


Introduction
South Africa has an inequitable distribution of doctors between the public and private sector1,2, with the national public health sector, staffed by approximately 30% of the doctors in the country, being the sole provider of health care for more than 40 million people who are uninsured and constitute approximately 84% of the population1. In contrast, approximately 16% of South Africans (8 million people) have private health insurance that provides access to health care from the remaining 70% of doctors who work in the private sector1. These ratios are similar for other cadres of health workers3,4. The rural areas in South Africa are historically underserved3-5, with a lack of access to healthcare providers being one of the primary root causes of health inequity, which is disproportionately experienced by people living in remote and rural communities6. There is some evidence that the health needs of rural populations are greater than those in urban areas, indicating the need for a proportionately higher number of health workers7.
The 2009 report on the KwaZulu-Natal (KZN) Department of Health, compiled by the Integrated Support Team8, acknowledged the problems leading to the lack of employment of healthcare professionals in areas of greatest need, as well as the absence of retention policies. An extract of the report notes:
Staff recruitment seems to be one of the biggest challenges facing the Department. For example, there is currently a shortage of about 78% of Pharmacists in the whole KZN province and this shortage is acutely felt in rural areas. Despite staff losses, no evidence was found of the existence of a clearly defined retention strategy in KZN Department of Health. The proposed Human Resource Management Structure developed by Human Resources also does not touch on the issue of retention. Despite the fact that the province has a large rural population, there is an over-concentration of health personnel in urban areas and an under provision of health personnel in rural areas.
The World Health Organization (WHO)6, in its global recommendations for increasing access to health workers in remote and rural areas, highlights education, regulatory frameworks and financial incentives, as well as professional and personal support, as significant aspects to be considered in the training, recruitment and retention of health workers for rural practice. In a tracking study of University of Witwatersrand medical graduates over the period 2007–2011, George et al9 reported that a rural background was the strongest predictor of working in a rural area, with respondents being nearly five times more likely to return to their home areas, as confirmed by other studies3,6,10.
In a review article11 that included 20 studies of health professionals in developing countries, the main factors affecting recruitment and retention highlighted opportunities for professional advancement, support networks and autonomy; managerial support; as well as maintenance of clinical skills and peer recognition as the major factors influencing retention in rural and remote areas. Other professional factors were identified, such as resource availability, hospital management and infrastructure11,12. Social or environmental factors listed in these reviews include feeling a sense of belonging in the community, working in a family-friendly environment, and having access to social networks11,12. The importance of general living conditions, better quality children’s schools, social/recreational opportunities, as well as safety and access to rapid transport to other cities was also highlighted as having an influence on retention2,11,12. Financial incentives related to health worker motivation were only mentioned in two reviews11.. Social and personal factors included employment opportunities and activities for spouses, as well as educational opportunities for children2,11,12, with the proximity of family and friends, and conditions facilitating conciliation between work and family, also being important2,11.
To address health worker staff shortages at rural district hospitals in KwaZulu-Natal (KZN) Province, the Umthombo Youth Development Foundation (UYDF), established in 1999, has been recruiting and supporting rural-origin health science students, with the intention that graduates would work in rural areas on completion of their studies13. Students are recruited from three districts (uMkhanyakude, Zululand, and King Cetshwayo) in KZN, study a health science degree at any public university in South Africa, and are provided with academic and social mentoring support to assist them to overcome the challenges they face, including 4 weeks per annum work exposure at one of the 15 participating rural hospitals in the above districts. From 1999 to 2018, students had a contractual work-back obligation that amounted to 1 year of financial support equalling 1 year work-back at a rural hospital. Through a memorandum of understanding with KZN Department of Health, graduates of the program were employed at rural hospitals.
Ross et al14 reported that 71% (52/73) of the 1999–2013 graduates with no further work-back obligations continued to work at a rural PHCF, as did 63% (91/145)13 in 2017. More recently, due to changes in the student funding mechanism, and shortages of funded posts at rural hospitals in KZN, where graduates would normally be employed, they are no longer contractually bound but are morally obliged to take up employment at a rural hospital if they are able to secure a post.
The 2018 Academy of Science of South Africa Consensus Report15, on reconceptualising South African health professions education, recommended the tracking of graduates in order to influence both the selection and education of medical students, and to provide evidence that they are impacting on service delivery in rural and underserved areas. In keeping with the Academy of Science of South Africa recommendations, this study aimed to determine the effects of various retention factors described in the literature on the choice of where rural-origin UYDF graduates worked, namely in a rural or urban, public, or private setting.
Methods
An online survey was conducted, with questions being compiled using factors reported in the literature11,12,16,17 that affect health worker retention in rural areas, and consisted of demographic details, personal satisfaction, hospital resources and employment factors; professional development and support; and community integration. The demographic data questions included (no names were collected) place of birth, marital status, number of children, primary and secondary school information, higher education details (degree, university, years to completion, rural exposure), work history and current place of work. Personal satisfaction questions included current job satisfaction, support of colleagues and supervisor appreciation/support, and safety. For hospital resources and employment factors, questions included sufficiency of physical equipment and medication, staffing sufficiency, renumeration and overtime. Personal and professional development questions were about practising their skills, continual learning, access to peers and senior staff or specialists, further study, and intention to leave, while community integration asked whether they felt part of the local community and belonged to any community group. Finally, they were also asked two questions: if they were not working at a rural hospital, what the reasons were; and the reasons why they work where they currently do, with a list of options provided. Where applicable, participants were required to choose a response from a 5-point rating scale (all the time, most the time, sometimes, not very often, not at all). The survey was compiled in Google Forms and the link emailed to all eligible graduates on 14 September 2021 with an invitation to participate. It was highlighted that the survey was anonymous, and choosing to proceed would be accepted as providing consent. Follow-up emails were sent encouraging eligible graduates to participate, with the survey closing on 23 November 2021.
The inclusion criteria were all UYDF graduates who had completed community service and at least one additional year of work by January 2021. The total number of eligible graduates was 317, of whom 139 responded, a 44% response rate. Of the 139 responses, four were excluded as two graduates had returned to full-time study, and two provided incomplete responses, giving a total of 135 viable responses that were used. Graduates had studied at 16 different universities across South Africa, with the majority (55%) graduating at the University of KwaZulu-Natal. Descriptive statistics were compiled using the statistical program jamovi v2.2 (The jamovi project; https://www.jamovi.org).
Ethics approval
Ethics approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (Approval No: BREC/00002918/2021).
Results
The demographic data are followed by the responses related to personal satisfaction, hospital resources and employment factors, professional development and support, and finally community integration. The demographic data on the 135 graduates (Table 1) indicate that 95% are from KZN and 98% are of rural origin, with 70% completing their secondary schooling in the rural district where they grew up. In addition, 63% are female and slightly more than 51% are single, and all were Black African.
Most of the graduates who participated were doctors (29%), followed by pharmacists (13%), and then radiographers (10%) (Table 2). At the time of the study, the majority (49%) of graduates were working at a rural PHCF, followed by 34% at an urban PHCF, and 11% in the urban private sector (Table 2).
The majority of graduates in the disciplines of audiology (56%), biomedical technology (50%), dental therapy (75%), dietetics (88%), nursing (75%), optometry (67%), pharmacy (50%) and social work (100%) were working at a rural PHCF. Regarding doctors, 28% (11/39) were working at a rural PHCF, 59% (23/39) in an urban PHCF and 10% (4/39) in the urban private sector. In total, 87% of doctors and 83% (112/135) of all graduates were working in the public sector (Table 2).
Regarding personal satisfaction, the majority, whether working in a rural PHCF, in an urban PHCF or in the urban private sector reported positively (all the time, most of the time) regarding enjoying their work (77% for rural PHCFs, 91% for urban PHCFs, 93% for urban private), enjoying their colleagues (77% for rural PHCFs, 78% for urban PHCFs, 100% for urban private), being part of a good team (77% for rural PHCFs, 84% for urban PHCFs, 88% for urban private), enjoying their colleagues’ support (68% for rural PHCFs, 80% for urban PHCFs, 69% for private urban), feeling safe in the workplace (78% for rural PHCFs, 84% for urban PHCFs, 69% for private urban), and feeling supported by their manager/supervisor (60% for rural PHCFs, 70% for urban PHCFs, 69% for private urban) (Table 3). The total responses for the last four questions were less than the total number of participants (127).
Regarding hospital resources (beds, equipment, medicines), the majority of graduates working at urban PHCFs (73%) and in the urban private sector (80%) responded that they were available ‘all the time’ or ‘most of the time’, while 40% of those working at rural PHCFs reported ‘all the time’ or ‘most of the time’, 28% said ‘sometimes’, and 21% said ‘not very often’ (Table 4). Regarding the question ‘Have you ever not been able to do something for a patient due to lack of equipment, medicine etc?’, for rural PHCFs, 21% of graduates reported ‘most of the time’ and 60% reported ‘sometimes’, while 52% of those working at urban PHCFs reported ‘sometimes’.
Staff shortages at rural PHCFs were greater than at urban PHCFs and private healthcare facilities as 45% of graduates working at rural PHCFs reported not having sufficient staff 'very often' or 'most of the time' (not at all), compared to 35% working at urban PHCFs and none in the private sector. Regarding being happy with their remuneration, 43% (28/65) of those working in rural PHCFs stated ‘all the time’ or ‘most the time’, compared to 57% (25/44) working in urban PHCFs, and 53% (8/15) in the urban private sector (Table 4). The majority of graduates, irrespective of where they worked, believed they could earn more money working somewhere else – 74% of those at rural PHCFs, 84% at urban PHCFs and 93% in the urban private sector. Fifty-two percent of graduates working at rural PHCFs stated that their overtime hours were ‘not at all/not very often’ excessive, compared to 31% for those at urban PHCFs and 45% in the urban private sector. In all cases, irrespective of where they work, the majority were paid for overtime (Table 4). Again, total responses to some questions were less than the total number of participants.
Regarding professional development and support, the majority of graduates (80%), irrespective of where they worked, felt they are able to practise their skills in their current workplace, and 78% report that they have learnt something new from a professional perspective in the last 6 months (Table 5). Conversely, nine (14%) of the 66 graduates working at rural PHCFs reported to be ‘not very often’ or ‘not at all’, stimulated by their work, while no graduates working at an urban PHCF, or in the urban private sector reported this (Table 5).
With regard to having sufficient time to interact with peers about difficult cases, it appears no matter where graduates worked there was insufficient time, as indicated by 67% at rural PHCFs, 47% at urban PHCFs and 65% in urban private facilities responding ‘sometimes’, ‘not very often’ or ‘not at all’ (Table 5). However, access to senior staff appears to be available particularly in urban PHCFs (78%) and private facilities (81%), but less available (47%) at rural PHCFs (Table 5). Regarding personal professional development, 67% of graduates working in urban PHCFs are pursuing a further qualification, compared to 40% in the urban private sector and 38% at rural PHCFs (Table 5).
Regarding graduates’ intentions to leave their current place of work, 54% of those at rural PHCFs, 52% at urban PHCFs and 60% in the urban private sector intended to leave in the next 12–24 months (Table 5). The main reason cited by those at rural PHCFs (35%) and urban private facilities (43%) was ‘personal/professional development’, while for 35% of those at urban PHCFs it is to specialise (Table 5). Graduates working at rural PHCFs wanted to move to a regional hospital, city or into the private sector, while those working at an urban PHCF sought to move to a tertiary hospital to specialise (Table 5).
Regarding community integration, 59% of the graduates working at rural PHCFs indicated that they feel part of the local community (all or most of the time), compared to 40% at urban PHCFs and 60% in the urban private sector (Table 6). More than 60% of graduates, despite where they work, reported belonging to a local church or group in the community (Table 6).
Graduates who were no longer working at a rural hospital were asked to provide reasons why they had left – they were able to choose more than one reason (Table 7). The lack of funded posts at rural PHCFs was the main reason (40%) that graduates were not currently working at a rural hospital, followed by the desire of doctors to specialise (30%), requiring them to move to a tertiary urban hospital (Table 7).
Further, graduates were asked to state the two main reasons they work where they do. Graduates working at rural PHCFs cited the ‘ability to serve their community’ and being ‘close to family and friends’ as the main reasons, whereas those working at urban PHCFs cited ‘good work experience’ as the main reason (Table 8). There were only three responses from graduates working in urban private settings and hence the responses were not included.
Table 1: Demographic data of participants (n=135)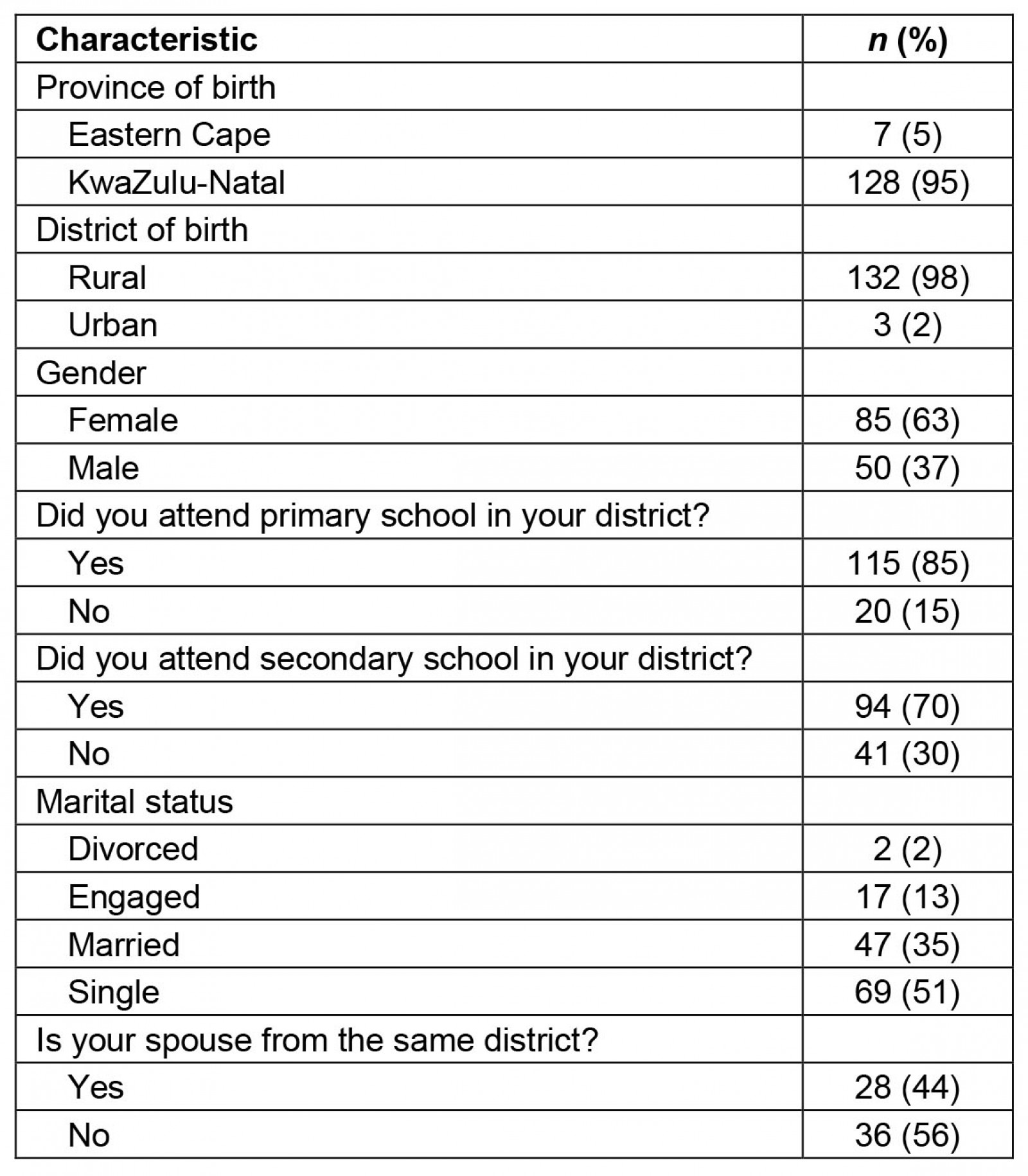
Table 2: Health science discipline of participants by place of work and gender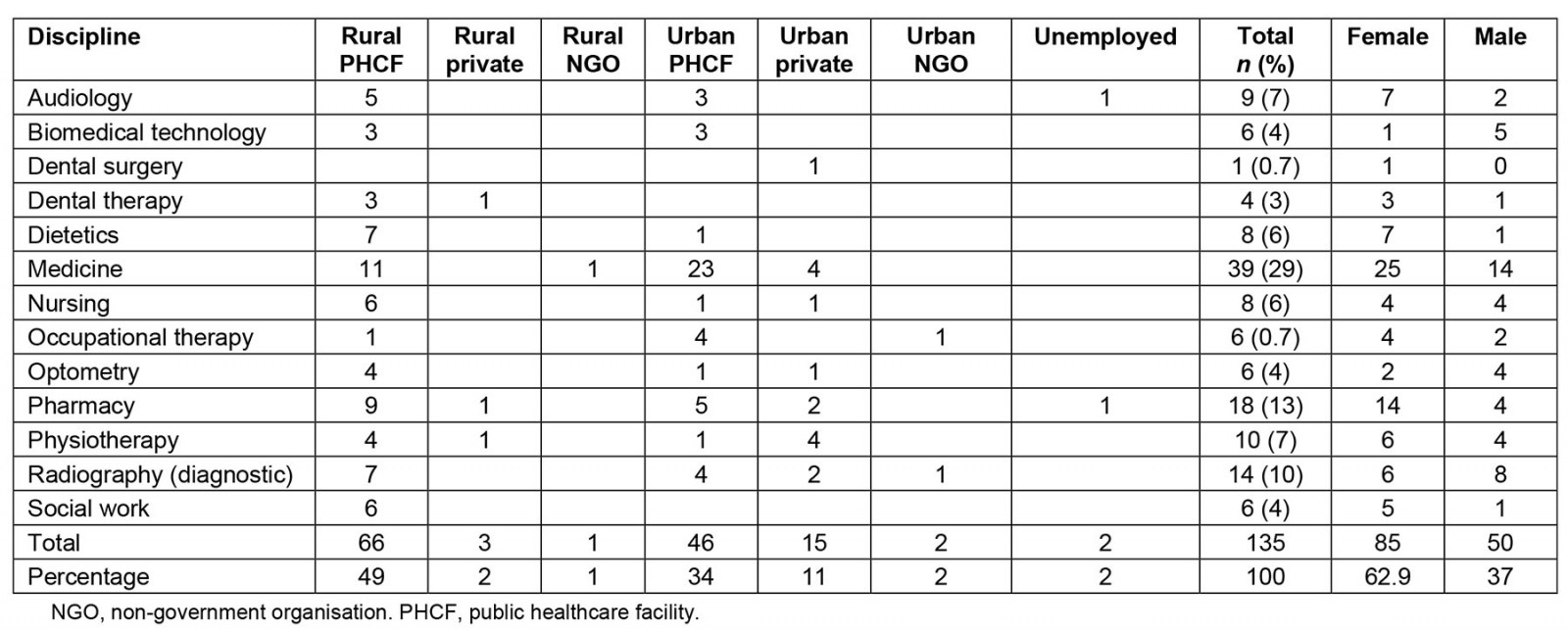
Table 3: Participant responses to questions about personal satisfaction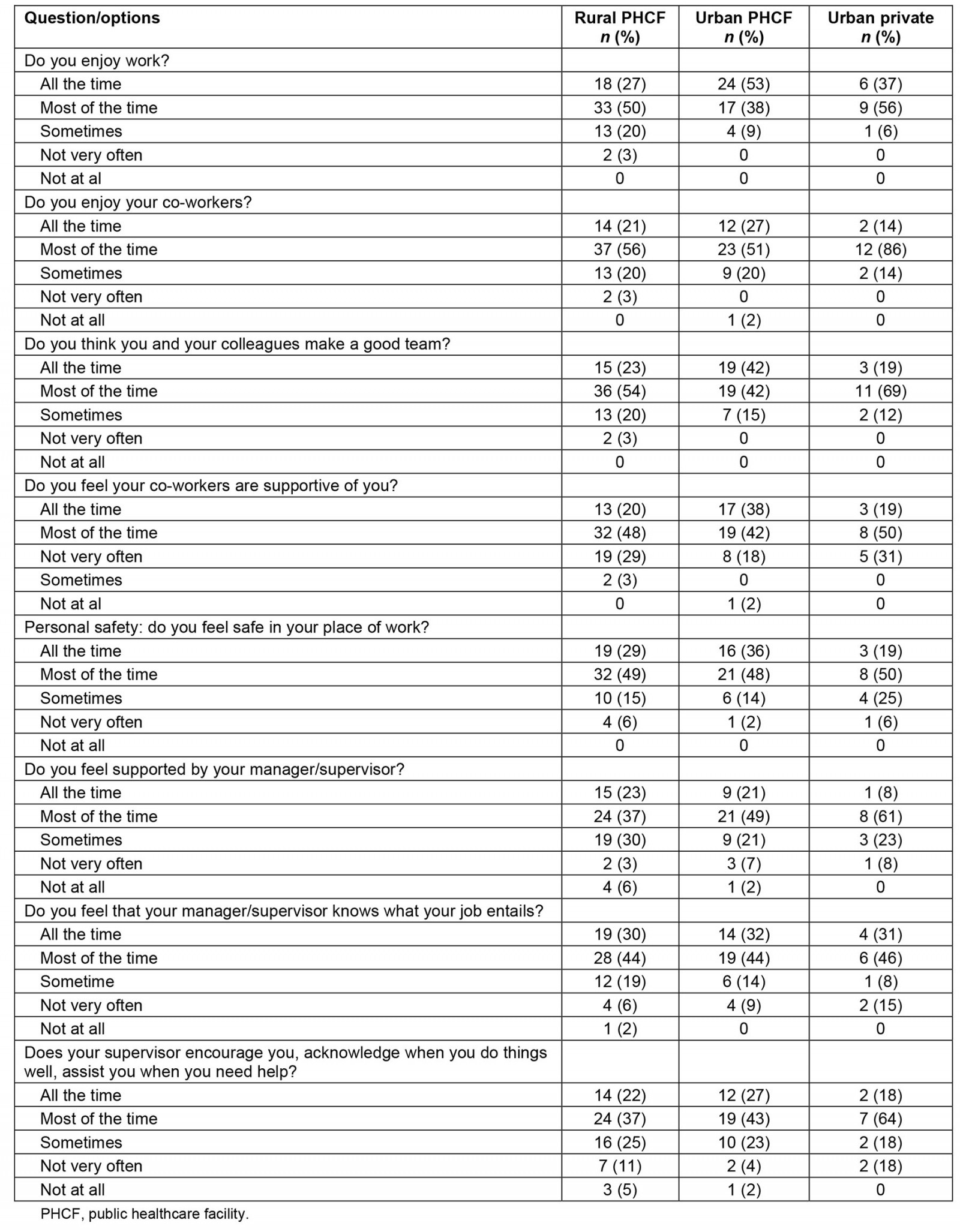
Table 4: Participant responses to questions about hospital resources and employment factors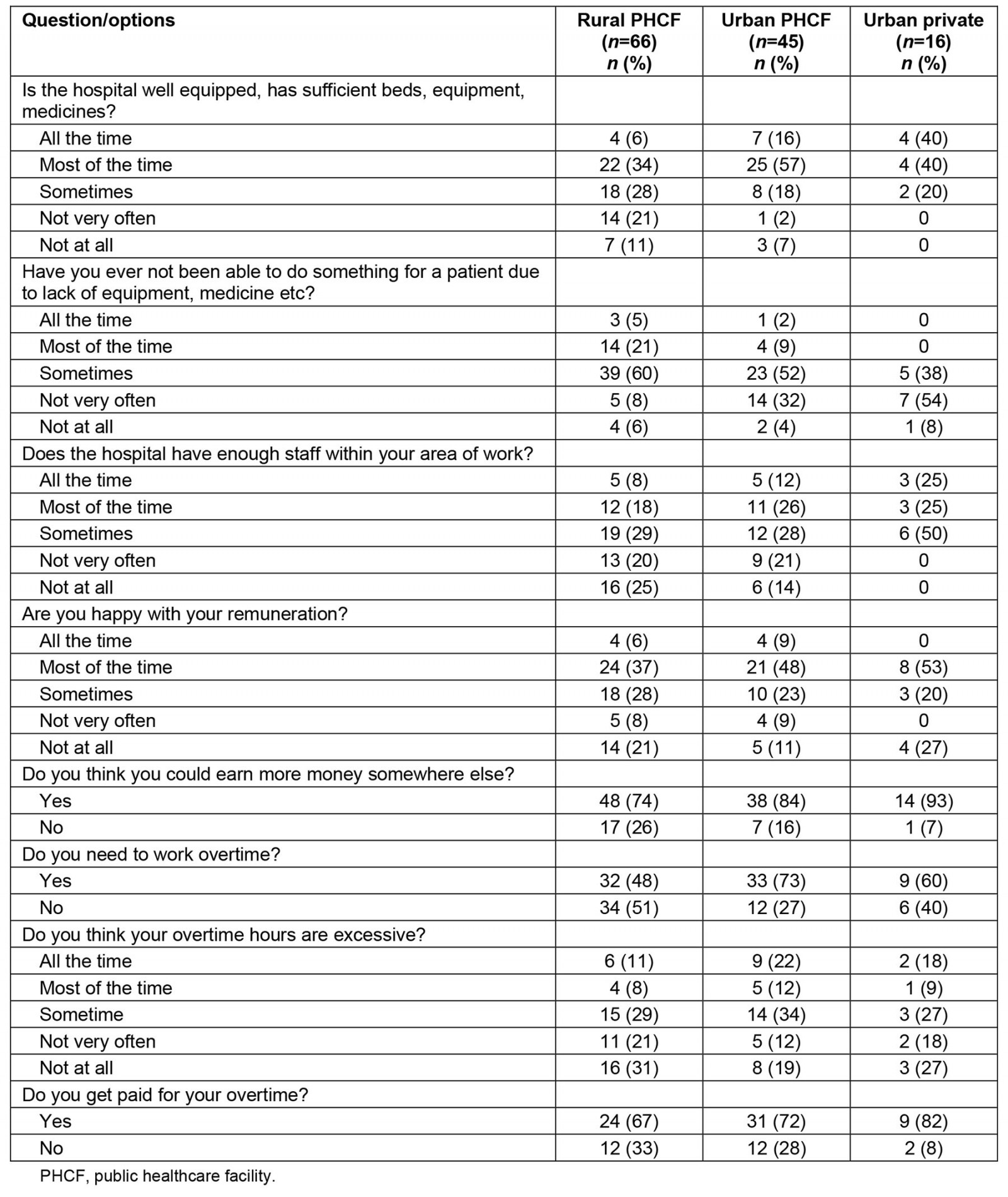
Table 5: Participant responses to questions about professional development and support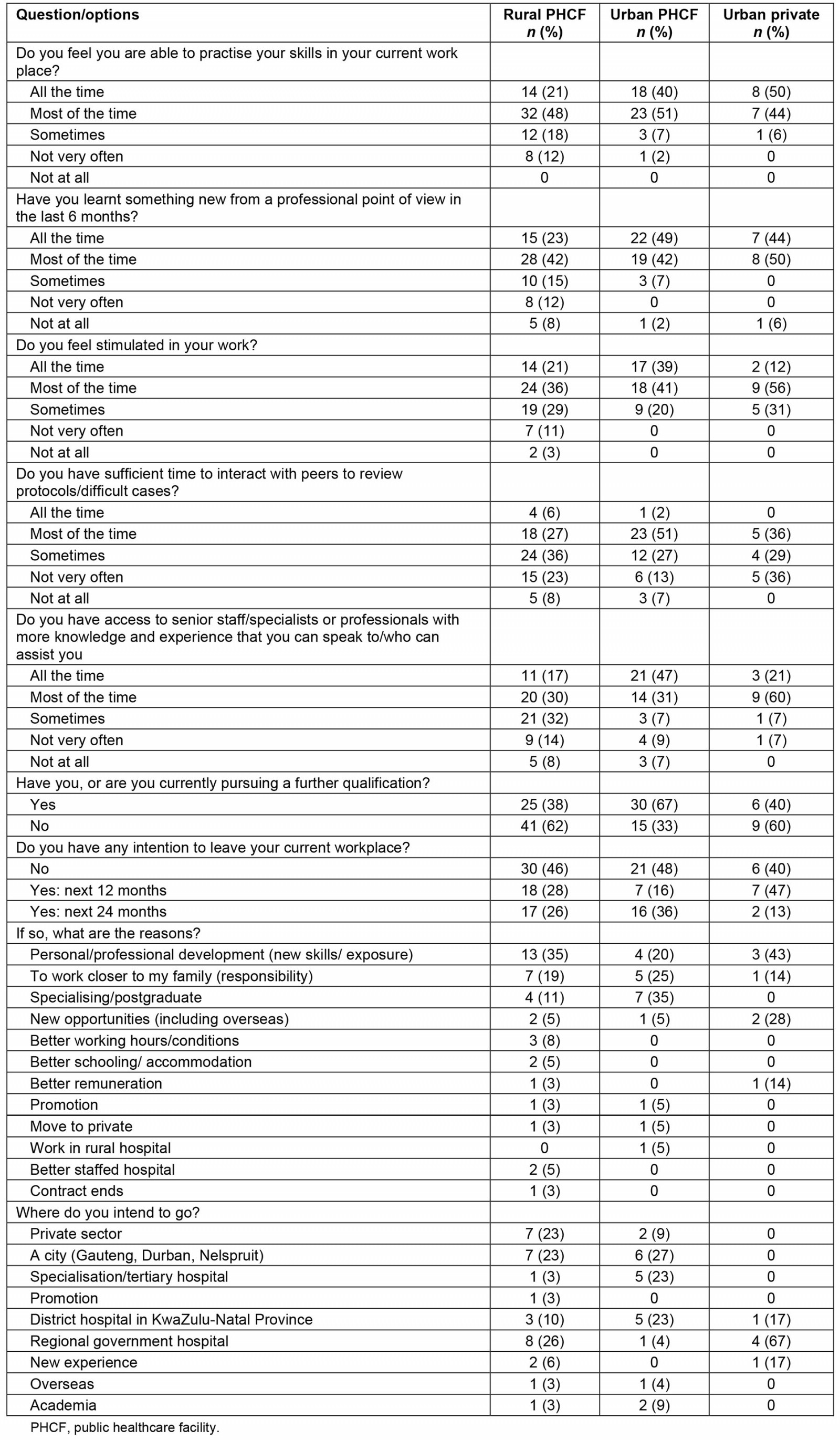
Table 6: Participant responses to questions about community integration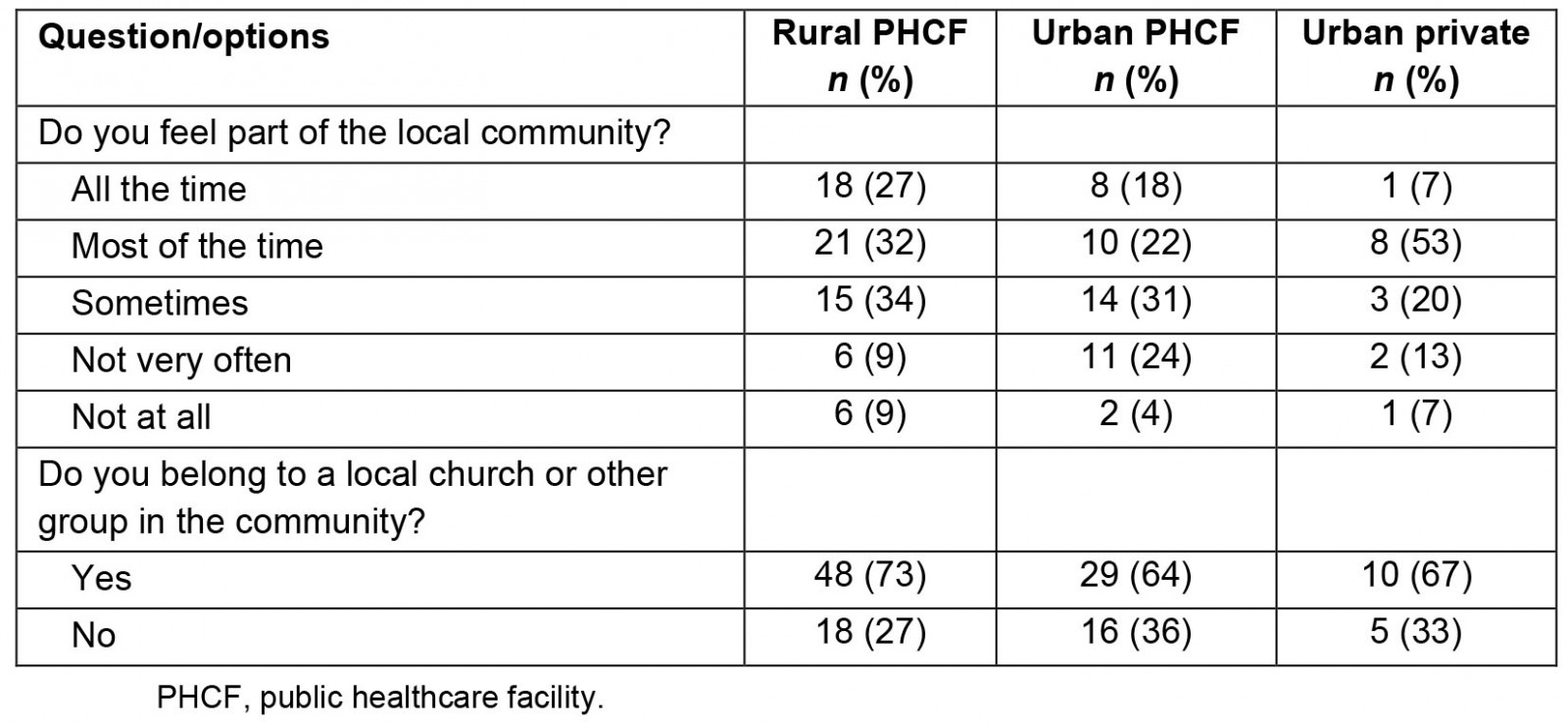
Table 7: Participant reasons for no longer working at a rural hospital (n=54)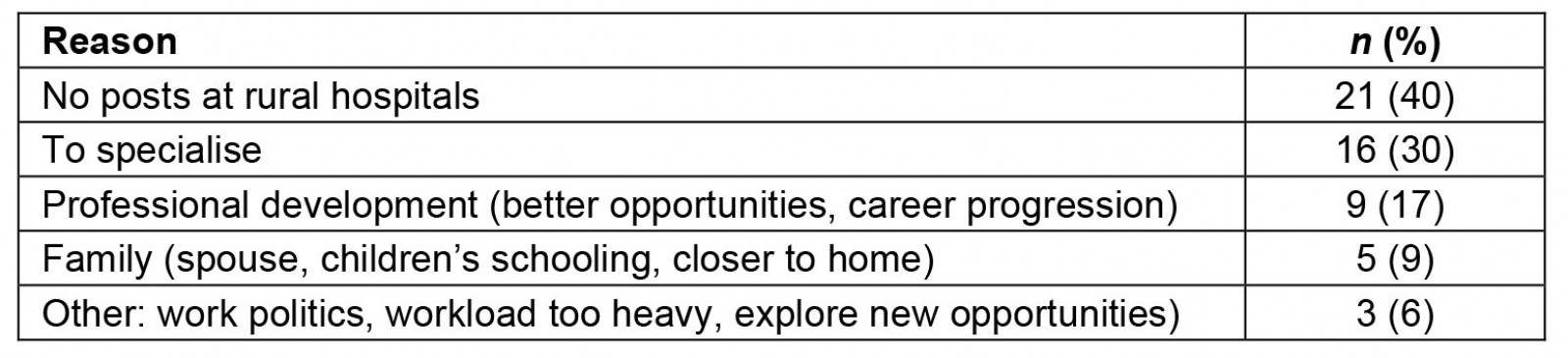
Table 8: Reasons participants work where they do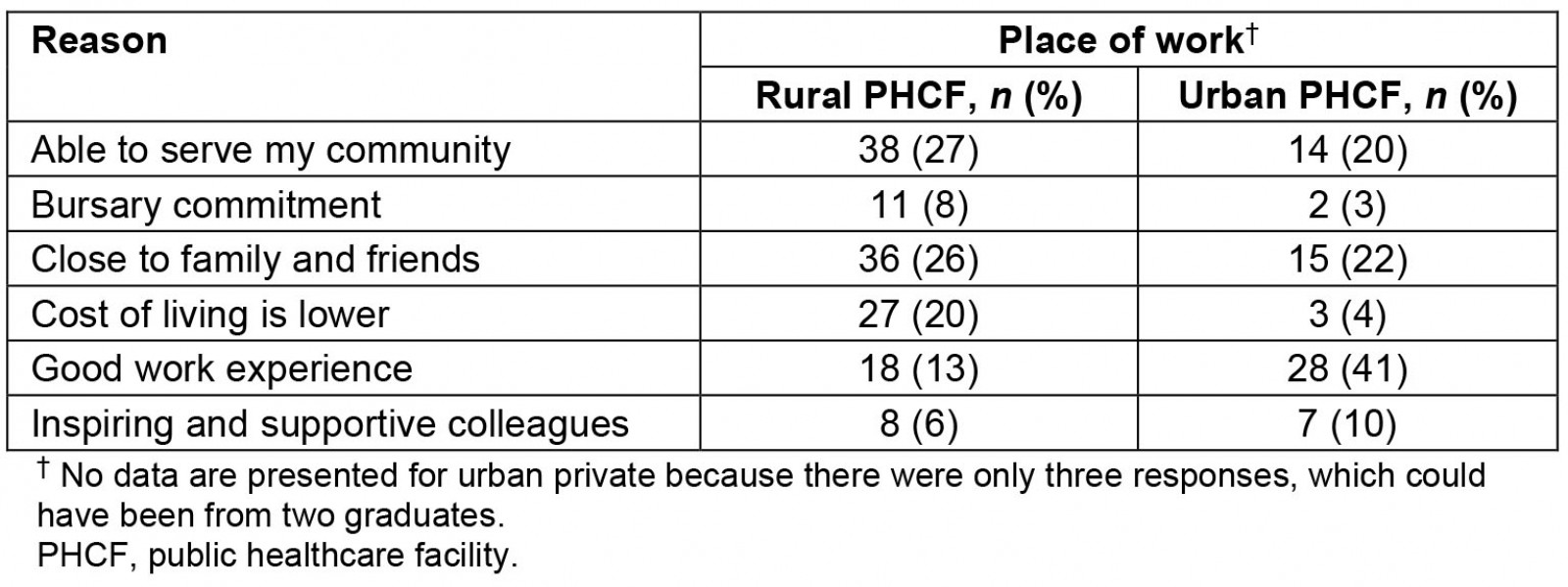
Discussion
The aim of the study was to determine the effects of various retention factors described in the literature on the choice of where rural-origin UYDF graduates worked, namely in a rural or urban, public, or private setting. All graduates in the study were of rural origin, with 98% originating from one of South Africa’s nine provinces, KZN, with 63% being female and the majority being doctors (29%), followed by pharmacists (13%). At the time of the study, 49% were working at a rural PHCF, 34% at an urban PHCF, and 11% in an urban private setting.
In terms of job satisfaction, it is encouraging that all participants, irrespective of where they worked, were happy with their working conditions, including their colleagues, felt part of a team, and felt supported by their managers. Further, the fact that the majority of graduates (70% at rural PHCFs, 91% at urban PHCFs, and 94% in private facilities) were able to practise their skills in their current workplace, and a high percentage (65% at rural PHCFs, and 91% at urban PHCFs and private) reported having learnt something new from a professional perspective in the last 6 months, is positive because these factors are critical, as highlighted by Mbemba et al11, to health worker retention, although the percentages were the lowest for graduates at rural PHCFs.
Those working at rural PHCFs reported that availability of hospital equipment and or medication were sometimes a challenge, resulting in patient care being compromised in some cases, which is a significant demotivator, as reported by Willis-Shattuck et al12. In addition, rural PHCFs suffered the most from staff shortages, placing an additional burden on existing staff, which is well documented in the literature3-6 and what UYDF seeks to address.
Despite more than 74% of graduates being satisfied with their remuneration (all the time, most of the time, sometimes), 74% of graduates working at rural PHCFs, 84% at urban PHCFs, and 93% in private settings believed they can earn more somewhere else, which appears contradictory, but may reflect the disparity in benefits between different cadres of health workers (eg some cadres do not receive a rural allowance despite working in a rural area); differences in benefits such as employer contributions to medical aids and provident funds, which may also differ between public and private employers, as well as terms of employment – casual/locum versus permanent. Importantly, although they believed they could earn more money elsewhere, only two graduates mentioned it as a reason to leave their current employment in future.
Despite reporting being able to practise their skills and having learnt something new from a professional perspective in the last 6 months, no matter where they worked, there was insufficient time to interact with peers about difficult cases. Those working at urban PHCFs and in private settings, however, reported that they had access to senior staff to assist them, which graduates at rural PHCFs did not have. The implications of a lack of senior staff at rural hospitals is that many more patients would be referred to secondary or tertiary hospitals, thereby extending or delaying the time to care of patients, as well as overwhelming the referral hospital with patients that ordinarily would have been treated at district level. This would be exacerbated by the shortages of staff at rural PHCFs, as reported above. In addition, in the absence of senior staff, rural health workers would not have the benefit of learning how to deal with such cases, thereby negatively affecting their personal and professional development.
Mbemba et al11, in reviewing articles on recruitment and retention of health workers in developing countries, found opportunities for professional advancement, professional support networks and financial incentives as the main factors impacting on retention, which was confirmed in this study. Willis-Shattuck et al12, having reviewed 22 articles on motivation and retention of health workers in developing countries, found that in 90% of the studies financial incentives were mentioned, followed by career development (85%), and hospital and clinic management (80%), with education and training opportunities having a strong motivating effect, as well as hospital infrastructure and resource availability, with lack of materials being a large demotivator. Recognition and appreciation by managers, colleagues or the community was mentioned to be important in 70% of the articles. All these factors have been shown to be relevant in this study.
Although, 84% of UYDF graduates were working in the public sector (49% at rural PHCFs and 34% at urban PHCFs), and only 11% working in the private sector, more than 50% of them intend to leave their current place of work within the next 12–24 months. Those working in rural PHCFs and urban private settings cited ‘personal/professional development’ as a reason, while a third of those at urban PHCFs sought to specialise. Graduates working at rural PHCFs wanted to move to a regional hospital, a city, or into the private sector, while those working at an urban PHCF sought to move to a tertiary hospital to specialise. Although the extent of staff mobility was not measured, the implication of continuous staff turnover, especially for rural PHCFs, is that critical skills are not retained as those with experience leave, perpetuating the problem of lack of senior staff for junior staff to learn from, which may compromise the delivery of certain services, while building a core, skilled team becomes more difficult.
A similar percentage (60%) of graduates working at rural PHCFs and in urban private settings reported feeling part of the local community, which is an important external factor affecting retention. It is not clear why such a high percentage of graduates working in urban private settings felt so integrated, as one would assume most of their family and friends lived in rural areas.
Lack of professional development opportunities, including the opportunity to specialise (career development), was cited as the main reasons graduates wanted to move from their current place of work, especially those working at rural PHCFs. Continuous professional development is a compulsory annual requirement for renewal of registration with the Health Professional Council; however, many of the continuous professional development activities are located in urban areas, making it difficult (and expensive) for rurally based health workers to participate in these activities. Lack of professional development opportunities related to distance and remoteness of rural PHCFs could be addressed by holding applicable courses within districts in which several hospitals are located, eliminating the long distances and extended time off work. Although not measured, the staff shortages at rural PHCFs would also impact on the ability of staff to undertake professional development opportunities due to distance and time away from work. Other options could include providing online professional development courses, especially to staff at rural PHCFs, assuming that stable and fast internet connections are available. Most specialist training is based at tertiary and regional hospitals situated in urban areas, and, therefore, necessitates a move to an urban area. This could be partially mitigated by offering specialist training in a decentralised manner, incorporating district hospitals, as has been done for family medicine specialist training in KZN. In addition, preferential selection of doctors for registrar posts could be given to those who have worked for a certain number of years at a rural hospital.
Regarding reasons for no longer working at a rural PHCF, lack of funded posts was cited as the main reason, which is the result of the KZN Department of Health attempting to reduce costs at the instruction of National Treasury, despite the need for more health workers, especially in rural areas4,8. This has been acknowledged by the National Department of Health4, and has resulted in as few as 10% of health workers of various key disciplines being absorbed in the public sector4. Strachan et al18 confirms this by reporting that only a tenth of medical graduates are absorbed into the public sector. This undermines all efforts to address health equity within the country19. Further, with many pressing national priorities, funding of posts in the public sector, and at rural hospitals specifically, will only become a priority if rural communities and rural hospital management can find a voice and pressurise the government into action, holding them to account based on the country’s constitution, specifically Section 27, which provides rights to healthcare services for all citizens. As the contractual obligations of graduates cannot be enforced by UYDF due to lack of funded posts after completing community service, the number of UYDF graduates working at rural PHCFs has decreased from 71% in 201514 to 63% in 201712, and now stands at 49%. In the absence of posts at rural hospitals, UYDF graduates are encouraged to obtain employment at regional (secondary) hospitals that serve as referral hospitals to the rural district hospitals, or obtain employment at any public hospital within KZN, or other provinces.
Regarding the reasons graduates work where they do, those working at rural PHCFs cited ‘their ability to serve their community’ and being ‘close to family and friends’ as the main reasons, while graduates working at urban PHCFs cited ‘good work experience’ as their reason. We believe the strong desire to ‘serve their community’ found among UYDF graduates is due to the expectation placed on them by UYDF, throughout their training, on their responsibility to go back and serve their communities, as well as the annual exposure throughout their studies to rural practice, facilitated by UYDF.
Government interventions in South Africa to attract and retain health workers to rural areas included the implementation of a rural allowance in 2004, a non-pensionable fixed percentage linked to the annual salary notch to most categories of health professionals, including doctors, dentists, dieticians, pharmacists, psychologists, radiographers, therapists and professional nurses with a 4-year diploma or degree20. However, the literature reports that financial incentives, in the absence of addressing the other critical factors, will not significantly improve retention21,22, which is confirmed in this study. Further, a 1 year compulsory community service was introduced for most health worker cadres in South Africa between 1998 and 2005, as a way of addressing staff shortages at rural PHCFs23,24. However, Reid23 reported that community service is ineffective in the absence of complementary longer-term human resource interventions to retain health workers in rural areas, which this study again affirms.
WHO6 highlights that many of the interventions are cross-cutting in nature, and that a Ministry of Health and/or individual healthcare organisations cannot solve the retention challenge on their own; this has been affirmed in this study, in that rural-origin health workers have been trained, and deployed, but cannot be retained due to financial constraints within the KZN Department of Health, as well as inadequate focus on retention of health workers. Engaging stakeholders across several sectors is a critical element for the success of rural retention policies, as it is for any type of health system or health workforce policy6. Ministries of civil service, finance and education, unions and professional associations, civil society, the private sector and, where appropriate, international development partners all have a role to play6.
Limitations
Since UYDF graduates were contractually bound to work at a rural hospital for the same number of years they were supported for, this may have caused a bias as to who responded to the survey because those who were non-compliant may have been less inclined to participate, despite the fact that compliance can no longer be enforced, and it being emphasised that the survey had nothing to do with their work-back status. Due to the sample being homogenous (ie all participants were of rural origin and Black African), statistical analysis was unable to highlight significant differences between graduates working in rural PHCFs or urban PHCFs, which may have been possible if there was a comparative group. Since less than half of the eligible graduates responded, it is not possible to know to what extent the responses reflect the group as a whole.
Conclusion
While nearly half of the rural-origin UYDF graduates surveyed continue to work in rural areas, this is considerably less than previously reported indicating that rural-origin health workers are similarly affected by retention factors as other health workers. The lack of funded posts at rural PHCFs is a major barrier to the employment and retention of health workers, and to addressing the unequal distribution of health workers between urban and rural PHCFs, and highlights that this program alone cannot solve the shortages of health workers in rural areas without commitment from government and other role players including economic development which might increase the attraction and retention of health workers in rural areas. It further highlights that focusing on the recruitment of rural students to become health workers, in the absence of adequate retention policies, is insufficient to adequately address shortages of staff at rural PHCFs, since in the absence of appropriate retention strategies, specifically professional development opportunities in this study, rural-origin graduates will move from rural PHCFs to facilities where they can access these benefits.
Funding
The research was self-funded.
Conflict of interest
The authors declare no conflict of interest.