




Introduction
An accelerated demographic transition has been observed in Brazil, mainly from the 1970s onwards. However, this process has not occurred homogeneously throughout the country. The aging rate in the South and Southeast regions was almost double the rate for the North region, which constitutes most of the Brazilian Amazon1,2. An increase in demand for services related to the aging process is expected, especially within the public health network, due to the increased burden of chronic diseases, which have a high occurrence with advancing age3. Determined by need, the use of health services by the elderly population can be considerably greater than that observed among the general population, especially for hospital admissions, but other barriers related to other levels of care may represent difficulties in accessing health services, especially for the most vulnerable populations, such as those living in rural areas4.
In Brazil, populations living in rural areas generally face greater difficulties in accessing health services and have poor health conditions when compared to urban populations5. The care network is centered on primary health care (PHC), with family health as the main strategy for organizing care and expanding access, through the work of teams responsible for populations in specific geographic areas, where individual and collective actions are carried out on an extended and continuous basis6. Barriers to access may be related to the characteristics of health systems and services, the availability of services and their geographical distribution, the availability and quality of human and technological resources, financing methods, the care model and information about the system, which are particularities of provision that impact access7.
Low physical performance is identified among the elderly, mainly due to the degradation of physical functions, such as decrease in the function of the musculoskeletal, cardiorespiratory and nervous systems, a condition that can prevent the elderly from performing their daily activities effectively8,9. Thus, the assessment of physical performance in the elderly population can help delineate the interventions aimed at this population, providing crucial information for determining the risk of future dependence, the worsening or diagnosis of chronic diseases, the risk of falls and other aspects of morbidity and mortality10.
During aging, there is a decrease not only in the number of muscle fibers, but also in their trophism. However, because this loss, to some extent, is part of senescence, it became necessary to better define the term ‘sarcopenia’. Thus, the European Working Group on Sarcopenia in Older People defined sarcopenia as a syndrome characterized by the progressive and generalized loss of skeletal muscle mass and strength11. This is the most accepted concept today, and to improve the accuracy of the diagnosis the adoption of means to measure muscle mass, strength tests and muscle performance tests was proposed. This definition is appropriate for differentiating muscle loss from its systemic repercussions; that is, the moment when the physiological becomes pathological.
In this context, public health policies aiming to ensure comprehensive care for the entire population have given greater visibility to a segment of the population hitherto neglected by public health: elderly people with a high degree of functional dependence12. In view of the above, the importance of conducting studies on the physical performance of elderly people living in riverside rural areas emerges, as well as analyzing the influence of sarcopenia and functional loss on the use of health services in socioeconomic and environmental contexts that are little explored. The aim of this study was to describe and test the association of sarcopenia and physical performance with PHC attributes and the use of health services by elderly people living in rural riverside areas in the Amazon, Brazil.
Methods
Study design
This cross-sectional observational study was carried out in nine riverside locations located on the left bank of the Negro River, in a rural area of the municipality of Manaus, Amazonas, Brazil.
Area and study population
The selected communities belong to four different micro-areas defined by the Municipal Secretary of Health of Manaus, covered by a single river family health team, which serves the rural localities on an itinerant basis, through monthly trips in a river mobile unit. The only team professionals residing in the territory are the community health workers (CHWs). A more detailed description of the service offered to these locations was presented by Garnelo et al13. In the most recent demographic census, the proportion of elderly people in the rural area of Manaus was 5.0%, with an increase of 1.5% from the previous census14.
Nine locations with the largest population were chosen to be part of the study: Nova Jerusalem, Nova Canaã and São Francisco (Mipindiaú area); São Sebastião do Cuieras and Nova Canaã (Cueiras area); Santa Maria, Pagodão and Chita (Santa Maria area); and Bela Vista do Jaraqui (Costa do Arara area). All these communities are accessible only by river transport and are located within reserves of sustainable development, in which traditional populations live in a regime of sustainable use of natural resources. The travel time to the nearest location included in the study by regular river transportation is 4 hours from the urban area of Manaus. Figure 1 illustrates the territory covered by the basic river health unit, showing the five micro-areas under its responsibility.
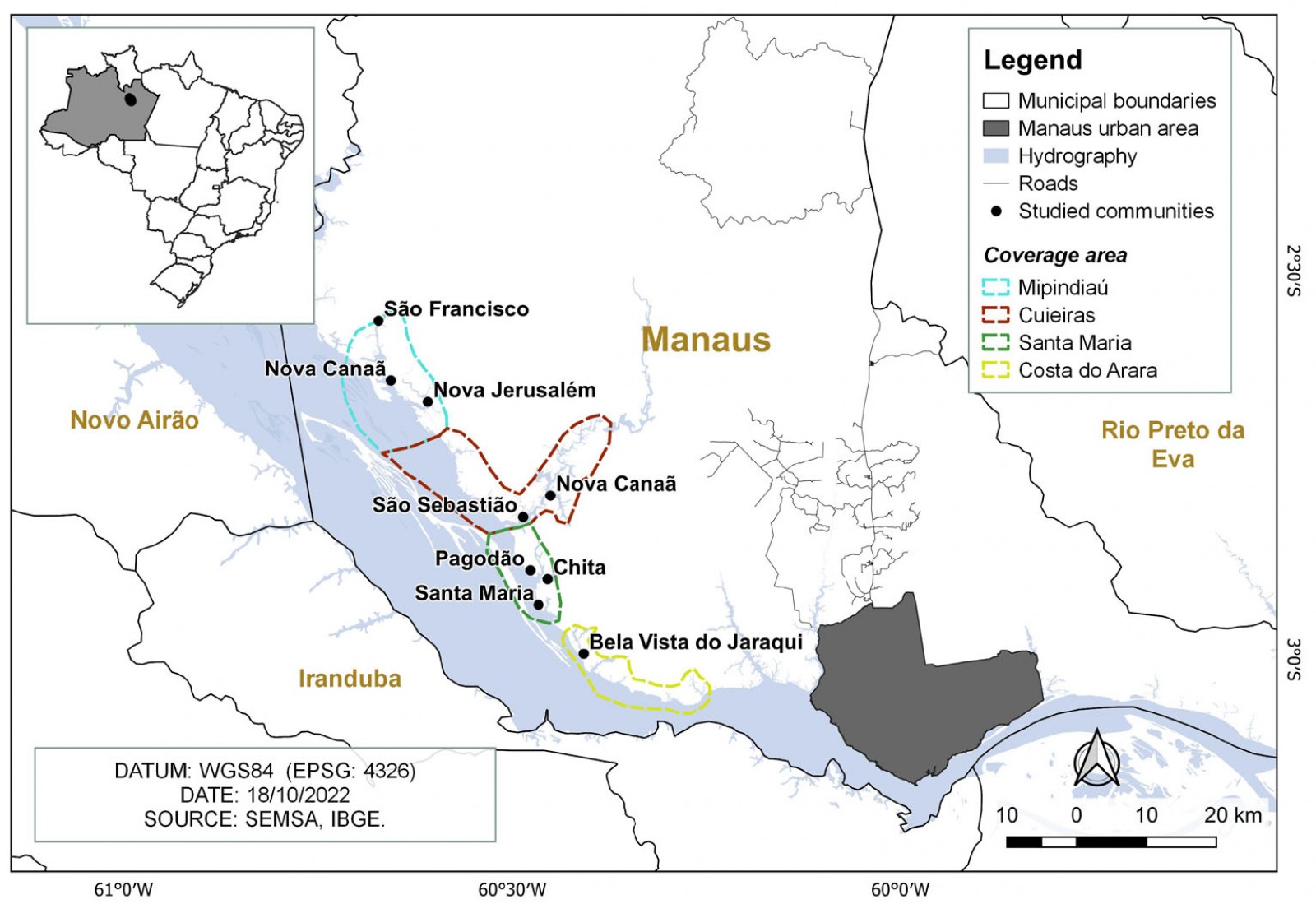 Figure 1: Riverside rural locations covered by the study – Manaus, Amazonas.
Figure 1: Riverside rural locations covered by the study – Manaus, Amazonas.
Population and sample
All residents aged 60 years or older, of both sexes, residing in the nine locations selected for the study were included in the study. Bedridden elderly people or those who had some temporary or permanent physical limitation that did not allow adequate assessment of physical performance at the time of evaluation were excluded. The Verbal Fluency Test (VFT), category ‘animals’15, was applied as a method of cognitive assessment of the elderly, initially planned as a potential eligibility criterion. However, despite the fact that 21 individuals obtained a low score on the VFT considering their level of education (16.3% of those who had not completed elementary school had a low score on the VFT, as well as 4.3% of those who were illiterate), it was decided not to exclude any of the participants given the characteristics of the study population, and to include the score on the VFT as an independent variable in the regression models. The estimated number of participants, based on the health service registration data provided by the CHWs, was 100 elderly individuals. Based on this population size, a prior analysis was made for computer-achieved power using software Stata SE, v15 (StataCorp; http://www.stata.com), considering α=0.05, effect size f2 of 0.12 in a model with five covariates, and estimating a loss of up to 10% (n=90). The calculated power was 90%. For the multiple logistic regression analysis, the calculated power was 80%, considering α=0.05, squared multiple correlation between the predictor variable and all other variables in the model of 0.2, probability of 0.4 that the response variable equals 1 when the predictor is at the mean and odds ratio (OR) of 2.0 (Stata powerlog command).
Data collection
Data were collected from April to June 2021 through a questionnaire that covered sociodemographic questions and characteristics related to the health service, as well as through the application of specific tests to assess sarcopenia and physical performance. The data collected were recorded on smartphones through the Research Electronic Data Capture (REDCap) application, used to create and manage surveys and databases, allowing field data collection without internet access, also capturing the geolocation of each household. Prior to the main study, theoretical and practical training was carried out, in addition to a pilot study for the training of researchers, in a controlled environment (within the institution), including 19 adults and elderly individuals. The evaluation of the reproducibility of the scores of the applied scales through the intraclass correlation coefficient showed good reliability of the measurements in the calibration (>0.75). A pilot study was also carried out in a rural riverside community close to the urban area of Manaus to reproduce the conditions of collection in the field.
Study variables
Socioeconomic and demographic data were collected with questions about age (years), sex (male/female), self-reported race/color (white/black/brown/indigenous), occupation (retired or pensioner/agriculture or pisciculture or extractivism/activity linked to trade or services or tourism/domestic activities/civil servant/unemployed), education (unlettered/incomplete elementary school/college or graduate degree), family income (reais), as well as related to the physical characterization of the home (predominant material on the floor, walls and roof of the home), water supply (artesian well river/stream/lake protected source/rain collection/other) and electricity (no/yes, regular/yes, but discontinuous), and disposal of waste and garbage produced at home (collected by cleaning service/placed in the community/buried or burned/other). The distances from the households to the health facilities and to the anchorage sites of the river mobile unit were calculated according to the travel path along the rivers or within the communities.
The health conditions of the elderly were also evaluated, including self-perception of general health (very good/good/regular/bad/very bad), limitation of daily activities in the previous 2 weeks (no/yes), reported diagnosis (no/yes) of systemic arterial hypertension (SAH), diabetes mellitus (DM), stroke, chronic low back pain (CLBP) and limitation due to chronic conditions (no limitation/a little bit/moderate/intensely/impedes daily activities), as well as aspects related to the use of health services. To assess PHC attributes, the Primary Care Assessment Tool was used, in a reduced version validated for Brazilian adult users (PCATool–Brazil)16. The PCATool–Brazil allows us, through interviews at home or in the health services, to identify aspects of the structure and process of the services that require reaffirmation or reformulation in the search for quality, both for the planning and for the execution of PHC actions14.
The reduced version of the adult PCATool–Brazil contains 23 items divided into 10 components related to PHC attributes. Based on the study objectives, five components were used: degree of affiliation with the health service (A), consisting of three items (A1, A2 and A3); first contact access – utilization (B), consisting of one item (B2); first contact access – accessibility (C), consisting of two items (C4 and C11); longitudinality (D), consisting of four items (D1, D6, D9 and D15); and coordination – comprehensiveness (E), consisting of four items (E6, E10, E11 and E13). The scores were calculated based on the responses to the items, in which the interviewee specifies his/her level of agreement for each item with four possible answers (1 = ‘definitely not’; 2 = ‘probably not’; 3 = ‘probably yes’; 4 = ‘definitely yes’). After recoding the inverse items, the score for each attribute was calculated by averaging the items, which was then transformed into a scale ranging from 0 to 10, according to the following equation: [obtained score – 1 (minimum value)] × 10 / 4 (maximum value) – 1 (minimum value). The overall score was calculated using the average score of the components evaluated. Higher scores indicate a better orientation of attributes for PHC17.
Physical performance was assessed using the Short Physical Performance Battery (SPPB) scale, translated and adapted for the Brazilian population18. The instrument is composed of three physical tests that evaluate, in sequence, static balance while standing; gait speed in habitual step, measured two times in a determined round trip; and, indirectly, muscular strength of the lower limbs through the movement of getting up from a chair and sitting on it five consecutive times, without the help of the upper limbs. The score for each test varies on a scale from 0 (worst performance) to 4 points (best performance). The SPPB total score was obtained by adding the scores of each test, ranging from 0 (worst performance) to 12 points (best performance). The score was also presented in a categorized way: 0–3 points, disability or very poor performance; 4–6 points, low performance; 7–9 points, moderate performance; and 10–12 points, good physical performance19.
The application of the Sarcopenia Formulary scale (SARC-F), validated and adapted to the Portuguese language20, was carried out, which consists of a questionnaire with objective questions allowing us to determine the level of difficulty perceived by the individual for five components: strength, assistance in walking, getting up from a chair, climbing stairs and falling. Each of the five components assessed was scored on a scale of 0 to 2 points (0 = ‘no difficulty or no falls in the past year’; 1 = ‘some difficulty or 1 to 3 falls in the past year’; and 2 = ‘very difficult/unable or 4 or more falls in the past year’). Calf circumference (CC) was measured with an inextensible measuring tape (accuracy of 1 mm) in the largest volume of both legs with the elderly person seated in a chair with the leg flexed at 90º. The highest CC measurement was used and muscle mass was considered low if ≤34 cm for men and ≤33 cm for women21. To assess sarcopenia, the SARC-CalF was used, which comprises the five items of the SARC-F plus the CC. The CC received a score of 0 in the absence of low muscle mass and a score of 10 when the presence of low muscle mass was verified. A total score (SARC-CalF) ≥11 points (maximum of 20) was considered suggestive of sarcopenia22.
To assess handgrip strength, a Saehan dynamometer (Saehan Corp., MASAN, Korea) was used. It has two parallel handles, one fixed and the other movable, which can be adjusted in five different positions, providing an adjustment to the size of the patient’s hand. The elderly person remained seated in a chair with one arm adducted and in neutral rotation and with the elbow flexed at 90º. At the beginning of the test, the needle was placed in the zero position. At the voice command of the researcher, the elderly person had to exert maximum force to bring the two rods closer to the device. Three measurements were taken for each hand with a rest interval of 1 minute between them, the dominant arm being identified and the highest value obtained used for the analyses. The reference values used for decreased handgrip strength were <33.4 kg for men and <18.6 kg for women23.
Data analysis
After collection, the data were exported directly by REDCap into database files of the Stata SE program. For the purposes of data analysis, descriptive statistics were applied using simple and percentage frequency, as well as measures of central tendency (mean) and dispersion (standard deviation). After the initial descriptive analysis of the data, the association between sarcopenia and the physical performance of the research participants was evaluated, as well as clinical and sociodemographic characteristics, with service utilization outcomes (having had a medical consultation in the previous year – dichotomous outcome) and with the total score and evaluated domains of the PCATool–Brazil (continuous outcome). The analyses were conducted using hierarchical logistic regression for the dichotomous outcome of the use of services, and hierarchical linear regression for the continuous outcomes of the PCATool–Brazil (total score and each of the domains). In model 1 the sociodemographic variables were inserted, and the clinical variables were inserted in model 2. Variables with p<0.20 were kept in the models. The significance level adopted for the analysis was 5%.
Ethics approval
The study was approved by the Human Research Ethics Committee at the Universidade do Estado do Amazonas (CAAE no. 4514220.1.0000.5016). The research participants received and signed the free and informed consent form, being informed about the research objectives, risks and benefits, and invited to participate in the study.
Results
A total of 98 residents (55.1% men and 44.9% women) from evaluated rural riverside localities, aged 60 years or older, were included in the study. The mean age was 70±7.4 years, ranging from 60 to 96 years. The average number of residents per household was 3.16 and the average monthly household income was R$1662.00±1089 (A$415.00±272.25). Table 1 describes the household, socioeconomic and demographic characteristics of the sample.
Table 2 presents the results related to health conditions, self-perception of health, limitation in daily activities due to health problems, physical performance assessment, handgrip strength and sarcopenia of the evaluated elderly people. Among the elderly interviewed, self-reported SAH was the most prevalent chronic condition (54.1%); 21.4% reported a medical diagnosis of DM, 12.2% had already had a stroke and 53.1% reported having CLBP; 45.2% of the elderly with SAH reported some limitation in their daily activities imposed by the chronic condition, 42.9% with DM, 36.4% of those who had suffered a stroke and 46.2% of those who had CLBP. According to the SPPB, 52.5% of the elderly participants had low or very poor physical performance. In addition, we found that 50.5% of the evaluated individuals (56.8% of the women and 44.4% of the men) had decreased palm strength. The mean handgrip strength was 18.4±6.8 kg for women and 32.9±10.6 kg for men. About 29% of the sample (32.6% of women and 25.9% of men) were identified with suspected sarcopenia.
Table 3 presents the results related to health services use and access by the elderly participants and the evaluation of PHC attributes through the PCATool–Brazil scale scores. Approximately 21% of the interviewees considered it difficult or very difficult to access the health unit and 55.1% traveled to the unit using boats. When asked about their last consultation, 79.3% reported having done it through the CHW. Most of the elderly participants rated the most recent service as good or very good. When asked about referrals and scheduling an appointment with a specialist, 59.8% reported that the appointment was made by the health unit and the user was informed at a later time. The main health service they used to seek care was the one available in the community itself (73.5%), which includes the basic fluvial health unit and physical health support units, with the elderly traveling an average of 2.3±3.1 km from their homes to the basic fluvial health unit stopping places. Most elderly people said they had seen a doctor in the previous 12 months (74.5%). The evaluation of the PCATool–Brazil general score and its attributes showed that affiliation, utilization and longitudinality were the most PHC-oriented domains, with the attributes accessibility and comprehensiveness showing lower scores.
Handgrip strength and total SPPB score were associated with the use of health services, although in a divergent way. The likelihood of medical consultation in the 12 months prior to the interview was higher among the elderly with reduced handgrip strength (OR=3.21; 95%CI=1.07–9.61; p=0.037); however, it was also higher among the elderly with better physical performance (OR=1.37; 95%CI=1.03–1.81; p=0.028) (Table 4).
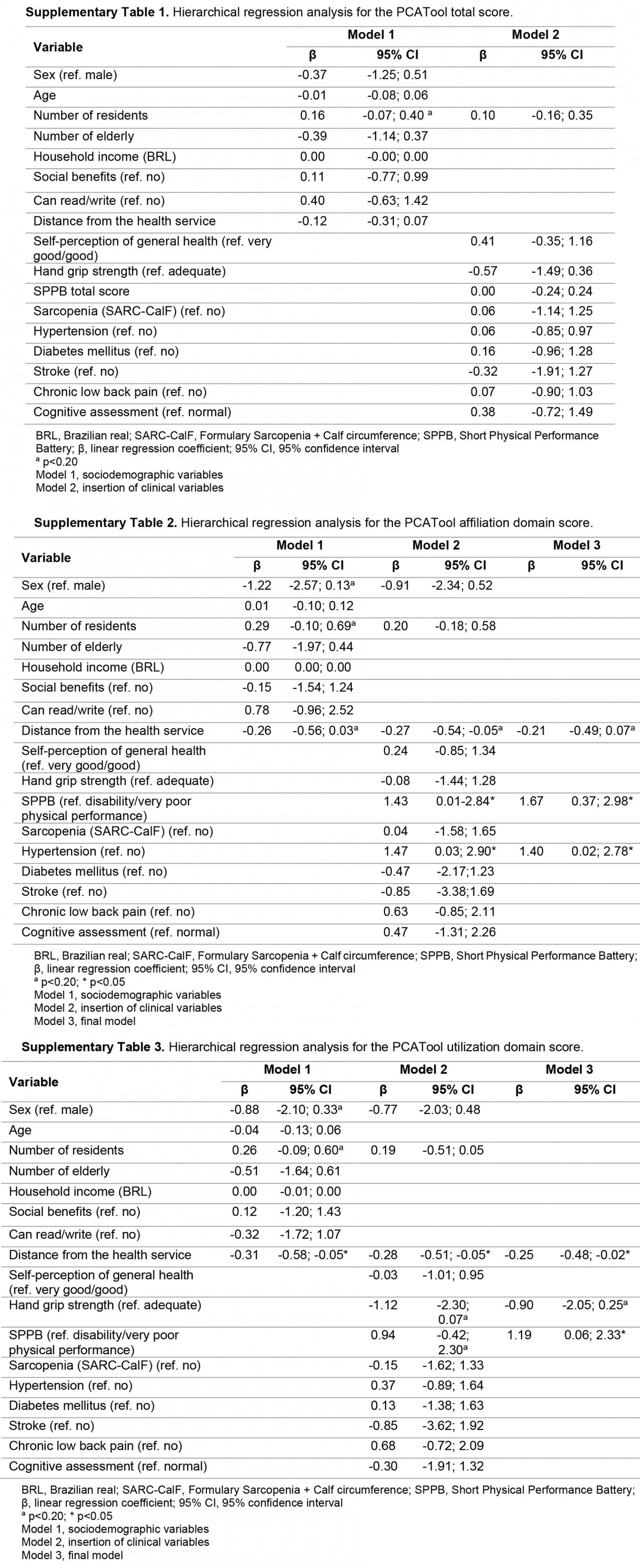
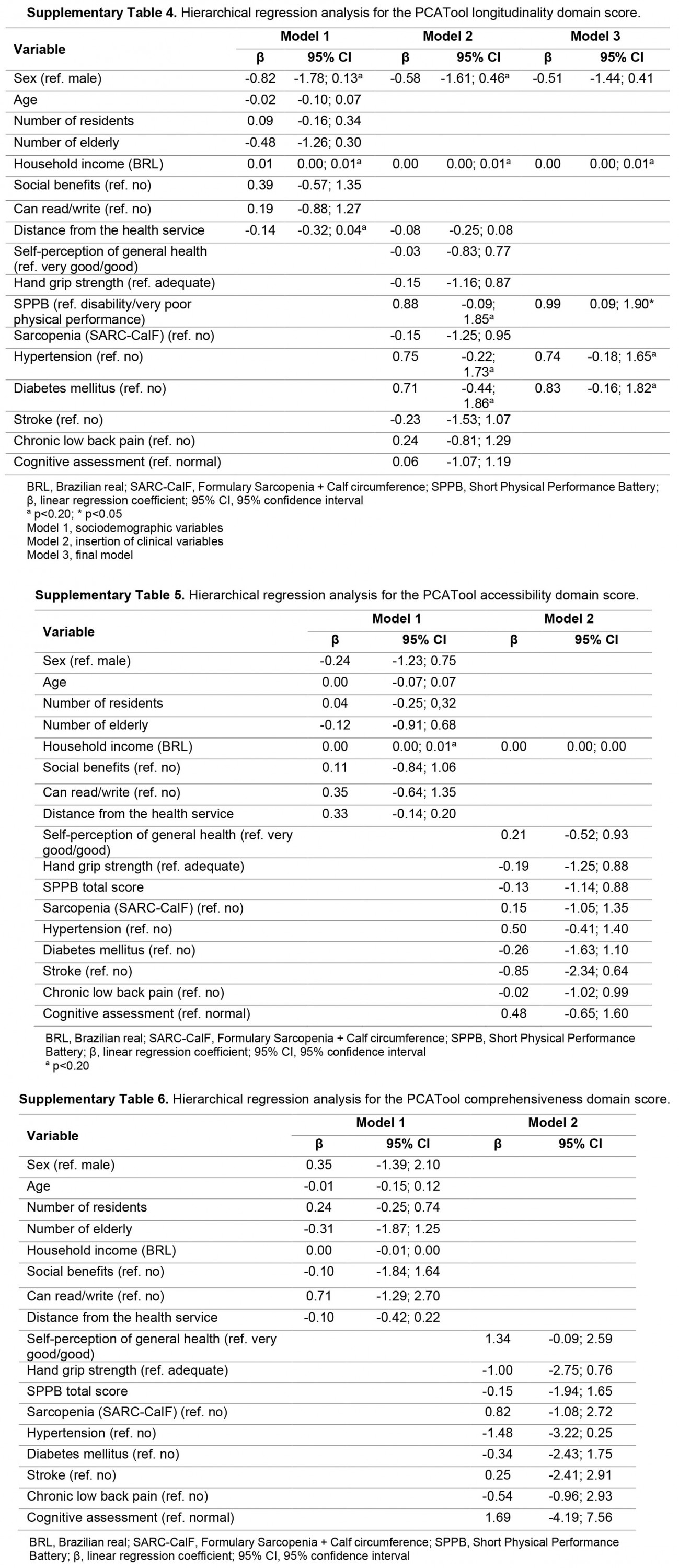
Despite the lack of association of independent variables with the total score of the PCATool–Brazil, the reproduction of multiple regression analyses for the scores of each of the five domains evaluated in the instrument showed that the variables of distance from the residence to the place of stop at the basic fluvial health unit (β=–0.21; 95%CI=–0.49–0.07; p=0.145), SPPB (β=1.67; 95%CI=0.37–2.98; p=0.013) and SAH (β=1.40; 95%CI=0.02–2.78; p=0.047) remained in the final model of the affiliation domain. In the final model of the utilization domain, the variables of distance to the stopping point of the basic fluvial health unit (β=–0.25; 95%CI=–0.48 to –0.02; p=0.033), handgrip strength (β=–0.90; 95%CI=–2.05–0.25; p=0.124) and SPPB (β=1.19; 95%CI=0.06–2.33; p=0.040) were maintained, showing that elderly people who lived further away from the team’s stopping place had a worse utilization score, and also that elderly people with better physical performance perceived better quality in this domain. For longitudinality, the final model was represented by the variables of sex (β=–0.51; 95%CI=–1.44–0.41; p=0.271), family income (β=0.00; 95%CI=0.00–0.00; p=0.068), SPPB (β=0.99; 95%CI=0.09–1.90; p=0.032), SAH (β=0.74; 95%CI=–0.18–1.65; p=0.112) and DM (β=0.83; 95%CI=–0.16–1.82; p=0.098), showing that the elderly participants with better physical performance also perceived higher scores in the domain. No association was identified in the analyses for the accessibility and comprehensiveness domains (Supplementary tables 1–6).
Table 1: Household, socioeconomic and demographic characteristics of the elderly, Rio Negro, Manaus, Brazil (n=98)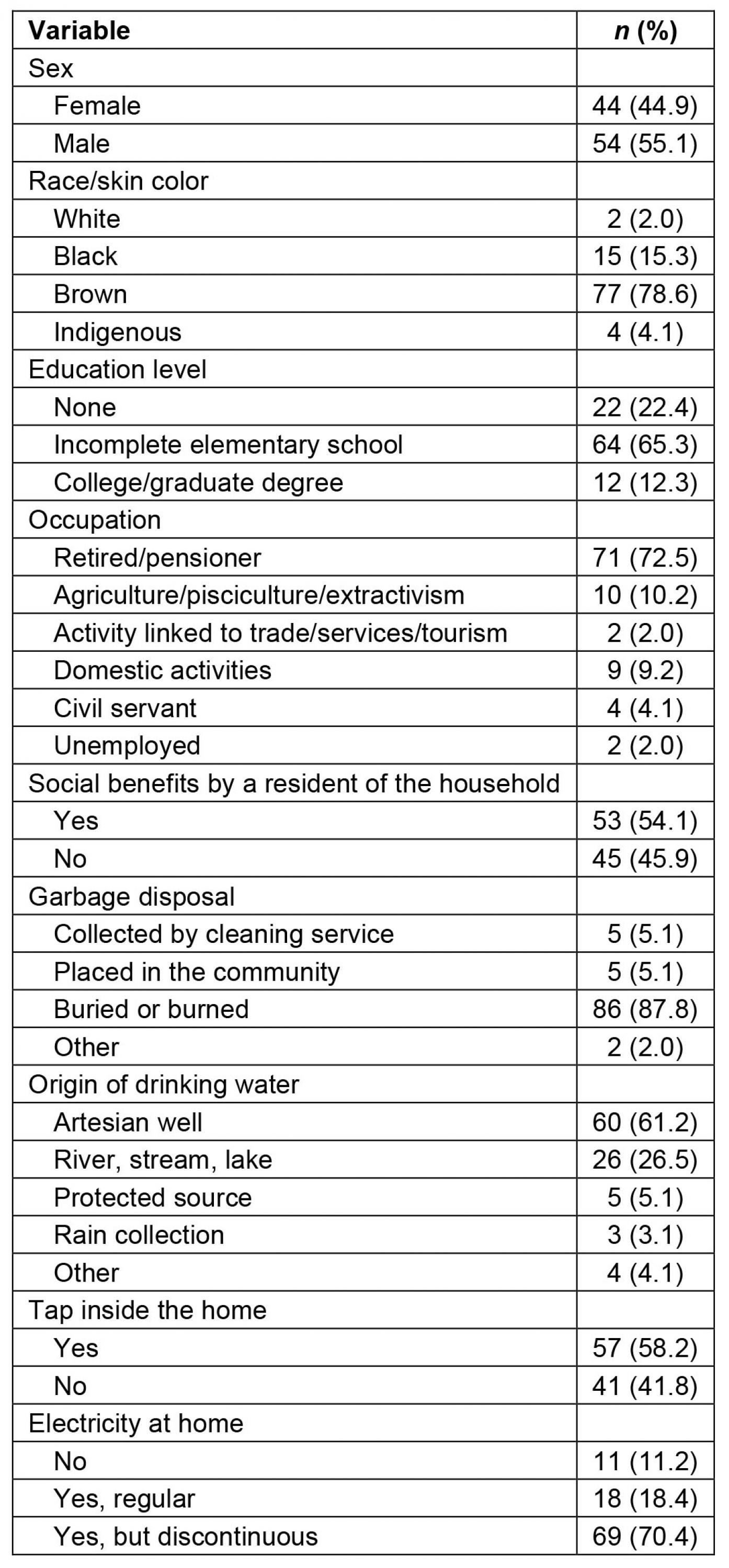
Table 2: Variables related to the health conditions of the elderly, Rio Negro, Manaus, Brazil (n=98) 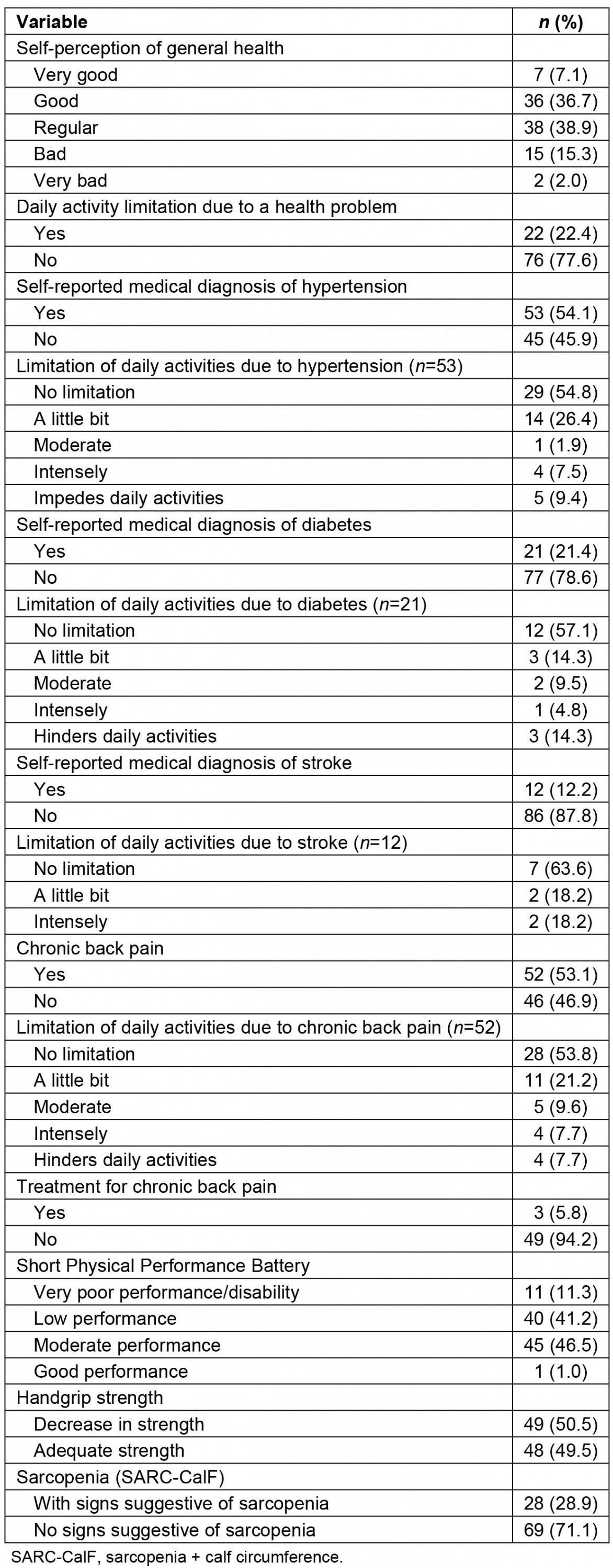
Table 3: Use of health services by the elderly, Rio Negro, Manaus, Brazil (n=98)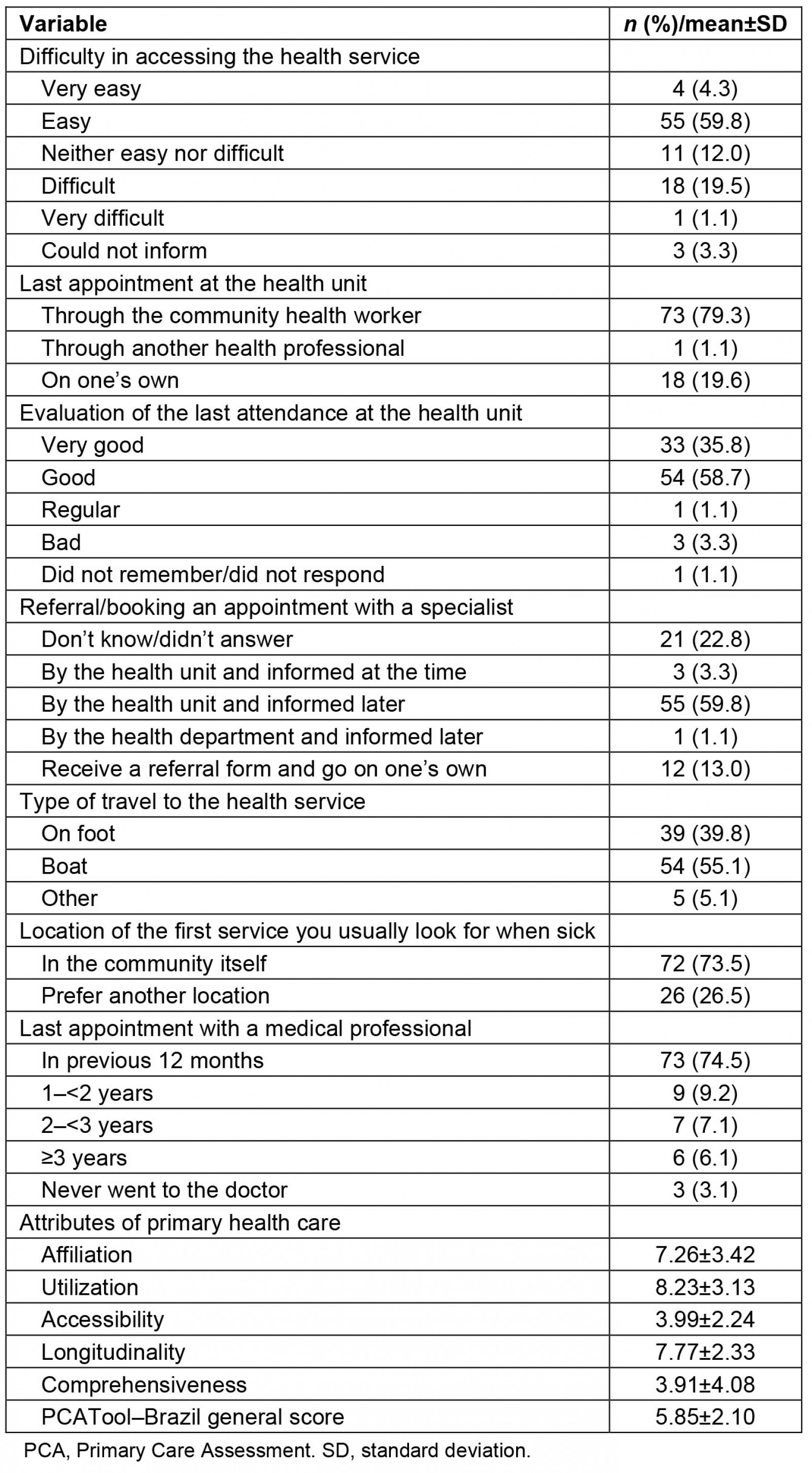
Table 4: Hierarchical regression analysis for the outcome of medical consultation in the previous 12 months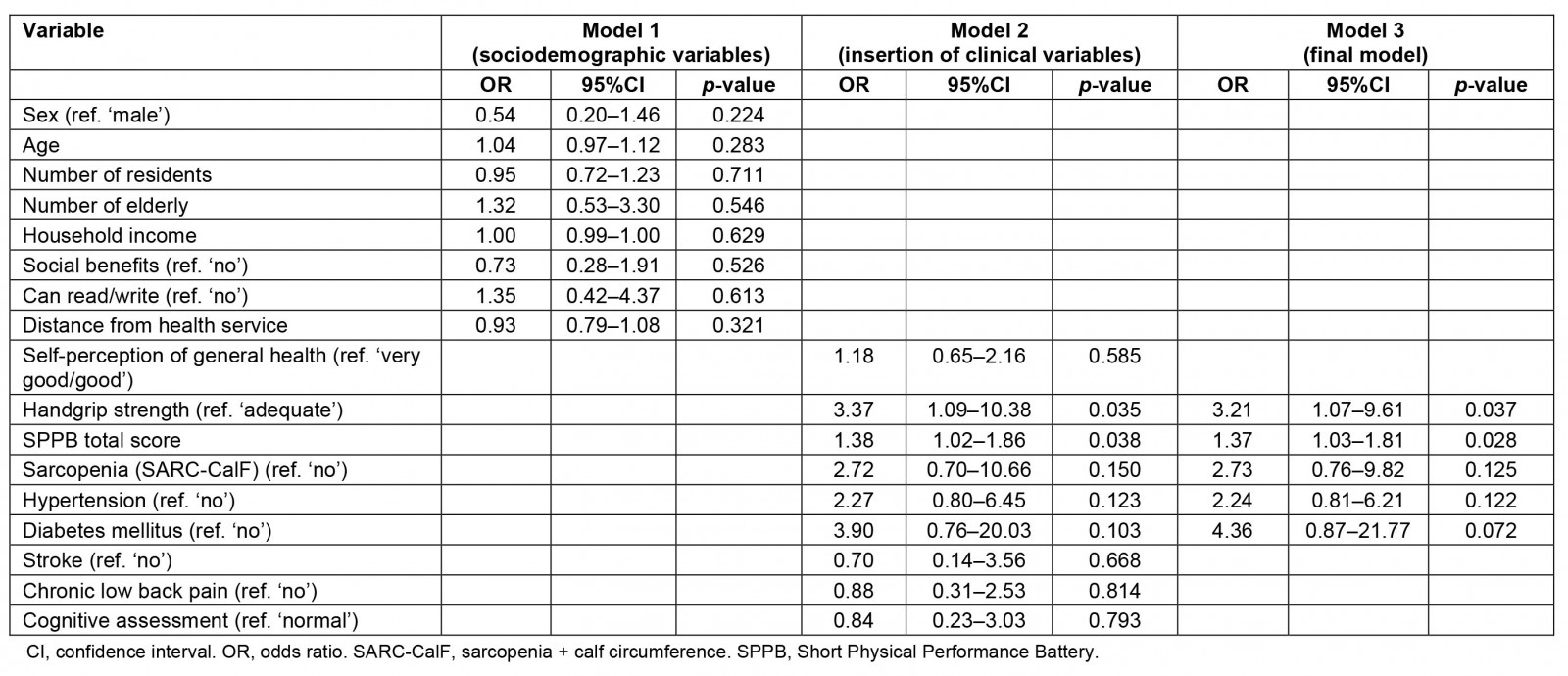
Discussion
The findings of the study show a low physical performance of the elderly participants evaluated, as well as signs suggestive of sarcopenia, according to the instruments used. Elderly people with better physical performance reported greater use of health services and higher scores in the affiliation, utilization and longitudinality domains of the PCATool–Brazil. SAH and the distance to the basic fluvial health stop location were also associated with the scores in the PCATool–Brazil domains affiliation and utilization, respectively.
The vast majority of the elderly participants lived in situations of socioeconomic and health vulnerability. Similar data were found in other studies involving rural riverside populations24-26. In public health, there is a consensus on the recognition that groups with worse socioeconomic conditions have a greater burden of disease, both chronic and acute, a greater burden of physical and mental disabilities at an older age, have a greater number of home or urban accidents, have less access to health care at all levels, and care, when provided, is of lower quality6. A study by Wu et al suggests that improving access to health care and services associated with the reduction of environmental health risks are fundamental to improving physical and psychological health by the elderly27.
SAH and self-reported CLBP were the most prevalent chronic conditions in the sample. Most respondents reported limitations in carrying out their basic activities of daily living due to one of these conditions. SAH, DM and the combination of both, as well as CLBP, are morbidities with a high prevalence in the elderly population living in riverside areas25,28,29. Corroborating our findings, several studies have already shown that functional incapacity to perform basic activities of daily living is associated with the presence of chronic diseases30,31.
Regarding self-reported low back pain, most of the sample did not undergo treatment for the condition, in addition to the intervention being usually restricted to drug interventions. The literature shows that the prevalence of CLBP in rural areas is associated with agricultural activity and worse self-perception of health, with the most frequent treatments involving self-medication and massage25,32,33. Chronic pain is a highly complex condition, related to multiple factors, especially as mediators of negative outcomes such as multimorbidity and functional disability34. A study carried out with a rural riverside population in the Amazon observed a high prevalence of elderly people diagnosed with chronic disease, low education and low income who reported low back pain and perceived their health as fair, poor or very poor33.
The present study identified a high prevalence of decreased handgrip strength, and a significant number of women showed signs suggestive of sarcopenia. Similar data were found in elderly people living in rural areas in Northeast Brazil35, as well as in a longitudinal study carried out in China27. However, in contrast to these findings, a study carried out in South Brazil showed that the prevalence of sarcopenia was significantly higher in women living in urban areas, and the place of residence remained independently associated with sarcopenia36. In the literature, studies have shown that women are more prone to the presence of sarcopenia than men, considering the hormonal implications, exposure factors associated with sex, the differences in the burden of disease between men and women with disabilities, and the greater susceptibility of women to these comorbidities37-39. However, the prevalence of sarcopenia may vary between different study populations and according to the adoption of different diagnostic criteria27,37,38. It is noteworthy that the difference in the outcome between men and women is a finding that emphasizes the importance of early tracking of muscle loss in those groups identified as more vulnerable.
There are several factors that interfere in or influence the physical performance of elderly people. Among them, chronic diseases, sarcopenia, chronic pain and housing and environmental conditions stand out. In a study carried out with elderly people living in rural areas of China who were stroke survivors, those who lived below the poverty line were more likely to have low physical performance and need assistance in their daily lives40. However, the high prevalence of elderly people with low physical performance identified in the present study contrasts with the results of a study carried out in the rural area of a municipality located in Northeast Brazil, in which were observed a high number of physically active individuals and a low prevalence of functional dependence41. In another investigation, which evaluated the functional capacity related to posture and balance of the elderly in riverside rural areas and in urban areas in the Amazon, a better level of performance was also observed in relation to the urban elderly, mainly in three of the six domains present in the Scale of Berg Equilibrium42. The differences in the findings can also be justified by the different realities and characteristics of the cities and population groups studied, in addition to the existence of variation in the concepts and instruments used in the studies to identify disabilities and functional limitations43. Given this scenario, the need to develop instruments that provide comparable results is unquestionable.
The study findings showed that elderly people living in rural riverside locations with better physical performance used health services more. It was also observed that the decrease in muscle strength itself was not capable of preventing access to services, which occurred when there was an impact on the physical performance of the elderly. Some of the key determinants of access include the personal skills of older people and characteristics of the health system, both in rural and urban areas. The lack of availability of services and distances are relevant aspects in rural areas, while the urban population maintains financial barriers as the main obstacle to accessing health services44.
To assess qualitative aspects of access and use of health services, this study additionally used the PCATool–Brazil scale, analyzing some PHC attributes. Sociodemographic factors associated with vulnerability (low income, living in rural areas and advanced age) have been associated with different attributes of PHC45, suggesting paths in the search for equity in the access and quality of the health services offered. The attributes evaluated in the study were considered satisfactory, especially when the area assigned to the basic fluvial health unit was evaluated or when the rural location had a basic health unit in a fixed location, making access easier. In this sense, a study carried out with a riverside population in the Northeast region of Brazil showed that the best evaluations of PHC attributes occur in places where there are fixed health units46, showing the impact of these forms of organization in such locations.
In the rural context, PHC is sometimes the only gateway to the unified health system, including for urgent and emergency situations. From this perspective, the availability of adequate means of transport must also be taken into account, as well as the qualification and appreciation of the CHW to act in the face of the specificities imposed in the rural environment, since he/she represents the main link between the community and the health service47,48. Considering the distance to access health services (on average more than 2 km from their homes to the basic fluvial health unit stop, traveled mainly by river), the duration of the trip (1 hour, on average) and the travel costs, it is important to emphasize the impact of any health problem and the financial burden on the individual and his/her family. These factors are relevant in view of the already limited resources of the riverside people, leading them to resort to the resources available in their own locality and performing self-medication and polypharmacy, which may aggravate their condition, in an attempt to solve the problem, or delay trying to reach the health service in the expectation of improvement25. Distance is one of the main critical factors that limit the access of these populations, both for the community health unit and for the urban area, in addition to hampering home visits by health team professionals49,50.
It is noteworthy that, despite the difficulties of access, the evaluated elderly reported a high frequency of use of services in the previous 12 months, which may be a result of the improvement in the availability of services by the basic fluvial health unit, as well as treating the elderly as a priority group in health actions. Care for people with SAH and DM is also a priority at this level of care51. However, despite the basic fluvial health unit operationalization strategy having provided great advances in access to services and offering programmatic care, it is still necessary to expand and qualify actions in rural areas for greater coverage of these populations52.
In this context, the findings of this study reinforce the concept that the presence of sarcopenia is related to physical performance, and this, in turn, influences the use of health services by the elderly population. An inversion of the logic explained by the present study is necessary, in which individuals with declining physical performance reported less contact with health services, despite their greater health needs. Thus, prevention and health promotion strategies should be planned in order to ensure, as much as possible, the independence and autonomy of the elderly. Priority strategies should guide managers, professionals and researchers to improve accessibility in order to reduce barriers to the availability of health services, to avoid low resolution of care and the unnecessary collapse of care levels with greater technological density. In addition, these strategies should increase the comprehensiveness of care, prioritizing actions that promote health, and specific care for the most prevalent diseases and conditions45. This need is demonstrated by the limited practice of prevention, self-care and social support actions for elderly people and their caregivers, showing the need for inexpensive health practices, but with a great impact on public health, as well as professional qualifications related to these practices53.
Among the limitations of the present study, the possibility of information bias for some variables self-reported by the elderly participants is included. Data on time and distance for access to health services may also vary in relation to the timing of the research; for example, this study was carried out during the flood season of rivers and lakes, which allowed navigation with less difficulty. This contrasts with periods of drought, when there is the possibility of isolation of some locations and a substantial increase in the time and effort to access health services. Another limitation is related to the study design, which, as it is cross-sectional, implies caution in interpreting the causality of the associations found, since it is not possible to determine whether better physical performance enabled greater access to services or whether individuals who sought health services more were those most concerned about their health and with better functional capacity. It is also important to highlight that only the most populated rural riverine localities were chosen to be part of the study. Therefore, the study findings may not be generalized to less populated or isolated riverine localities, which tend to have worse health conditions and even more limited access to health services, and may face greater barriers to the health services utilization in the presence of lower physical performance. On the other hand, this study was conducted with a population that has been little studied in Brazil, covering all the elderly in the selected locations, thus being able to add support to the elaboration of specific actions aimed at rural riverside populations.
Conclusion
The study findings showed high prevalence of impairment in physical performance and suggestive signs of sarcopenia in elderly people living in the studied rural riverside localities. Better physical performance was associated with use of health services in the last year and with better evaluation of some primary care attributes. Recognized barriers to access faced by this population group can be aggravated by the decrease in physical performance, reducing the use of health services, as well as the attributes of the care obtained. Thus, improving access for this population requires organizational measures of the local health system that enhance access to health services and the organization of care flows. Finally, the importance is recognized of carrying out other studies with elderly people living in riverside areas, involving larger populations and with longitudinal monitoring, in order to expand knowledge about the determinants and implications of physical performance in the health care of these patients.
Funding
The study was funded by the Foundation for Research Support of the State of Amazonas (FAPEAM) PPSUS-01/2017 - EFP_00014168, and PROEP-LABS/ILMD Fiocruz Amazônia, call for projects 001/2020. Aline M Queiroz and Jordana H Siqueira received scholarships (Master’s degree, and Scientific and Technological Development, respectively) from the FAPEAM. Fernando Herkrath is a FAPEAM research productivity fellow.
Conflicts of interest
The authors declare that they have no competing interests.
References
Supplementary material is available on the live site https://www.rrh.org.au/journal/article/7957/#supplementary
You might also be interested in:
2022 - Perceived risk and pandemic response awareness in low-capacity public primary health care in Greece