the Indonesian Government’s program. Hence, the local government would be committed to routinely allocating budget, conducting routine monitoring, evaluation, and adjusting the programs whenever needed.
Strengths and limitations
The involvement of policy-makers, health service providers, and the community in the study allowed the researchers to gather comprehensive perspectives on factors contributing to adolescent pregnancy and to triangulate the data44. Additionally, the advocacy strategies employed were found to be effective in influencing the policy-makers to formulate a policy regarding early pregnancy prevention and stimulate active community participation in the study setting. However, in most studies, PAR requires some time for changes to occur as expected. This study has not been able to present measurable changes in socioeconomic conditions and people’s behavior because of efforts initiated by research participants. According to the Mesuji Primary Health Center report, the rates of adolescent pregnancy were decreasing. Before the study was initiated, there were 10 incidents of adolescent pregnancy in 2015, slightly rising to 11 incidents in 2016. When the study started in 2017, adolescent pregnancy was reduced to six incidents and in 2018 there was zero. However, these changes could not necessarily be associated with PAR.
This is worth noting as one of the limitations of the study. The second limitation is that the detailed demographic data of the FGD participants were not recorded. If the discussion participants’ demographic data were recorded, it would allow a more in-depth interpretation of the data. Third, in-depth interviews were not conducted with key informants such as community leaders. However, close consultations with policy-makers at the central (Ministry of Health and National Population and Family Planning Board), province (Province Health Department), and district (District Health Department, District Religious Affairs Department, District Social Department) levels were conducted to mitigate the research limitations and ensure the quality and validity of the findings. Hence, the results of this study can be used as a reference for policy formulation for areas with population characteristics, geographical location, and socioeconomic conditions that are similar to this research setting. Additionally, it is hoped that this study’s findings can be used as the basis for further quantitative studies.
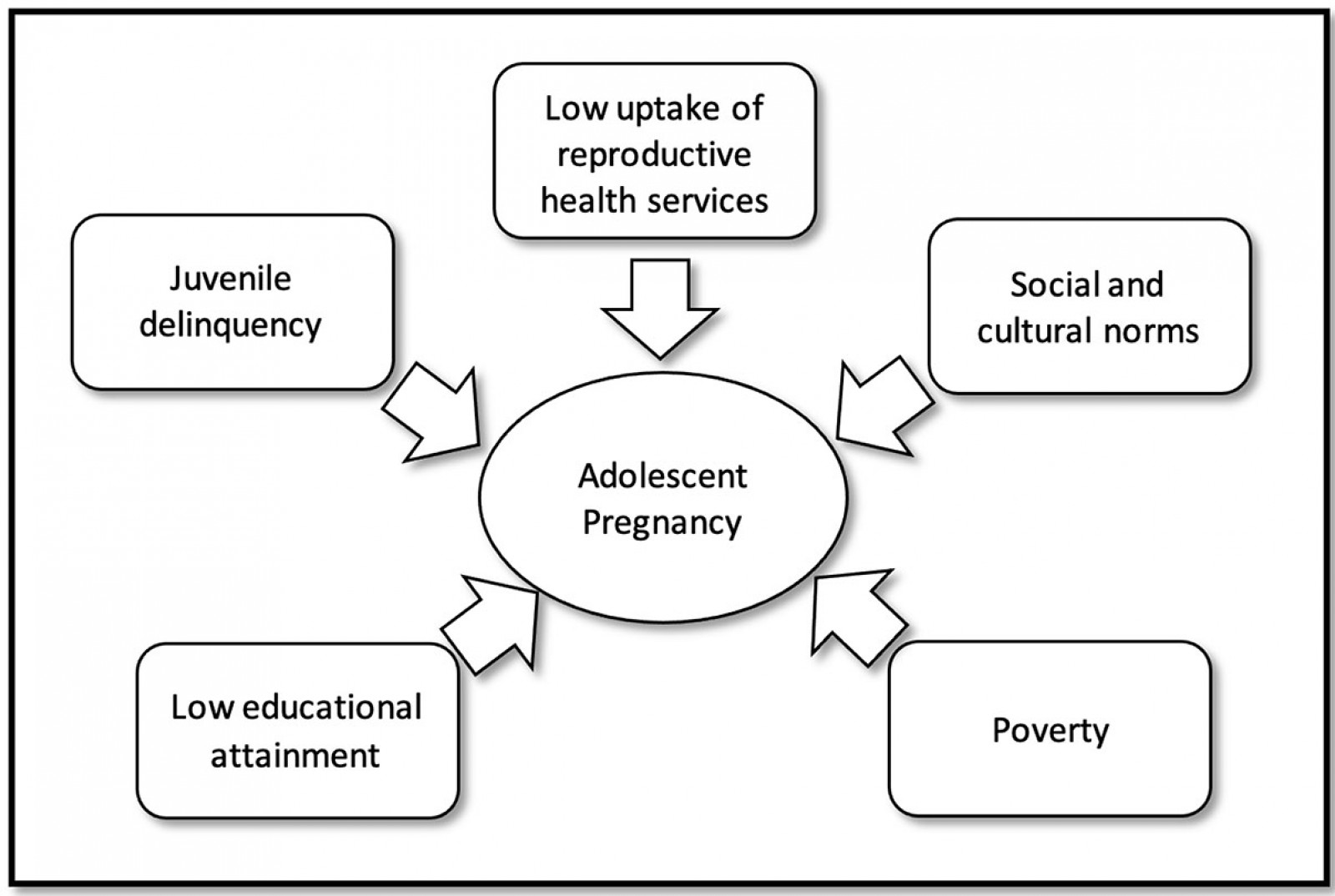 Figure 2: Contributing factors to adolescent pregnancy in Mesuji.
Figure 2: Contributing factors to adolescent pregnancy in Mesuji.
Conclusion
This study revealed that factors contributing to the occurrence of adolescent marriage and pregnancy in Mesuji were low uptake of reproductive health services, sociocultural norms, low educational attainment, poverty, and juvenile delinquency. Hence, most of the actions of intervention derived from the participants’ initiatives were intended to solve these problems. This study suggests the Mesuji District Government should continuously support reproductive health education and other intervention actions derived from this study. The youth–family development program from the Indonesia National Population and Family Planning Board could also be adopted to complete the intervention actions. Policy-makers should understand that adolescents are sexual beings. They need to be equipped with knowledge and support to protect themselves from risky sexual behavior and to delay pregnancy until an appropriate age. This research also suggests that specific context-based studies are needed to identify problems relating to socioeconomic conditions and disparities in health services for marginalized groups in rural and disadvantaged areas. At the same time, it is crucial to hear the voices of these people to make appropriate interventions that respect the social and cultural norms prevailing in the local community.
Acknowledgements
The researchers would like to thank the Director of Research Center for Humanities and Health Management, Ministry of Health of the Republic of Indonesia, for funding this research. Appreciations also go to all informants, local collaborators, the Mesuji District Government, the Mesuji Primary Health Center, the National Population and Family Planning Board, and all those who have assisted this research.
References
You might also be interested in:
2016 - Supporting nurses' transition to rural healthcare environments through mentorship
2011 - Colorectal cancer screening among rural Appalachian residents with multiple morbidities