

Context
Debriefing following a significant incident is vital for healthcare teams. It allows team members to reflect on the experience, process emotions, identify key lessons, and ultimately enhance the abilities of the team1. A growing body of research in emergency medicine supports the use of debriefing given the high intensity and high-stakes nature of the specialty2,3. However, additional challenges facing healthcare workers (HCWs) in remote isolated settings are less well described in the literature. This article reviews the debriefing literature from the perspective of a clinician working in remote emergency services and considers the potential role of debriefing in supporting HCWs given the unique and often unforeseen challenges faced.
Debriefing is a tool utilised across many different fields, including the military, aviation and health care, with clear benefits; a meta-analysis found that debriefing can improve overall team performance by 25%1. Kessler et al describe a detailed approach of how to implement debriefing within an emergency department when reviewing critical incidents, including pragmatic tips such as participants to include, and location and timing4. In broad terms, debriefs are subdivided into three types – hot, warm and cold – based on time after the incident.
A hot brief occurs immediately after the critical incident, ideally when all involved team members are available. A number of different tools have been developed for this purpose, including the STOP5 tool, which provides a clear structure to guide the team with a target time of less than 5 minutes5. Hot briefs allow recall of events, time for a break, and also an opportunity for providing psychological first aid for team members. Warm debriefs occur within minutes or hours of the incident, are still brief, and have similar intentions as hot debriefs, but occur in a slightly delayed fashion when a hot debrief may not be immediately possible for logistical reasons.
Cold debriefs are delayed by days or weeks. They are longer in length (usually 1 hour), in a private location, scheduled, and ideally run by a dedicated and trained facilitator. They allow the collation of data, case analysis, presence of external guests and other team members not able to be present for the hot/warm debrief (eg paramedics, retrieval services, and other specialist teams including pathology, radiology and support services)2. This type of debrief should have established ground rules, an agenda, a dedicated scribe and a support person in the room to provide immediate psychological first aid if required. The purposeful delay allows team members to digest the emotions and reflect on the incident, while also contributing to broader, system-wide quality improvement initiatives.
Regardless of the type of debrief, there should be a clear structure with a dedicated leader, who is non-judgemental, capable of time management, and understands interpersonal dynamics.
Issue
HCWs working in remote healthcare settings are faced with unique challenges that may impact successful debriefing and implementation of the processes described above.
Staff and time availability
One of the core elements of any debrief is the participation of staff involved in an incident. This is not usually an issue for hot debriefs because they occur soon after an incident; however, warm and cold debriefs pose challenges to participation. Many isolated regions in Australia function with less healthcare staff per capita than major cities6. For example, small Indigenous communities throughout the Northern Territory have access to experienced remote area nurses or Aboriginal health practitioners with minimal support staff – without doubt they are unrecognised heroes of the Australian healthcare system. Following a critical incident, remote services may yet face ongoing community health needs that may not allow staff participation in debriefs, particularly if their involvement would effectively require closure of the service. Similarly, participation may be further limited by the demands of continuous on call for remote staff. In small regional emergency departments, arranging a time for all members of a team to debrief is logistically difficult for several reasons: healthcare staff fulfilling multiple roles throughout the hospital/region, fly-in-fly-out staff rostering, locum staff, minimal buffer in the roster to relieve clinical duties, and fatigue management due to chronic staff shortages.
Location
In remote healthcare settings, there may be vast distances between various healthcare providers involved in patient care, including pre-hospital personnel, primary care, hospital, retrieval and referral hospital providers. This is very different to different team members assembling from multiple departments within a larger hospital. One counter-argument to this is the expanded use of teleconferencing facilities, especially in the current COVID-19 pandemic, where there has been a large uptake of this technology in health care. However, this assumes all providers have access to reliable technology and stable internet connection. Furthermore limitations do exist with teleconferencing, with loss of non-verbal cues, impaired assessment of group dynamics, sound interference, and lack of immediate support following the meeting if concerns are identified.
Social factors
HCWs who have relocated to rural and remote areas are often away from their families and other networks, hence may not have the same psychosocial support structures in place when experiencing a significant event. Consequently, HCWs frequently have their professional and social networks intertwined, as a protective mechanism to offset the degree of social isolation. However, these same protective factors may indeed become harmful in a crisis where there has been tension in the workplace, or a disagreement. This can pose a barrier to open disclosure and constructive discussion, hindering the debriefing process. Interpersonal conflict may then translate into a further distancing of locally available psychosocial supports. When frontline HCWs encounter a critical incident in this setting, there is a higher likelihood of the patient being known to a member of the team through their social networks. This amplifies the impact on staff, may lead to loss of objectivity in debriefing, and increase the need for prolonged psychological support. Despite these challenges, remote communities function as a large family in many parts of Australia, with incredible resilience and creating a sense of belonging. Local support networks may not come in the form of large formal organisations, but in the form of low-cost, high-impact gestures of kindness. In the setting of a traumatic event, simply offering to cook a meal may restore the morale of an otherwise isolated HCW.
Low frequency of critical events
Approximately 28% of the Australian population live in rural and remote areas; however, critical illness does not respect geography6. Rural and remote healthcare workers manage patients with the same severity of illness compared of those in tertiary centres, but with less frequency7. High-volume trauma centres may undertake numerous debriefs daily, streamlining and tailoring the process, and forming an integral part of the resuscitation itself. For those in isolated settings, critical illness and debriefs may occur very infrequently or even rarely. Hence, the debriefing process may be a challenging and unfamiliar process for remote teams.
Lack of access to formal training
Formal debriefing education and courses are available, but may be hard to access for rural and remote clinicians. Not only are courses predominantly run from capital cities, but accessing leave to attend these courses may be difficult due to lack of relief staff coverage. This training is crucial because debriefing is a professional skill, like any other in health care. A lack of training before embarking on a formal hot debrief may indeed lead to deleterious effects, and reduce engagement from affected staff with subsequent warm and cold debriefs.
Psychological support
As part of the debriefing process, it may be identified that members of a team need access to further support to prevent psychological trauma, and development of acute stress disorder or post-traumatic stress disorder8. Most government-run health services have access to subsidised psychology and counselling through a dedicated scheme; however, long waiting lists or no access to these services on-site may lead to prolonged trauma.
Lessons learned – alternative models of debriefing, and potential solutions
For those working in rural or remote settings, the case scenario (Box 1) may resonate closely and is unfortunately common. When a critical incident or death occurs, the effects are felt beyond the walls of the emergency department or clinic. It impacts on the entire community, outside of health care, with associated consequences and ongoing needs of the community. Each rural and remote community is unique in its community structures. Due to this, a generic approach to handling traumatic events is difficult to achieve. The principles of formal debriefing need to incorporate several stakeholders including local health services, supporting essential services (police, ambulance, firefighters), volunteers, local councils, small businesses and non-government organisations.
Debriefing needs to be adapted to the rural and remote context. It may not be physically possible for everyone involved to be present for a hot, warm or cold debrief. Hybrid models may need to be developed to suit local needs. In the current pandemic climate, there is a need to minimise large group gatherings of HCWs and adopt social distancing measures. The use of teleconference facilities can provide an alternative method for debriefing, and has been used effectively overseas in low-resource settings9. The same ground rules and structured approach should apply to the online environment, and every effort must be made to address connectivity issues for all team members.
Formalising debriefing skills into university health curriculums is another avenue we should standardise, similar to other basic competencies expected of university graduates. Including students as a debrief observer, as part of their clinical attachments, provides a key opportunity for learning. In the postgraduate medical setting, debriefing forms part of the core vocational training curriculum in those specialties that are exposed to high volumes of critical incidents, including, but not limited to the Australian College of Rural and Remote Medicine, Royal Australian College of General Practitioners, Australasian College of Emergency Medicine and the Australian and New Zealand College of Anaesthetists10-13.
Simulation is a method of teaching utilised in all healthcare disciplines to create a safe and effective environment for learners. In addition to the primary objective of the simulation (ie case scenario, procedures, skill development), the debrief is a crucial component of simulation-based learning and provides a valuable opportunity to practice, refine and standardise debriefing skills7. The benefits of simulation cannot be understated in remote healthcare settings and provide an avenue to practise debriefing regularly, promote team development and guide system changes.
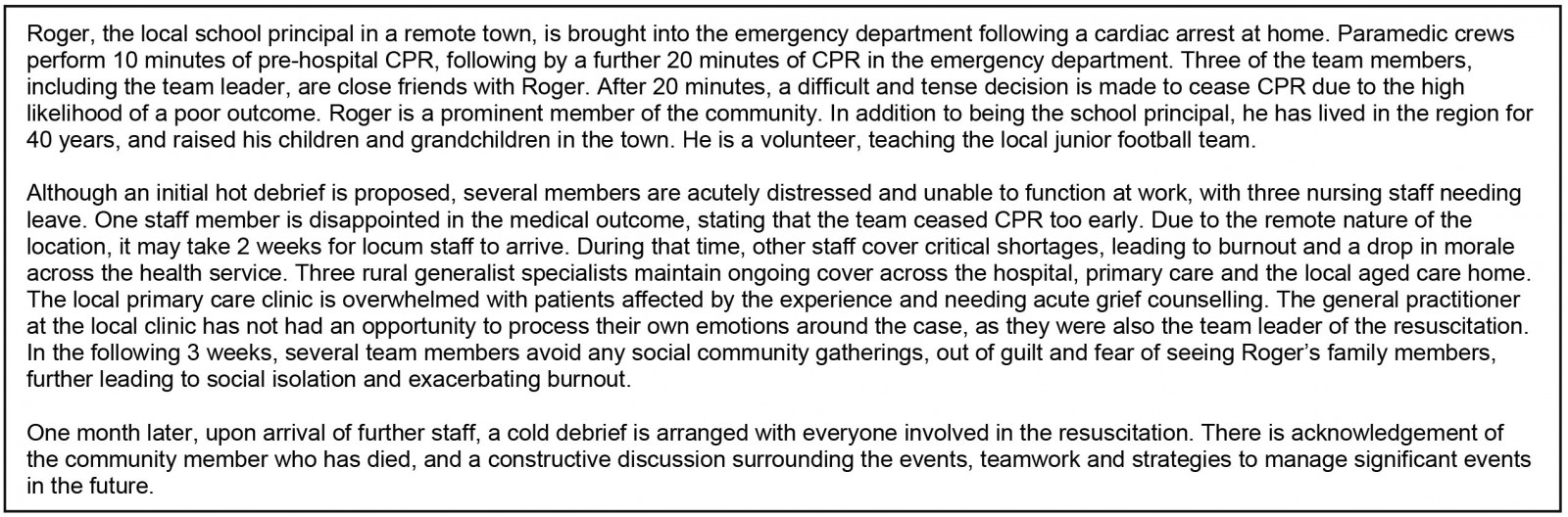 Box 1: Hypothetical case study – Healthcare worker team debriefs after treatment of a friend
Box 1: Hypothetical case study – Healthcare worker team debriefs after treatment of a friend
Conclusion
Debriefing is an essential activity following a critical incident. By understanding the provision of health care in rural and remote settings, the aforementioned strategies can be integrated accordingly, with a community-centric approach.
Acknowledgements
Thanks to the dedicated rural and remote healthcare staff around Australia who work tirelessly to support our communities; and to Dr Laksmi Govindasamy, who reviewed the original draft, has an interest in debriefing and provided valuable feedback.