











Context
Introduction
Health equity is a crucial aspect of public health, ensuring that all members of society have equal opportunities to achieve their full health potential. While New Zealand has focused on health inequities, these have mainly been based on ethnicity or gender. In recent years, New Zealand has increased its focus on rural health equity, leading to the development of, for the first time, a specific Rural Health Strategy in 2023 underpinned by legislation1. The importance of a specific strategy for rural health, particularly in countries with large rural populations and regions, has been well established2. This article delves into the background and context of rural health in New Zealand and the specifics of the development and implementation of the first New Zealand Rural Health Strategy.
New Zealand began reform of its health system in 2018 with the commissioning of the Health and Disability System Review3. The emergence of a specific rural health strategy was contributed to significantly by the simultaneous presence of three important factors, which will be discussed below.
- The restructuring of the healthcare system with a focus on equity, including geographic equity in access and coverage, were government priorities that enabled rural access and health equities to be brought to the fore in this context.
- The increased awareness of geographic inequities for rural communities and the emergence of high-quality research data demonstrating clear rural/urban health disparities.
- The emergence of the Hauora Taiwhenua Rural Health Network as a single strong collective membership-led and driven advocacy voice for health care in rural communities.
The Health and Disability System Review3 was tasked with taking a system-wide approach to identify what needs to change to ensure the future health system achieved better and more equitable health and wellbeing outcomes for all New Zealanders. The Health and Disability System Review highlighted regional inequities in health services and outcomes, alongside other factors like ethnicity, but had little focus on rural/urban disparities3. This may be partially explained by the concept of geographical narcissism, the subtle, often unconscious, devaluation of rural knowledge, conventions and subjectivity4 seen with the increasing urbanisation of many countries. It did, however, raise concerns about the sustainability of rural health services and equity for rural communities. The Pae Ora (Healthy Futures) Bill, on which the Pae Ora (Healthy Futures) Act 20225, was based was introduced to Parliament for its first reading in October 2021. The Bill provided the direction for the reformed system and, in the legislation introduced to Parliament, there was a focus on equity and priority groups that included rural communities within the expectations for the Government Policy Statement on Health (GPS), but no mandated Rural Health Strategy. However, after much background advocacy work and representation from the Minister for Rural Communities, the final version of the Act mandated a specific Rural Health Strategy. This crucial rural health advocacy work was effectively led by, and continues to be led by, the Hauora Taiwhenua Rural Health Network6 in addition to a number of other rural advocacy groups such as ‘Federated Farmers of New Zealand’ and ‘Rural Women New Zealand’.
The Hauora Taiwhenua Rural Health Network was formed in 2022 but was preceded by the New Zealand Rural General Practice Network founded in 1991 by a group of rural general practitioners passionate about providing primary care to rural communities. In 2022, the New Zealand Rural General Practice Network made the transformation to unite with its partners Rural Health Alliance Aotearoa New Zealand, Rural Nurses New Zealand, New Zealand Rural Hospital Network, Students of Rural Health Aotearoa and the New Zealand Institute of Rural Health to form a new collective organisation representing the breadth of the rural health sector and thus the Hauora Taiwhenua Rural Health Network was born. The importance of having a strong collective advocacy voice with a bicultural focus for rural communities was seen most clearly when it resulted in the inclusion of rural communities as a priority population, thus mandating a Rural Health Strategy, in the Pae Ora (Healthy Futures) Act 20225.
This Rural Health Strategy was mandated alongside strategies for four other priority groups and an overall New Zealand Health Strategy. The New Zealand Health Strategy takes a whole-population focus, and considers systemic issues, opportunities and priorities1. These priorities are also relevant to improving health in rural communities, as well as nationally. In the period prior to rural communities being a priority group within the Pae Ora (Healthy Futures) Act 2022, there was not a specific focus from health agencies on outcomes in rural communities or the impact of health system settings on rural communities. While differing services and access issues were acknowledged for rural communities, there was no focus on inequitable outcomes, often due to a lack of specific rural outcome data or because it was assumed that inequitable outcomes between rural and urban did not exist. This changed with the emergence of high-quality data and key reports that clearly demonstrated the disparities in health outcomes for many rural communities in New Zealand7-9.
The recent New Zealand health reform, which consolidated 20 separate District Health Boards into a single entity of Health New Zealand, means that, for example, the rationale for new funding streams for rural health are still being developed. The health system in New Zealand consists of Manatū Hauora, the Ministry of Health, which is the chief steward of health and the health system, and the lead advisor to government on health. To give effect to this role, the Ministry sets the direction, policy, regulatory framework and investment for health, and monitors outcomes and system and organisational performance10. The Rural Health Strategy was developed by the Ministry and approved by government, with input from the Māori Health Authority (disestablished in 2024), Health New Zealand, other government agencies, and engagement with the health sector, stakeholders and general public. The main entity responsible for delivering or purchasing health services for New Zealanders, including for rural communities, is Health New Zealand. Health New Zealand is responsible for commissioning, planning, funding and providing all health services, both primary and secondary.
Rural definitions and classification
The New Zealand Rural Health Strategy focuses on people who live in rural communities where rural areas are not just categorised by the lower population density but also by the degree of isolation in terms of distance from main urban centres and services1. For the purpose of measuring outcomes within the strategy, rural communities or populations are defined using the Geographic Classification for Health (GCH), which has been developed for categorising New Zealand’s rural and urban areas to monitor health outcomes11. This was part of the new research emerging at the time the Rural Health Strategy was mandated. Generic rural classifications have previously underestimated rural health needs, perpetuating health inequities in rural communities. The purposively designed GCH provides a more accurate representation of rural health in New Zealand and has spelled a significant change for rural health, for the first time producing an evidence base for both advocacy and monitoring purposes. The GCH has five categories. It has three rural categories (R1, R2 and R3) based on distance to urban centres and services, and relative sizes of populations in the area. The most remote and isolated rural communities are classified as R31. There are two urban classifications, one for the six main urban centres (U1) and one for provincial centres (U2).
Around one in five (19%) people in the New Zealand population live in rural areas12. Most of the people in rural communities are in areas that border urban areas, or relatively large rural centres (R1)1. The R1 category comprised 12% of the New Zealand population; the R2 category, 6% (this group are either further away than R1 or have smaller populations than R1); and the R3 group, the most remote rural areas including offshore islands, such as Rēkohu | Chatham Islands and Rakiura | Stewart Island, have around 1% of total New Zealand population1. In countries with a similar total population to New Zealand, Finland (30%) and Sweden (25%) have higher rural populations, while Norway (18%), Denmark (18%) and Scotland (17%) have similar rates to New Zealand, and Ireland a bit less (14%). Rural communities in New Zealand have a higher proportion of Māori than urban populations, with around 22% identifying as Māori, compared with 15% in urban areas.
Issues
Rural–urban and within-rural differences in health service coverage and outcomes
In the exploration of rural–urban health inequities, the definition of rurality is a key factor that has been clearly described in countries such as Canada, the US and Australia12-15. This issue of a clear definition of ‘rurality’ for health has now been resolved with the creation of the GCH as described earlier. Historically, rural areas in New Zealand have faced challenges in health service coverage compared with urban areas. The Rural Health Strategy1 has outlined factors, such as limited healthcare infrastructure, workforce shortages, distance from specialised services and socioeconomic disparities, which contribute to these differences:
- Rural people experience worse overall health outcomes compared with urban populations7.
- Mortality rates for rural communities are generally higher than they are for their counterparts living in urban centres16. These differences are heightened for rural Māori communities17.
- Suicides for males are considerably higher in rural areas and, for 15–44 year olds, the rural suicide rate is 64% higher than the urban rates12.
- Rural communities have a larger share of populations with high health needs, including Māori and older people7.
- Rural Māori face significant unmet health needs and face inequities in access to, and quality of, care1. Māori health in rural communities is poor for a range of complex reasons, including histories of structural and interpersonal discrimination and racism based on ethnicity and the impact of wider socio-economic factors including poverty and poor housing.
- Barriers to access services means that rural people do not have the same uptake of prevention or public health initiatives, or options that mitigate health conditions, including early diagnosis, immunisation and screening. Rural Māori (56%) and rural non-Indigenous (75%) children have lower rates of being fully immunised at the 2-year-old milestone than their urban counterparts1.
- People living in rural areas are more likely to be daily smokers than those living in urban areas. Rates of hazardous drinking are higher in rural areas.
- Rural communities persistently experience poorer mental health outcomes than the general population. This is likely to be due to both challenges in accessing specialist mental health support in rural communities, as well as the social, economic, environmental and cultural factors affecting rural communities.
- Higher levels of socioeconomic deprivation are associated with poorer health. Deprivation, as measured through the New Zealand Deprivation Index18, is a combination of communication, income, employment, qualifications, home ownership, support, living space and transport. Rural communities have a higher share of their population living within areas considered to have the highest deprivation (top quintile), than the main urban areas. Deprivation is felt hardest in remote rural areas, R3, with around 40% of the people living in these areas categorised as being in the group with highest deprivation.
- The Ministry of Education’s Equity Index19, which is also used to determine the schools that will receive the Ka Ora, Ka Ako Healthy School Lunches programme, suggests that families with children in rural areas are more likely to have more socio-economic challenges. Of rural-based students, 41% were in schools that received the Ka Ora, Ka Ako programme at the start of 2023 (versus 24% in urban-based schools) while for Māori rural-based students, this figure is around 66% (versus 48% in urban-based schools), and for Māori students in the most remote rural schools, it is over 70%19.
- The poorer levels of educational achievement of students in rural-based schools can also have health workforce implications, with the enrolment rate of rural-background students (enrolments per 100,000 rural population) in medical school being less than half that of the enrolment rate of students from urban areas20.
In addition, the Rural Health Strategy highlights a number of specific rural health system challenges. Rural health workforce shortages in New Zealand are a challenge to achieving equitable access to health services for rural communities. The workforce gaps within healthcare professional groups, including doctors, nurses and allied health workers, are a significant issue internationally, limiting the availability and timeliness of care. The Rural Health Strategy recognises these challenges and emphasises the need to improve rural health training pathways to attract and retain health professionals in rural areas, as well as more flexible workforce arrangements to support broader care in rural communities.
There are service gaps in rural communities, sometimes due to workforce shortages, or the services are not available in their community, such as acute mental health or aged residential care. There is also the uneven distribution of pharmacy and laboratory services or diagnostic testing, making diagnostics and, at times, essential medications difficult to access. Consequently, rural communities can face delays in diagnoses and treatments, or travel to main centres to access diagnostic testing. Limited access to specialist care further amplifies health inequities in rural communities. Rural residents often need to travel long distances to urban centres for specialist consultations and treatments, incurring substantial indirect costs related to travel, accommodation, and time away from work and caring responsibilities. These financial and logistical barriers deter many from seeking necessary care, leading to poorer health outcomes. Additionally, while digital health and telemedicine solutions have the potential to improve access to care, their effectiveness is hindered by inadequate internet access in some rural regions.
Primary care, rural hospitals and urgent after-hours unplanned care are areas of essential services for rural communities that have sustainability issues. The current settings and models are not sustainably supporting these services in rural communities. Primary care services, while having some rural ‘add-ons’ are mainly urban-based models. Integrated, broader and different workforce models are needed to support primary and community services in rural communities.
Barriers to health promotion and prevention activities for non-communicable diseases, alongside challenges in integrating social and health services for ageing populations, are also noticeable issues in rural New Zealand. Limited resources, workforce shortages and geographic isolation impede health promotion initiatives. The fragmented nature of social and health services complicates the provision of comprehensive care for older adults, who often require coordinated support across multiple sectors. The Rural Health Strategy highlights the need for innovative, integrated approaches to overcome these barriers and ensure that rural communities have equitable access to preventive care and wraparound services that support ageing in place. Technology is a key enabler of such innovative approaches and has been shown to improve continuity of care for rural communities by increasing access to care and reducing the need for travel and associated costs21. However, technological solutions will not work in isolation but must be culturally appropriate and co-created with rural communities and must involve ‘relational work’, building connections and relationships to prioritise cultivating trust in partnerships over specific outputs22.
Role of the Rural Health Strategy
The Pae Ora (Healthy Futures) Act 2022 required the New Zealand Government to produce a Rural Health Strategy, including, for the rural context: an assessment of the current state of health outcomes and health sector performance; an assessment of the medium and long-term trends that will affect health outcomes and health sector performance; and an identification of priorities for improving the health sector, including for the rural health workforce1. The role of this strategy is to set the long-term direction for improving rural health. The strategy does not commit to precise actions for health entities. More specific decisions and actions are made in the GPS and the New Zealand Health Plan, which set out specific actions and priorities for 3-year periods, the current period being 2024 to 202723.
The development of the Rural Health Strategy has been informed by engagement with the public, stakeholders and those within the health sector. Rural Health Strategy engagement was also undertaken alongside the other five mandated Pae Ora Strategies. Between November 2022 and May 2023, Manatū Hauora received feedback and submissions across multiple different channels, including through in-person and online engagements, regional wānanga and social media1. The engagement for Pae Tū, Hauora Māori Strategy, had particular insights for rural Māori. An overall summary of feedback across the strategies was published24 as was specific engagement from Māori communities25.
Specific engagement on the Rural Health Strategy was carried out through public consultations, workshops and interviews held in rural communities across the country, ensuring diverse perspectives were included in the Strategy. The process was sense-checked by sharing initial drafts of the strategy with stakeholders for review and comment. This approach allowed for refinement of the strategy and ensured that the strategy accurately reflected the needs and priorities of rural communities.
New Zealand Rural Health Strategy aims and objectives
The Rural Health Strategy 2023 sets the direction for improving the health and wellbeing, both physical and mental, of New Zealanders living in rural communities over the next 10 years1.
This strategy identifies five priorities over the next 10 years1:
- Considering rural communities as a priority group. Health policies and planning are designed to meet the specific needs of rural communities – rather than expecting rural communities to fit into funding approaches and ways of offering care in urban settings.
- Prevention: paving the path to a healthier future. Rural communities have building blocks in place to support healthier futures – stable jobs, good pay, quality housing, digital connectivity and resilience to climate change. Preventive health interventions (such as screening) and promoting and protecting people’s health and wellbeing are key areas of focus.
- Services are available closer to home for rural communities. A wider range of service options are available in the home or in the community, including from outreach options (such as mobile outpatients’ clinics and digital solutions).
- Rural communities are supported to access services at a distance. Where it is not possible to access health services locally, coordinated support is available to help rural people travel or use digital technology to receive care.
- A valued and flexible workforce. The rural health workforce is developed and supported to deliver the care that rural communities need – including through kaupapa Māori approaches and extended healthcare roles and rural specialisations.
Activities
One of the objectives of the Rural Health Strategy, which is part of a wider health system reform, is to better align and integrate the accountability arrangements that set direction and priorities for health agencies. The reforms put in place a new approach that aims to ensure clarity and coherence, from long-term strategic objectives to shorter-term priorities and expectations (Fig1).
This new approach provides a clear pathway for translating strategies into action, and monitoring and evaluating the impact of strategies and the performance of agencies. The role of health strategies is critical to providing the long-term vision and priority areas that inform decisions on the other documents. The Government Policy Statement on Health 2024–2027 (GPS)23 sets five priority areas for improving health for New Zealanders: access; timeliness; quality; workforce; and infrastructure. These priorities are key to improving health system performance. There are several GPS expectations outlined below that can improve rural health outcomes23:
- Work in partnership with local communities to ensure primary and community care services are increasingly tailored to better respond to people’s needs, including family and community-based services.
- Implement initiatives that support an increased understanding and uptake of online care and telehealth, particularly in primary and community health care settings, and equip people, families and whānau to better meet their own mental wellbeing needs.
- Improve the transport and accommodation assistance support, particularly for disabled people and people living in rural communities.
- Improve access to domestic training pathways to deliver a culturally competent and home-grown workforce that better reflects the population of New Zealand as a whole.
Health New Zealand is currently developing the New Zealand Health Plan, which will have actions that give effect to the expectations of the GPS. Three areas of work already underway of key importance for rural health include the Rural Unplanned and Urgent Care review, the Rural hospital sustainability project and the Primary and community care design work.
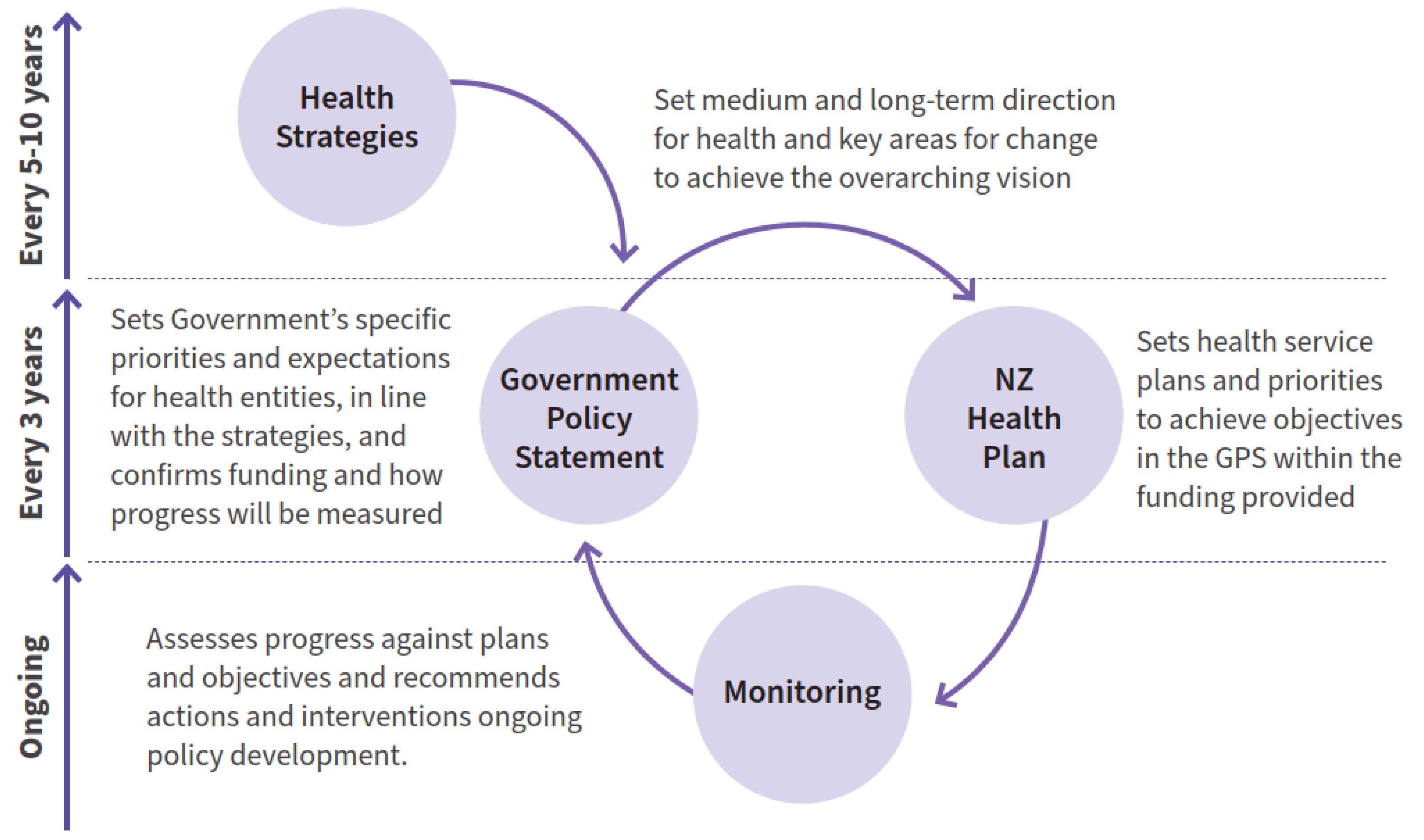 Figure 1: System architecture of the health system post-reforms. Source: Minister of Health, 20231; reproduced with permission.
Figure 1: System architecture of the health system post-reforms. Source: Minister of Health, 20231; reproduced with permission.
Monitoring approaches
The health strategies set a direction towards achieving pae ora | healthy futures for all New Zealanders and include goals to eliminate health inequities and improve health outcomes. Monitoring progress towards this vision requires a long-term approach to measuring key health outcomes and policy changes. A monitoring approach is being developed by the Ministry of Health for the Rural Health Strategy.
The GPS for 2024–2027 sets out several measures for monitoring the priorities and overall health trends. The expectation is that these will be reported by key breakdowns, including rurality, where appropriate and feasible. The monitoring approach for the Rural Health Strategy will look to align with some of the GPS monitoring measures, where appropriate, but also draw on rural-specific areas that support direction set by the priorities in the strategy.
Lessons learned
The New Zealand Rural Health Strategy envisions a future in which the health system considers the different needs of rural communities, and the insights and strengths of rural communities are used to improve wellbeing, address equity and achieve pae ora – healthy futures1. In this vision, rural communities are valued, and the needs of people in rural areas are considered across the health system, which is an excellent foundation for achieving rural health equity in any healthcare system and society. The health sector is committed to fulfilling the special relationship between Māori and the Crown under Te Tiriti o Waitangi | The Treaty of Waitangi23. Regarding the text of Te Tiriti and declarations made during its signing, the Crown, as the kaitiaki and steward of the health system (under article 1 of Te Tiriti), has the responsibility to enable Māori to exercise authority over their health and wellbeing (under article 2) and achieve equitable health outcomes for Māori (under article 3) in ways that enable Māori to live, thrive and flourish as Māori. These requirements were highlighted in the findings and recommendations from Stage One of the Waitangi Tribunal’s Health Services and Outcomes for Māori Inquiry26.
The New Zealand Rural Health Strategy takes a rights-based approach to rural health equity by recognising and prioritising the hauora – health and wellbeing – of Māori as supported under Te Tiriti o Waitangi. This approach acknowledges the Treaty’s principles of partnership, protection and participation, ensuring that Māori have a voice in health decision-making processes and that their cultural needs are respected and integrated into health services. The strategy emphasises the importance of reducing the significant health inequities experienced by rural Māori. Key tenets of this approach include the commitment to Te Tiriti o Waitangi, the integration of Māori health perspectives into policy and service delivery, and the focus on partnership in health solutions with Māori communities. The strategy also underscores the need for culturally appropriate health services that respect Māori values and practices, and it calls for changes to address the underlying social determinants of health that disproportionately affect Māori in rural areas. This inbuilt recognition of the needs of Indigenous peoples, in this case Māori, across the healthcare system is another real strength of the rural health strategy.
The Rural Health Strategy also aligns with the broader government effort to rural-proof policies, with significant contributions from other government departments, such as the Ministry for Primary Industries. This cross-sectoral rural proofing approach helps deliver more effective services by aligning them with the community’s needs. This represents a significant shift for the New Zealand health sector, with lots of existing settings not considered in this way. It may take some time to look at existing settings and fully realise the benefits for rural communities. The primary care programme of work – looking at national policy and funding settings – provides an initial test of how the process and final decisions support the different needs of rural communities.
New Zealand’s government arrangements are mainly at a central government level for health, with local or regional government involved more in social determinants of health, such as transport and environment. Health New Zealand (central government entity) has regional-level decision making around service delivery and approaches within their area but aligns with national policy and funding settings. There are also Iwi–Māori Partnership Boards at a local level. Their role in the health system is still being developed but this decentralisation of decision making is likely to benefit rural communities more and is always worth considering in the development of such strategies.
In regard to the development of a Rural Health Strategy, there is always potential for more collaboration across different levels of government, such as national and local. However, current collaboration around health in New Zealand is limited to quite specific areas, such as drinking water and the regulation of alcohol consumption. The Local Government (Community Well-being) Amendment Act 201927 sets out an expectation that local authorities can play a key role in promoting the social, economic, environmental and cultural wellbeing of their communities using a sustainable development approach. This acknowledges the importance of local leadership in enhancing community wellbeing, but the extent of this involvement varies widely due to the differing sizes and financial positions of 73 local authorities and 11 regional authorities across New Zealand28. There are opportunities to strengthen this coordination to better achieve the ambitions of the Rural Health Strategy during the development and implementation phases.
The development and implementation of any rural health strategy is a key first step towards rural health equity. This must continue to be underpinned by high-quality research evidence. For example, New Zealand’s most remote communities have the lowest rates of health service utilisation, despite high amenable mortality rates, which raises questions about geographic equity in health service design and delivery and warrants further in-depth research29. As we examined the experience of New Zealand, it is apparent that a number of other key levers are crucial to enhancing progress towards rural health equity globally. Strong advocacy and collaboration among rural health stakeholders is a vital foundation for success. In New Zealand, the continuing development and operation of the umbrella rural membership/advocacy group Hauora Taiwhenua Rural Health Network is a really good example of this30. Government and health system infrastructure that specifically focus on ‘Rural’ is also a vital building block. Examples of this in New Zealand are the role of the Office for Rural Communities in assessing rural community impacts and rural proofing policy changes across government, as well as health organisational structures including a dedicated rural health commissioning team and a national rural clinical network within Health New Zealand. There is a clear need for evidence-based policies and interventions tailored to rural contexts and often these solutions will emerge from the ground up and will be context specific, which is why effective community engagement and empowerment in health decision making is vital. Areas that have developed solutions that work for their community and that show models and approaches that could work for other rural communities need to be championed and shared nationally and internationally.
Conclusion
The New Zealand Government set the direction for a reform of the health system in 2018. This focused on improving overall health outcomes and health equity, including for geographic areas of New Zealand with a specific focus on Māori health. The emergence of better information on rural health outcomes, together with effective advocacy for rural health, contributed to rural communities becoming a priority group for the government, thus mandating the development of a Rural Health Strategy. The resulting Rural Health Strategy is a key first step towards rural health equity and improving rural health outcomes in New Zealand. Over time, monitoring of the implementation of the priorities of the strategy, and monitoring of overall health outcomes for rural communities, will assess the progress made towards the vision set out in the New Zealand Rural Health Strategy.
|
Māori terms |
Literal translation/significance |
|---|---|
|
Hauora |
Health/Health and wellbeing |
|
Hauora Taiwhenua |
Rural health/Umbrella Rural Membership and Advocacy Organisation |
|
Hapū |
Subtribe/Primary political unit in Māori society |
|
Iwi |
Tribe/Tribe |
|
Kaiāwhina |
Assistant/Term to describe non-regulated roles in the health and disability sector. |
|
Kaitiaki |
Guardian/Caregiver |
|
Ka Ora, Ka Ako |
To be satisfied with food, to learn/ Healthy School Lunches Programme that provides nutritious lunches, every school day, to primary and secondary students. |
|
Kaupapa |
Principle/An approach that incorporates the knowledge, skills, attitudes and values of Māori society. |
|
Manatū Hauora |
Ministry of Health/Ministry of Health |
|
Pae Ora |
Healthy Futures/Pae ora is a holistic concept that includes three interconnected elements: whānau ora, mauri ora and wai ora31 / The Pae Ora (Healthy Futures) Act 2022 is the foundation for the transformation of New Zealand’s health system |
|
Pae Tū, Hauora Māori |
Māori Health Strategy/Māori Health Strategy |
|
Te Tiriti o Waitangi |
The Treaty of Waitangi/The Treaty of Waitangi |
|
Te Whatu Ora |
The weaving of wellness/Health New Zealand |
|
Wānanga |
Meeting/Conference |
|
Whānau |
Family/Extended family |
Acknowledgments
This article is part of the WHO-sponsored Special Edition on Rural Proofing for Health of the journal Rural and Remote Health (RRH).
Ethics approval
Ethical approval was not required as this report did not involve human participants, personal data, or experimental procedures.
Disclaimer
This article represents solely the views of the authors and in no way should be interpreted to represent the views of, or endorsement by, the World Health Organization, or the authors respective employers. The World Health Organization shall in no way be responsible for the accuracy, veracity and completeness of the information provided through this article.
Funding
Funding for this work came from a grant to WHO from the Government of Canada entitled ‘Strengthening local and national Primary Health Care and Health Systems for the recovery and resilience of countries in the context of COVID-19’. The funder had no role in the design of the study, data collection and analysis, decision to publish, or preparation of the manuscript. The work was commissioned to the University of Limerick by WHO (as part of preparations for a ‘WHO Consultation on Rural Proofing for Health Equity’) through Agreement for Performance of Work 203424943 in 2024. The content used in this article was finalised, and reflects the context as of 13 February 2025.
Conflicts of interest
The authors declare no conflicts of interest.