




Introduction
Viral diseases transmitted by mosquitoes of the Aedes genus are a priority public health problem worldwide. Colombia is one of the most affected countries in Latin America by the presence of dengue, whose incidence, mortality and fatality rate have increased since the 1950s due to a large presence of the Aedes mosquito (more than 90% of the national territory located less than 2200 m above sea level), an intense and growing transmission, and the simultaneous circulation of the four serotypes. Some cities have been classified as hyperendemic due to the many cases reported year after year1-6. In 2022, a total of 69 497 cases were registered in the country. This figure is 46.1% lower than that of 2019 and 30.3% higher than that of 2021. According to the National Institute of Health of Colombia, this change shows an epidemic behavior of dengue in the country7.
Nowadays, there are no specific antiviral therapies against dengue and mass vaccination is not available yet. However, the way forward for dengue prevention and control involves addressing a complex disease with an integrated set of solutions that implement new approaches of vector intervention measures and vaccines in a population-based, combined with sound clinical, laboratory, and entomological, surveillance. This integrated approach requires unprecedented coordination of efforts to prevent dengue, with substantial political will, goodwill, and community participation at all levels8. For this reason, communication between the population and the technical–scientific personnel in charge of governmental control programs and actions should be fluid9-12. For decades, medical anthropology has emphasized that in order to integrate the community into tropical disease prevention and control programs, it is necessary to start from their systems of cultural meanings and representation, understanding the dimensions that establish a hierarchy of values and guide social practices related to prevention, illnesses and care13.
In Colombia, anthropological research has revealed a mismatch between the perspectives about dengue fever of international agencies and official institutions and those of people’s daily lives14-17. The role of discourse on the risk of this disease is central to this mismatch because these are configured about the specificities, knowledge and understandings found in the different perspectives.
The word ‘risk’ has changed meaning over the centuries, and its use is now quite common. In contemporary daily language, according to Lupton, ‘the term 'risk' is often used to denote a phenomenon that has the potential to deliver substantial harm, whether or not the probability of this harm eventuating is estimable’18. There are different theoretical approaches to the meaning of risk in the scientific field. In the technical–scientific approach18,19 predominant in epidemiology, which arises from methodological individualism20 and is linked to libertarian and utilitarian philosophical positions, risks can be identified and controlled by scientific measurement and calculations21,22.
From this approach, recently published research has evaluated the association between dengue risk perception, using questions about the perceived severity of the disease and the probability of presenting it in the near future, and the knowledge, attitudes and practices regarding dengue. In studies carried out in Colombia23 and Cuba24, an association was found between risk perception and knowledge about dengue, but no association was found between risk perception and intra-domiciliary practices to avoid dengue or mosquito bites. However, the association between risk perception and preventive practices25, and the mediating effect of risk perception between attitudes and dengue prevention practices26 have been reported in other investigations.
Although this approach provides valuable knowledge for feedback on dengue control programs, it does not allow for investigating how risks are constructed as social facts. At the same time, the social, cultural and political dimensions of the concept of the population are not recognized because they are reduced to the sum of individuals in the denominator of calculations15. This approach has been questioned by sociology and medical anthropology because it ignores what people do in their daily lives16,27.
Other theoretical perspectives on risk emphasize the social and cultural contexts in which risk is understood, experienced, embodied and negotiated. From a constructionist approach, knowledge about risk relates to the everyday contexts in which it occurs. Thus, instead of ‘risks’ being understood as realities outside society and culture, they are seen as meaningful groups, logic and beliefs around realities and concrete facts. In this sense, it is only possible to know and experience risks through our location in a particular sociocultural, economic and political context. This concept has become central to late modern thinking, pervading every aspect of everyday life with risk awareness. Therefore, this perspective highlights the integration of understandings and perceptions of risk and emphasizes that these often differ among actors in different contexts and bring contrary logic about the risk facing the same event18,28,29.
According to Lupton18,19,29, discourses allow the identification of meanings and sociocultural implications of risk. A discourse can be understood as ‘a delimited body of knowledge and associated practices, a particular way of giving meaning to reality through words or images’19. In this sense, discursive analyses of risk reveal the changing meanings of risk phenomena and the struggles over these meanings.
Specifically, this article focuses on analyzing the discourses on the risk of these diseases constructed by lay people of sectors with a high number of cases, community leaders, and some health officials in the control of vector-borne diseases. These three groups of actors experience different realities about these diseases, and communication between them is essential for their control. Community leaders represent a bridge between the community and the control agencies. This report is part of a mixed-approach research aimed at understanding the distribution and transmission of Aedes in a Colombian municipality (Floridablanca) with a high presence of cases of these diseases30 and the links between dengue, zika and chikungunya with sociocultural aspects of the population between 2016 and 2018.
Methods
Study area and sample size
Based on geospatial and temporal analysis of cases reported during 2014 and 2015, urban population clusters were selected in the municipality of Floridablanca that concentrated on a high number of cases of dengue and zika fever. All conglomerates corresponded to sectors of socioeconomic strata 1–4 (government classification based on the stratification of residential real estate and public services. It is a proxy for socioeconomic status in Colombia; 1 is the lowest economic resources). Ethnographic approaches were conducted in December 2016 and January 2018, periods with a high and low number of incident cases reported to the surveillance system in the municipality, respectively. Three groups of actors participated in the fieldwork: lay people, community leaders, and health officials in charge of vector disease control. The first group comprised 65 people (38 in 2016 and 27 in 2018) with a subjective experience of the illness, who manifested any illness, or who had relatives or close people with recent experience of the illness. This group of people was contacted through community leaders or by a snowball process. The other two groups of actors were made up of four community leaders from the same conglomerates and two health officials, one of them from the municipality and the other from the government department.
Data acquisition
For collecting information, semistructured and open interviews, informal dialogues and recording observation notes in the field diary (voice and written) were used. The key domains of the interview guide directed to lay people and community leaders included understandings and perceptions about dengue, zika and chikungunya, conditions that denote risk for these diseases, and practices (preventive and curative) to deal with these diseases in everyday life. The interview guide for health officials focused on the participation of residents in control measures and the reasons that explain the community’s participation or lack of participation in the control of these diseases.
The interviews were conducted in the homes or workplaces of lay people and community leaders (marketplaces, shops/miscellaneous, tire change workshops or pharmacies). The health officials were interviewed at their workplaces. With the consent of the participants, the interviews were audio-recorded and later transcribed into text files. Participants were provided information about the facilitators’ and researchers’ identities and affiliations, the aims of the research, confidentiality and informed consent issues, and the right to withdraw voluntarily. All participants gave consent before participating in the interviews and meetings.
Analysis
The information was collected until saturation of categories was achieved, having as topics of analysis the explanation of the occurrence of the diseases and the daily prevention practices. The analysis was carried out in two periods subsequent to the data collection periods, which allowed the fieldwork and analysis of 2018 to be guided by the findings obtained in 2016.
The research group used an inductive social methodology to analyze the information through open reading, coding by cycles, structural analysis and critical interpretation31. Initially, each team member coded all texts and then, in discussion meetings, the reduction and critical interpretation of categories were achieved. The information on the different categories was collected and handled in qualitative analysis matrices, using spreadsheets for systematization and relational analysis. The information was triangulated by multiple observers, theories (using theoretical framework and different approaches to risk), methods and data sources.
Ethics approval
The study was approved by the Institutional Research Ethics Committee of the Universidad Autónoma de Bucaramanga (Act. 082, 31 October 2016).
Results
The findings are presented in two categories: lay knowledge and explanations about dengue, zika and chikungunya in the discourses of the lay people and community leaders, which configure a multisituated risk that refers to the inside and outside of their homes; and the prevention practices referred by the different agents, in which a continuity of tensions between lay people, leaders and government officials can be observed.
When diseases come from outside and are uncontrollable: daily explanations of dengue, zika and chikungunya
Lay people and community leaders establish their knowledge about mosquitoes and the disease through four channels. First is the information they receive directly from hospital health personnel when they attend medical consultations. Second is the information they receive from health personnel or health officials in community activities and talks held in the neighborhoods. Third is the information that arrives through the media (television, radio and internet), which appears above all when there are disease outbreaks, and it is necessary to warn the population. Fourth is ‘word of mouth’, through the comments, value judgments and appreciation with which people share their experiences, relationships and daily lives. These channels end up configuring a notion of seriousness, attention and action against this group of diseases. In general, the bite of the same mosquito is recognized as the direct explanation of these diseases. However, this was doubtful given that most of the appreciations came from expressions such as ‘that is what I understood’ or ‘I am not sure if it is like that,’ leaving open the possibility of the existence of specific mosquitoes for each disease.
Despite these doubts, most lay people’s narratives emphasize mosquitoes’ ‘attack’ and bites as part of coexisting with them and the possibility of acquiring one of these diseases.
Although the bite does not cause alarm, its understanding distances the notion of contagion as the cause of the disease. Contagion is seen only as close contact with a sick person. The bites are understood as the imprint of the mosquito attack and are described as daily events, showing the normalization of vectors’ presence (Table 1, quotes 1–4).
Lay people are not able to explain the consequences of a mosquito bite. They do not make the relationship between the bite and a virus, but to random ways of coinciding with the infected mosquito (‘I was bitten by the infected mosquito’), and in this way, ‘the disease spreads’ or ‘spreads from person to person’. Mention was even made of a ‘poison that goes around the body’, which is acquired through mosquito bites.
The presence of mosquitoes is mainly associated with neglected spaces full of garbage, tires, foul odors, stagnant water outside the home, and abandoned lots, among others. These are identified as the main sources of mosquito proliferation and, therefore, of diseases (Table 2, quotes 5 and 6).
Only two participants from the group of lay people residents referred to specific training on dengue control in primary education or formal training by the municipality’s health secretary. One community leader, a pharmacist, described specific characteristics of the mosquito and its transmission cycle. For example, they recognized that the female mosquito is the only one capable of transmitting the virus through its bite and that it can reproduce only in clean, stagnant water.
Dengue, zika and chikungunya are explained as diseases that people do not control because they are caused outside their houses (are out of people’s hands by coming from outside and settling in the environment). This ultimately translates into specific relationships of the subjects with the environment and the diseases, showing that ‘outside’ (of the home) refers to the external and uncontrollable. In this sense, the risk discourses of lay people are linked to environmental and external conditions such as the weather and the presence of mosquitoes in the environment, especially in neglected or abandoned places outside their homes. These uncontrollable elements are linked to their living conditions, such as the unlawful nature of the neighborhood in which they live, proximity to unbuilt spaces, abandoned natural spaces, or proximity to crowded places such as parks and marketplaces. In one of the clusters, the stories refer to how ‘the area[s] is in a state of crisis because there is much construction to be done; that is, there are many unoccupied and uncared-for lots’, and most of the houses have been self-built, leaving abandoned lots with garbage or weeds.
In a traditional sector of the municipality, mention was made of the swimming pool project, which consisted of constructing two public swimming pools in the neighborhood for sports and recreational use. However, according to the inhabitants, their use was interrupted, and they refer to the municipal administration abandoning the space, which further deteriorated and became a focus of mosquito proliferation. This place refers to the absence of the State in the face of a community need (Table 2, quotes 7 and 8).
Another group of lay people’s accounts referred to rural areas as ‘natural’ sites for the presence of the mosquito, thus associating people living in these areas with a higher risk of getting sick than people living in urban areas (Table 2, quote 9).
The scenario, then, has different layers ranging from outside the home, outside the community, to the State itself, as guarantor of the environment and people’s wellbeing. In this sense, a multisituated outside is configured, translating into a multisituated risk.
Table 1: Quotes 1–4 about daily explanations related to dengue, zika and chikunguna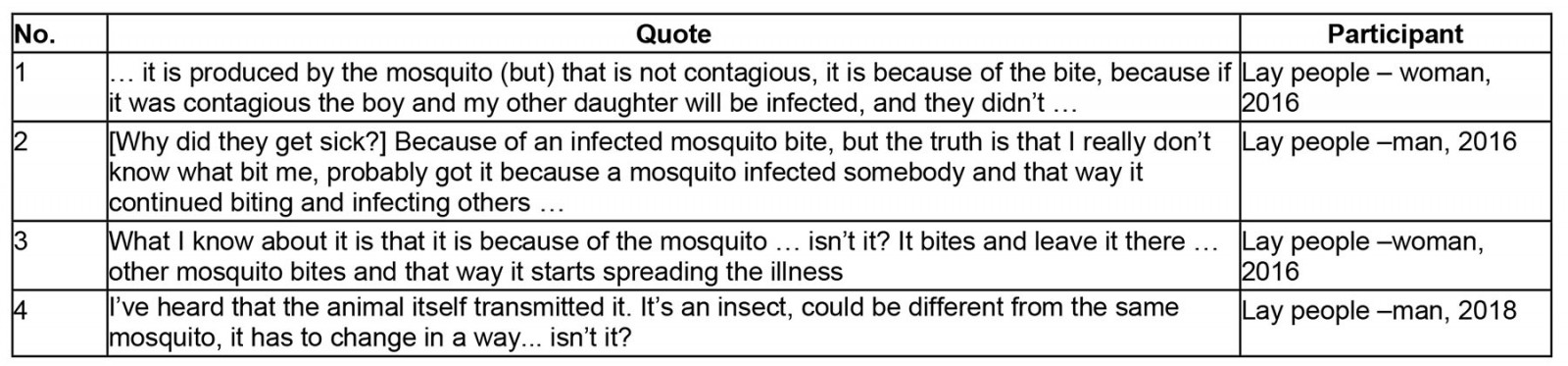
Table 2: Quotes 5–9 about daily explanations related to dengue, zika and chikunguna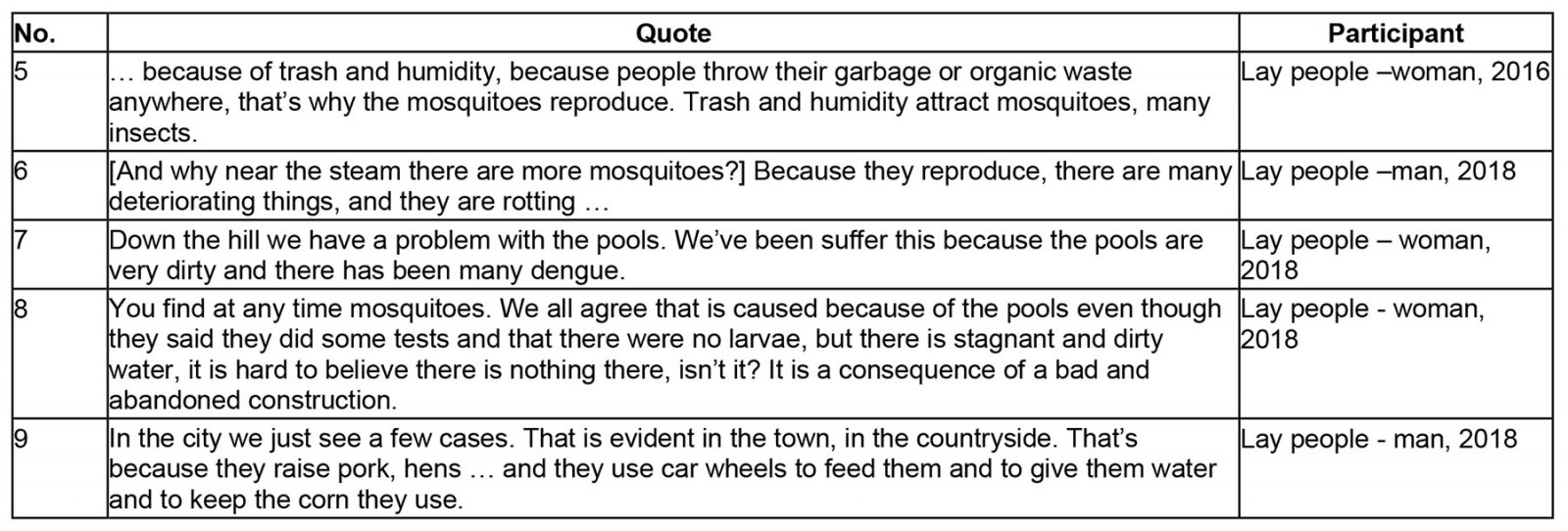
Prevention of dengue, zika and chikungunya: tensions ‘inside/outside’, ‘individual/collectives’, ‘control institutions-State/collectives’
The prevention practices for these diseases are influenced by antagonistic positions on lay and expert explanations of the presence of the mosquito, which denote constant tensions between actors that converge in daily events. The ‘inside/outside’ tension links a discourse of risk in which people confront these diseases with measures to avoid the entry and permanence of mosquitoes in their homes, thus avoiding the bites that can make them sick. This tension continues simultaneously with others that refer to different meeting places in the multisituated outside: ‘individual/collective’ and ‘collective/State’.
In order to keep their homes free of mosquitoes, lay people and leaders referred to different measures they apply, which consist of daily cleaning (including mopping with fuel oils), cleaning the sink, avoiding standing water, picking up garbage, fumigating, and using burns and incenses. The mosquito net is used only by people considered more vulnerable – children, pregnant women and the elderly – because it causes significant discomfort and it is perceived as not very esthetic (Table 3, quotes 10–12).
Lay people and some leaders perceived the ‘inside’ (ie homes or private places) as a clean and controlled environment, generating security and not representing any risk. In contrast, the ‘multisite outside’ was not perceived as under their control, individually, because it was not understood as their responsibility but as the responsibility of others, such as the State or the community, present in different levels of the outside. Here, the tensions between the inside and the outside with the individual, the collective and the State become visible. To keep the surrounding areas free of garbage, clean the unbuilt lots and, in general, all areas that for lay people and leaders may constitute a risk for getting sick, such as parks, public swimming pools, squares, and encroachment areas, leaders and lay people are demanding different measures from the ‘others’, understood to be their neighbors, the community and the State itself (Table 3, quotes 13 and 14).
Understood as a duty of the State, there is a claim of lay people and a continuous request for fumigation in the neighborhoods to keep the ‘outside’ in good condition so that the ‘inside’ is not affected. The absence of fumigation in recent years was interpreted as the State abandoning its functions, and other actions to control dengue, zika and chikungunya in the territories were also not perceived (Table 4, quotes 15 and 16).
On the other hand, community leaders expressed that education campaigns are recurrently proposed to prevent dengue and other vector-borne diseases. In these activities, lay people have a low participation. At the same time, they emphasized the continuous pressure lay people exert to achieve greater State presence in their neighborhoods, by demanding fumigation, or garbage collection, among other requests.
However, the health officials in charge of vector events control explained the various State actions and initiatives that are continuously made to control the appearance of these diseases and the presence of the vector, changing their strategy and focus from the vertical control program to the current integrated strategy, following national and international guidelines. They developed different initiatives, including communication strategies to impact behavior (Communication for Behavioral Impact (COMBI), scaling up, bottom up) and educational campaigns for the school population to achieve their active participation in vector control. These educational campaigns are accompanied by home visits that are part of the community control strategy when intervening in a case or facing an outbreak or epidemic.
According to the health officials, the desired effect of these actions is that people change their behavior and eliminate breeding sites in their homes, being clear that the persistence of dengue transmission is intra-domiciliary. Some even commented on the need to resort to coercive measures that reward or punish the presence of breeding sites in homes (Table 4, quote 17).
In addition, there was an intention to raise awareness among the population about the reasonable use of emergency services and the need to educate medical personnel on the importance of giving their patients clear information about their illnesses and how to treat them. In this way, as soon as lay people come into contact with the health system, the aim is to educate the population on the expected answer to an event related to these diseases, aiming at a ‘’responsible self-care’’ of dengue, zika and chikungunya, in addition to providing the necessary knowledge to prevent the spread of any of these diseases.
However, the general perception of the lay people about the actions organized by community leaders and the government control entities is that they express corruption, which is manifested in improper political influence in the organization of activities, the use of community spaces for political proselytism, lack of fulfillment of commitments, and hiring of non-suitable personnel to lead prevention programs, among others. It becomes evident that there is a lack of credibility in the community action boards, the health secretary, the mayor’s office and other control entities (Table 5, quotes 18 and 19).
The low participation in training or population actions proposed to control the mosquito, on the other hand, is interpreted by leaders and health officials as a ‘lack of awareness of the people’, ‘and that is why they do not participate’, emphasizing that people only request fumigations without understanding that these are no longer considered adequate and that in the different actions proposed by the control agencies, the central element is learning about mosquito control inside the homes through changes in their behaviors.
Following the explanation above, two tensions can be identified that follow up the tension between the inside and outside: ‘individual/collective’ and ‘collective/State’. In the first one, is evident a notion of people as single entities, separated from the rest of their neighbors and community, almost in an attitude of resignation, ‘it is up to you’, controlling according to them, the only thing that is under their responsibility: the interior of their homes. In other words, the participants do not perceive themselves as part of a collective. Therefore, they cannot act as part of a group to achieve common objectives, such as eradicating mosquitoes, for which they individually advocate and demand a desired presence of the State in their daily lives.
In the second tension, the individual perception of the absence of the State is contrasted with the lack of collective participation expected from the government control entities. In other words, the lack of collective participation is used to answer to the State’s limitations to carry out concrete actions to control the mosquito. However, State institutions recognize the lack of knowledge and expertise to approach communities powerfully, revealing how complex it is for people to get involved and maintain the processes beyond the periods of direct intervention (Table 5, quote 20).
Table 3: Quotes 10–14 about dengue, zika and chikunguna prevention practices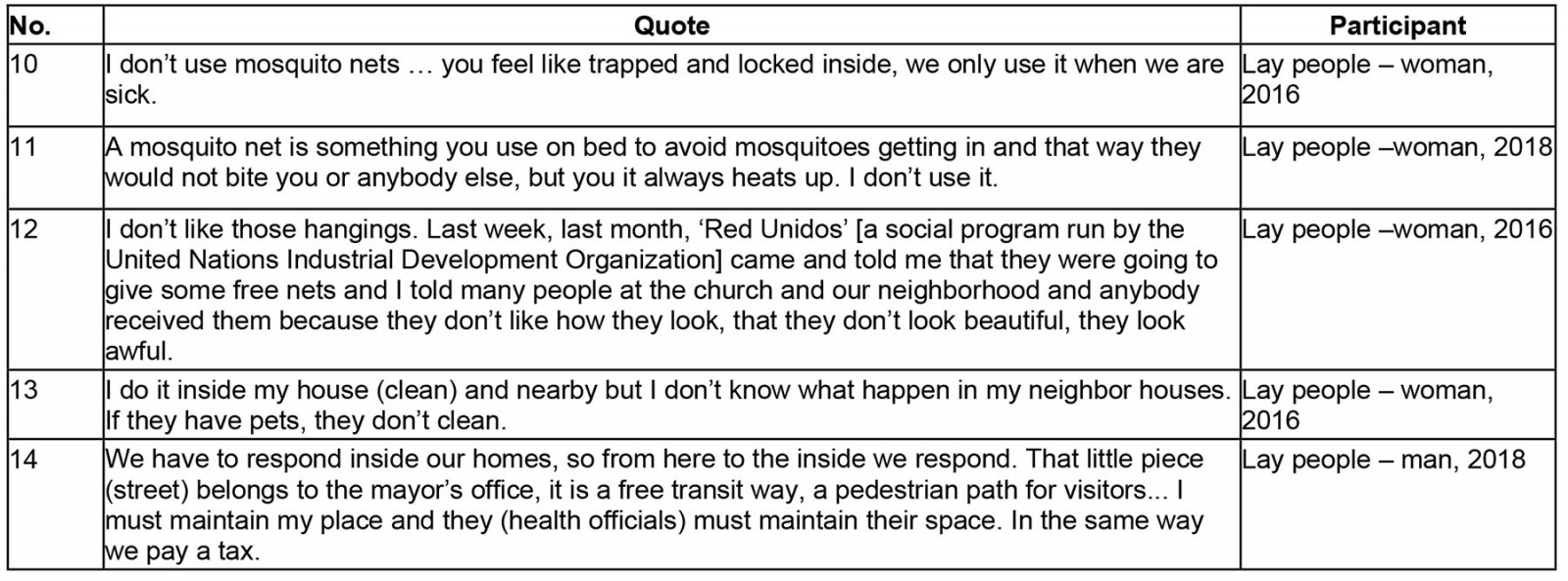
Table 4: Quotes 15–17 about dengue, zika and chikunguna prevention practices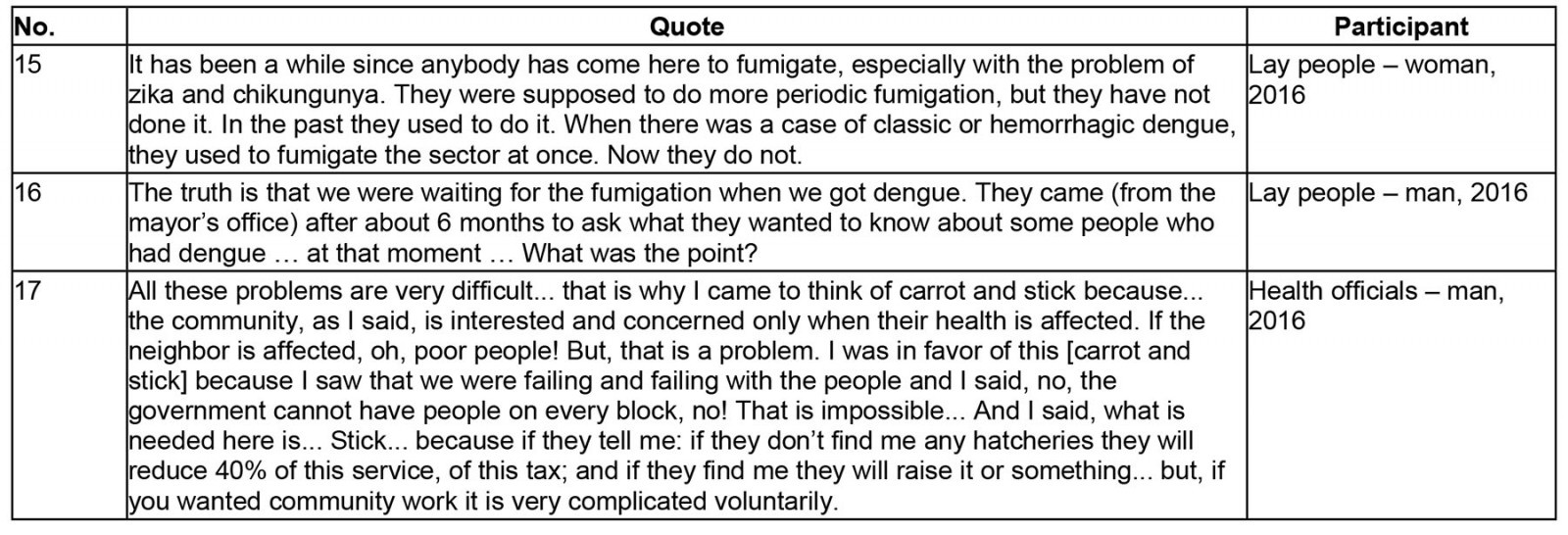
Table 5: Quotes 18–20 about dengue, zika and chikunguna prevention practices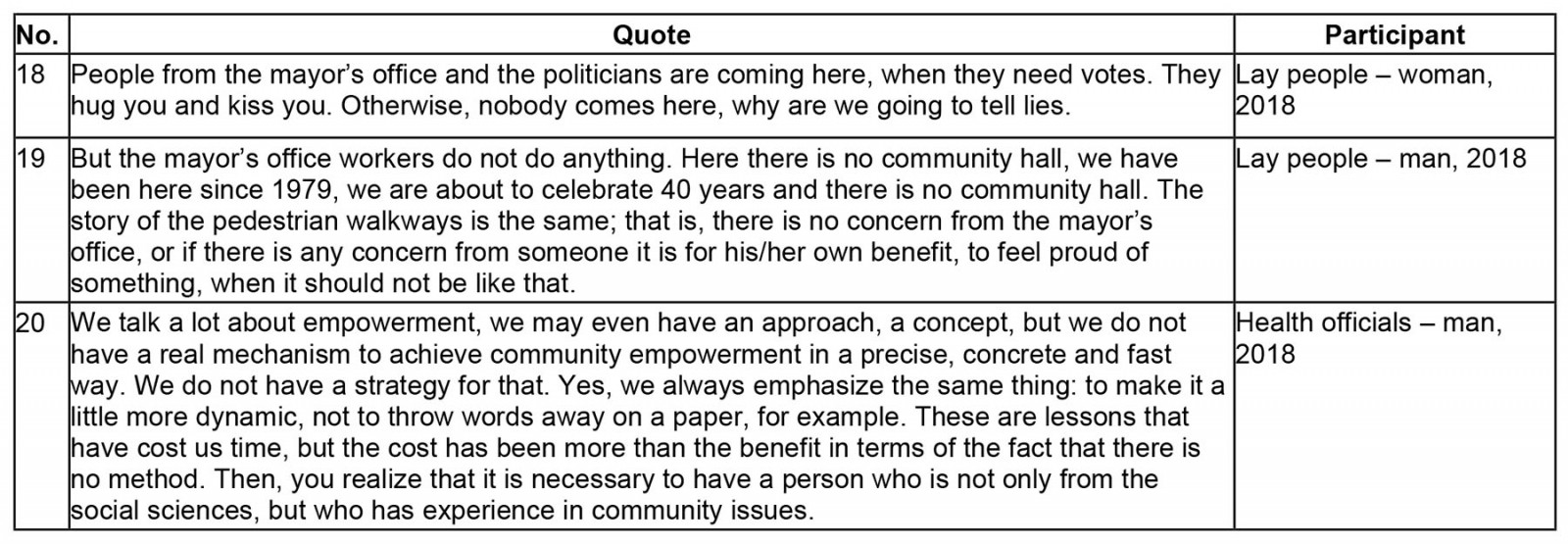
In this work, we seek discourses on the risk of diseases transmitted by Aedes mosquitoes constructed by different actors in an urban territory with a high number of cases. The findings reveal how different discourses arise, how they materialize in practices and how they can be assumed, negotiated or resisted. In this sense, for this research, infectious diseases are, at the same time, biological realities and social constructions that reflect both natural and social relationships and interactions.
Discussion
Several elements stand out in lay people’s discourses. First, the location of risk in the ‘outside’, in the external and uncontrollable areas, contrasts with the controllable and, therefore ‘risk-free’ place represented by the homes themselves. However, this differs from the biomedical notion that emphasizes vector control within homes9; that is, the place where the risk for the development of dengue, zika and chikungunya is located.
Second is the random relationship between mosquitoes and infection, which is very close to the relation described by Suárez et al about the social representation of ticks, their bites and spotted fever in the Colombian municipality of Villeta16,32. Similar to Suárez’s description, mosquito bites are part of daily life and ‘normal’ experiences. Although the bite of a mosquito is the direct explanation for the occurrence of the disease, not every mosquito produces it, only the one that is infected and with which people encounter at random. That is why it is not typical of daily situations16.
Third is the construction of risk by lay people characterized by the ‘social invisibility’ of mosquito-borne diseases, which, according to Suárez, is possible because their manifestations may be associated with other diseases (or with none in particular) or because the relationship between risk and vector may not be direct or specific in the experience of daily life16. A previous report from the same research showed how the recognition and identification of diseases transmitted by Aedes mosquitoes are mediated by cases, especially those referenced to zika and chikungunya. When the absence of cases in a territory occurs, these events are ‘forgotten’ or understood as other ways of naming already-known diseases, such as dengue. Thus, the social construction of dengue, zika and chikungunya is crossed by a fundamental tension between recognition and oblivion30.
Finally, we found that stagnant water, dirty water and dirt in general (eg garbage, waste) are defining elements for the presence of the vector. Similar to what has been found in other studies, the role of clean water in vector reproduction is unclear33. Different studies have emphasized the need to work on vector reproduction control in domestic water storage. Many of Latin America’s actions have focused on these prevention strategies, especially in contexts where such storage is justified34-36. However, many of these works are based on the association of clean water and the reproduction of the vector. Our work proposes that it is necessary to return to how people, from their daily experience, build the notions of clean and dirty water and its relationship with the generation of diseases. As stated by Vigarello37,38, cleanliness is part of the civilization process that speaks of conceptions of hygiene, absence of disease and self-care. Being clean or having clean water is related to getting rid of what paralyzes and harms. In this way, cleanliness also acquires a moral and social meaning, a sign of dignity, respect and citizenship38.
These elements are very important to consider in planning preventive and control practices by State agencies. Following Suárez16,32, if the relationship between a tick (mosquito in our case) and infection is mediated by change, the idea of prevention has no place. In Floridablanca and among the inhabitants of Villeta, it is preferable to locate the risk in places external to daily life, which are hardly under their control and, therefore, are understood as a random relationship.
Conclusion
The findings presented here on prevention measures are in conversation with those of other studies that deal with cultural conceptions of dengue. These studies have also found that the inhabitants perceive that individual and community actions are secondary to the actions of health officials or they express dissatisfaction with the role of the government in the management of garbage, insecticide spraying and actions against mosquito breeding sites39-41. This research also shows that for the inhabitants, the risk is located on the ‘outside’, and tensions are identified involving the actions of ‘others’, from neighbors to State institutions, in this way configuring the inside–outside binary relationship.
The image of the State is constructed based on the daily relationship that people have with institutions. Perceptions of these institutions play a key role in the construction of risk42,43. Thus, for example, fumigations or garbage collection and street cleaning campaigns mark the presence of State institutions and represent concrete efforts to mitigate the risk of vector-borne diseases. By not identifying the presence of the State materialized in this type of action, the spaces outside are configured as high-risk places.
Thus, the main point is to discuss the relationships of trust and information disclosure built in the encounters between citizens and the State. Trust can be understood as the support that people have to delimit the scope of the actions carried out by State institutions42. In the context of this research, it is identified that there is distrust in the State’s capacity to mitigate the risks that people located on the outside.
In this way, the construction of risk by lay people responds to a judgment about institutional behavior, in which risk is not only related to a representation of the disease but also to the management and presence of State institutions in daily life. On the other hand, the institutional framework implements vector control strategies based mainly on epidemiological research. It proposes behavioral changes44 to help make ‘the communities’ healthier, based on education and information dissemination campaigns, because according to their discourse, the responsibility for prevention is in the hands of each inhabitant.
These positions configure a multisituated risk through entrenched places and actions. First, for the State, the problem is inside the homes, which are in the charge of the people. Therefore, its function is to teach them to preserve the inside free of risk. That is why risky behavior is often considered careless and irresponsible and, consequently, labeled as deviant. As Vigarello38 states, health risks are the face of dispersion, disorder and incoherence.
Second, for people, the problem is outside, where the State should be present, but in its absence, the preventive actions taken by lay people in their homes are understood as isolated efforts. In this sense, risk logics are evident that are opposed to each other and translated into expectations of the other.
The above evidence is a dissonance between the constructions of risk discourses, which affect how State institutions think of prevention and control. According to Kelly and Barker45, six frequent errors are identified in attempts at policies aimed to change the behavior of populations: thinking that people can change their behaviors by following their common sense; assuming that people lack in-depth understanding when confronting diseases, and therefore it is only a matter of informing; assuming that information alone will drive changes in behaviors; believing that people only act rationally when facing health and wellbeing matters; assuming that people act irrationally because they do not follow healthy recommendations, without taking into account the logics or contexts behind people’s behaviors; and believing that it is possible to accurately predict people’s behavior, although differentiated population patterns are observed.
The background to these mistakes is the absence of dialogue between actors (institutional, community and individual) facing a typical situation; for example, the prevention of vector-borne diseases. From the perspective of the social construction of risk, prevention requires a dialogue between actors based on recognizing the other and the configurations of risk constructed in their daily lives. This implies reconfiguring the vertical relationship between ‘health experts’ and the general population, considering that the presence of experts and how knowledge is disseminated is key to how people configure their discourses on risk46.
In this context, it is necessary to assume the concept of the population with a more social and historical character. This requires overcoming its statistical vision as a sum of individuals or homogeneous groups occupying a territory. As stated by Arias Valencia21, quoting German philosopher Jürgen Habermas, the population is the place of social interactions and relations, where people construct themselves and build the human, the social and the political. In these interactions, they construct their reality, configure and give meaning to their social practices, health, illness and wellbeing.
In this sense, working with communities means going beyond working on ‘groups and populations at risk’ or on ‘individual behaviors’. As Cardona47 states, it is a matter of working with people and actors who have their ways of giving meaning to what they live and do. From these reflections, it is necessary to consider participation as places of encounter and recognition of others, understanding that multiple subjectivities, temporalities, spatialities, determinations, inequalities and power relations cross health-related practices.
To achieve such an approach, it is necessary to apply new theoretical and interpretative frameworks that allow us to see the complexity of the ways of acting, feeling and thinking related to health. This is possible thanks to the integration between social sciences and health sciences approaches that allow a large toolbox to, as stated by Hahn and Inhorn48 and Cortés-Garcia49, facilitate the dialogue of knowledge, the recognition of the relativity and complexity of it, and local knowledge. These elements can visualize the needs felt by the population and broaden the reductionist views on the processes of health and disease.
Funding
This study receive funding from the Universidad Autónoma de Bucaramanga and the Universidad del Rosario.
Conflicts of interest
The authors report no conflicts of interest.