






Introduction
In Australia, improvement in health service access by reducing systemic racism and enhancing cultural safety are key outcomes sought by the National Aboriginal and Torres Strait Islander Health Plan 2013–20231. Cultural safety is determined by the receiver of care and relies on cultural competency among all service providers. It is contingent on provider self-awareness and cultural proficiency2,3 enhancing clients’ sense of trust and feeling respected4,5.
Nevertheless, interrelated and compounding barriers, such as racism, cultural insecurity and paternalism, continue to challenge mainstream service providers with respect to Aboriginal peoples’ access3,6. This is particularly true in rural and remote areas that are already experiencing economic and environmental challenges, relatively high exposure to health risk factors and poorer service access generally7. Prout et al argue that for health practitioners to adequately respond in this context, characterised as it is by complexity and uncertainty, requires becoming cognisant of how one’s worldviews, values and attitudes intersect with one’s knowledge base and influence professional judgements and decision making processes7. An appreciation of one’s own cultural identity consistent with a culturally safe approach supports appropriate engagement with Aboriginal clients by focusing on self-reflection and change within the clinician, rather than change in the client or other workers8.
Self-reflection also nurtures practitioner empowerment and potential agency9-12. Empowerment has been broadly defined as a social action process that promotes improved mastery and control at personal, family, community and societal levels, improved quality of life and social justice13,14. Research among Aboriginal and Torres Strait Islander people highlights empowerment’s role in hope, goal-setting, communication, empathy, perseverance, better ability to identify the root causes of problems, and a belief that change can happen in the social environment13. Aboriginal, First Nations and Maori practitioners and scholars affirm the deep interconnections between healing from trauma experienced within communities as a result of past and continuing policies and practices, the experience of empowerment congruent with personal, family and core cultural values, and enhanced social and emotional wellbeing and self-determination4,10,11,15,16.
Aboriginal community controlled health services (ACCHSs) are specifically designed to improve Aboriginal people’s access to care using holistic multilevel empowerment approaches to engage individuals, families and communities6,17. ACCHSs face numerous workforce challenges, however, including stress arising from the multiple community and service roles expected of their staff in addressing cumulative, transgenerational trauma and lateral violence4,5. Insensitive individual and organisational responses to behaviours arising from such trauma and unresolved grief can perpetuate cultural insecurity, poor interpersonal relationships, inappropriate management responses, absenteeism, health problems, burnout, staff turnover and service ineffectiveness4,18,19. They may also contribute to an ambivalence among co-workers that perpetuates prejudice and discrimination based on interpersonal and systemic racism20.
Traditional postgraduate university education stemming from a biomedical model is not always conducive to developing cultural proficiency, nor the transformative learning from which empathetic understandings at a personal level develop and underpin healing processes embedded in trauma informed care. This circumstance and its interrelationship with workforce challenges, such as turnover among Aboriginal health workers due to stigma they experience from non-Aboriginal workers21, may contribute to the sharply reduced health status and poorer health outcomes experienced by rural and remote Aboriginal and Torres Strait Islander communities compared to their urban counterparts22,23.
Aboriginal-developed empowerment and leadership programs, such as the Family Well Being Program (FWB), can facilitate healing and promote wellbeing among service providers and community members13,24,25 and support transformational workplace team and leadership development26,27. FWB may also promote cultural competence using empowering processes that encourage self-awareness and reflexivity with respect to professional and organizational values and practices11,28. Reflexivity involves understanding one’s ‘professional, socio-cultural and personal standpoint including values, perspectives, attitudes, assumptions, beliefs, [and] behaviours regarding Indigenous people and their health’ (p. 28)29. An extension of self-reflection, reflexivity requires ‘exploration of self-positioning, to understand the lenses that influence our understanding of one another’ (p. 8)30.
Such empowering processes are also important in the tertiary studies context, particularly with so many students now enrolled in universities externally and often having limited face-to-face engagement with their peers and course convenors. Empowering learning experiences offer opportunities to enhance student resilience31 and wellbeing25. A student’s preparedness to critically reflect upon and question the values, identities and ethical bases of their professional and personal development32,33 – skills that are emphasised in emerging social and leadership competencies required of 21st century health professionals34,35 – is contingent on their sense of empowerment36.
Despite the national focus on strengthening workforce capacity in relation to Aboriginal health37, little has been reported on this aspect of postgraduate learning and its measurement. A small number of studies have evaluated transformative learning in relation to students’ attitudes, beliefs and preparedness to work in Aboriginal health contexts3,7,38-40, but these did not examine empowerment. Health Workforce Australia identified that cultural competency measures remain underdeveloped and needed to recognise each student’s developmental journey41. Existing measures of transformative learning such as the Learning Activities Survey are not designed to capture personal empowerment or wellbeing systematically, nor to measure change over time42,43.
One potential tool for use in education to examine the processes and impacts of empowering change in peoples’ broader lives is the multi-scale Growth and Empowerment Measure (GEM). The GEM, with its distinctive language and appearance, was specifically designed to measure steps in processes (12 Scenarios; S12) and impacts (14-item Emotional Empowerment Scale; EES14) of empowering change valued by Aboriginal and Torres Strait Islander people44.
The full GEM has been found sensitive to change among Aboriginal and non-Aboriginal males in treatment for substance abuse45 and its EES14 has shown sensitivity to change among child safety workers46 and undergraduate students25 introduced to FWB.
Two courses, designed by Muru Marri, the dedicated Aboriginal Health Unit in the School of Public Health and Community Medicine, UNSW Sydney, explicitly sought to stimulate transformative learning based on Aboriginal empowerment principles, with postgraduate health professionals facilitated to grow in how they understood themselves, appreciated strengths in others, recognised trauma and its multilevel impacts and saw and made meaning of the world7,47. This article reports on the feasibility, sensitivity and specificity of the full GEM in measuring empowering change among a largely non-Aboriginal cohort of postgraduate students completing these courses.
Methods
The authors tested two hypotheses: first, that the GEM would be sensitive to change at individual and group levels among students; second, that the GEM would reveal different patterns of change between the two courses, corresponding to differences in content and delivery.
Learning context
Two 13-week postgraduate electives were designed in direct response to calls from communities desperate for skilled practitioners with an appreciation of Aboriginal worldviews. These were the Aboriginal public health ‘Perspectives’ course and the Aboriginal empowerment and wellbeing ‘Lifespan’ course. Through dialogue and reflection, both courses aimed to change the lens through which students viewed Aboriginal health.
Student engagement was fostered through initial face-to-face workshops on Bedegal Country at UNSW Sydney’s Kensington campus, supported by comprehensive learning materials, structured online discussions and assessments aligned with real-world application. Both courses were designed and co-facilitated by a team of Aboriginal and non-Aboriginal academics and community leaders, including the faculty’s inaugural Aboriginal Elder-in-Residence; and the emphasis was on social competency development through learning experiences that promoted student social, emotional and spiritual wellbeing and growth48. Within this context it was considered appropriate to pilot the GEM as a tool for interpreting the student experience, given its focus on reflexivity, transformation and empowerment.
The Perspectives course used an innovative scenario planning process and ecological lens to think strategically about collaborating with Aboriginal communities to fulfil local, workplace and national policy imperatives49. Over the two workshop days, students engaged in deep listening, and in reflective dialogue stimulated by interactions with facilitators and each other. In one activity, students reflected on the video Crossing the line, which depicts the experiences of two medical students who undertake a placement in an Aboriginal community in Far North Queensland50. While watching the video, students were asked to focus on one of the characters (eg medical superintendent, Aboriginal health worker, community member) and to speak from that character’s position in the semi-structured conversation that followed. By shifting their perceptual positions51, students vicariously explored points of view different to their own. Later reflection on this exercise revealed students valued being able to delve into previously unexplored assumptions, the myriad structural barriers within the Australian healthcare system, and to have gained a deep appreciation of the inner strengths the residents portrayed. As one student commented, ‘they sort of informed my reading and my perspective and … kind of made me reassess my own thoughts and how I should approach my work and guide my thinking’.
A second activity involved short trigger videos produced by the university. Three Aboriginal women, one from regional NSW and two from regional and remote Northern Territory, as well as two non-Aboriginal academics, contemplated what Aboriginal health and wellbeing is to them, and what it would take to make a difference to the current situation. These vignettes prompted a staged, semi-structured, scenario-building process that involved brainstorming a vision of the future, which students then built on through ongoing, small-group, collaborative online discussions of potential barriers and enablers, before arriving at a proposed set of actions aimed at improving Aboriginal health and wellbeing outcomes49,52,53.
In the Lifespan course, students experienced a 3-day immersion in stage 1 of FWB, led by accredited Aboriginal facilitators. Students worked together in large and small groups to consider their inner qualities, basic human needs, emotions, relationships, conflict resolution, beliefs, attitudes and life journeys. Reflective journalling was encouraged, and key concepts in Aboriginal health, social and emotional wellbeing, culture and empowerment theory were reinforced in formal presentations. Students then had the opportunity to integrate their new insights into structured online discussions that investigated psychosocial and physical health challenges faced at various life stages by many Aboriginal people as well as written assignments where they demonstrated their understanding of multilevel empowerment. This format stimulated continuing engagement, reflection, and individual and group dialogue around concepts and their application personally, professionally and more broadly.
Sample and recruitment
Over 6 years (2010–2015), all students commencing the workshop for Perspectives (N=109) and Lifespan (N=85) were offered the opportunity to take part in evaluating each of the courses. The GEM was used during the pre-course workshops as a prompt to encourage critical reflection on aspects of empowerment important to Aboriginal people at individual, family and organisational levels46 and, from consenting students, to obtain de-identified baseline measures of those domains, as well as characteristics such as age, gender, occupation and Aboriginal and Torres Strait Islander status, mode of enrolment and study pattern.
Following the release of final grades, students were mailed a post-course GEM and letter requesting its completion and return in an enclosed postpaid envelope.
GEM scales
The GEM’s S12 examined processes of empowerment that enable people to gain more control and psychosocial wellbeing in their lives44. For each of the 12 scenarios, respondents chose from one of four states of empowerment and wellbeing that best matched their situation, or one of three intermediate options (Fig1). For example, scenario 7 asks the question ‘Do you have a sense of knowing who you are?’, with response options ranging from ‘I don’t know who I am’ (scored as 1) through to ‘I’m very strong about who I am’ (scored as 7). Two subscales are associated with S12: Healing and Growth, and Connection and Purpose44. A newly defined short form of S12, the Core6, has emerged from confirmatory factor analysis of GEM responses collected from more than 900 Aboriginal and non-Indigenous people (Table 1).
The Emotional Empowerment Scale (EES14) is a 14-item, five-point Likert scale used to capture specific signs or impacts of empowerment people perceive within themselves in their everyday lives44. Scores range from 1 (‘least desirable situation’) to 5 (‘most desirable situation’). It has two subscales, EES Inner Peace and EES Self-Capacity44. Confirmatory factor analysis led by the second author has indicated that item 8, ‘belong in community, feel connected’, loaded strongly on the Self-Capacity subscale. Therefore, in this article, EES Self-Capacity included items 5, 6, 7, 8 and 9 (Table 1).
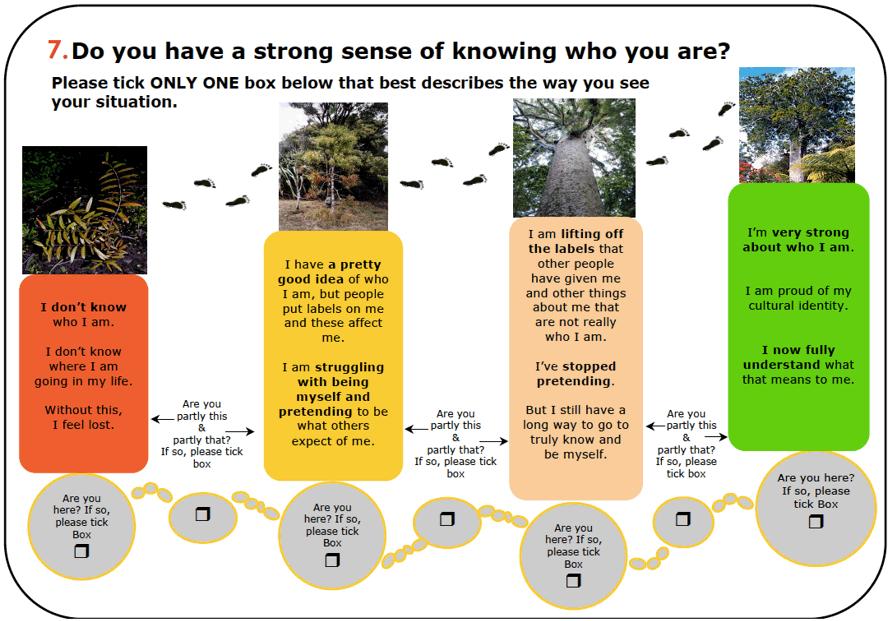 Figure 1: Examples of the seven potential states within each scenario item of the Growth and Empowerment Measure44.
Figure 1: Examples of the seven potential states within each scenario item of the Growth and Empowerment Measure44.
Table 1: Estimates of Growth and Empowerment Measure scale and subscale reliability and homogeneity, with participants’ mean item scores at baseline arranged in ascending order (including the Core6) 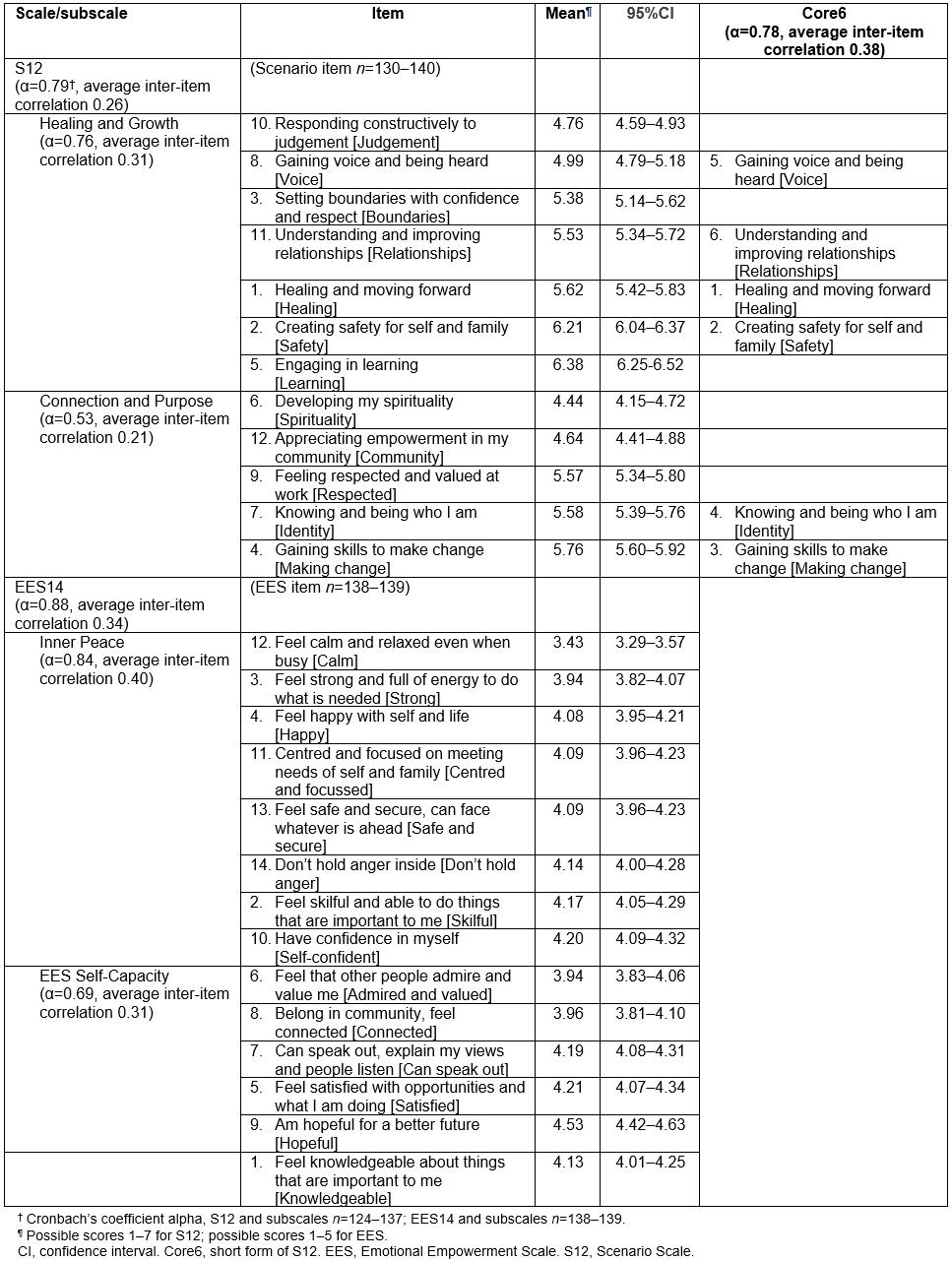
Data management and statistical analyses
Over 6 years, students’ administrative and GEM data (including participants’ demographics) were reviewed and coded. Duplicate administrative and demographic data from students attending twice were removed prior to descriptive analysis. Survey pairs were matched, and analysed using the Statistical Package for the Social Sciences v23 (IBM Corporation; http://www.spss.com). Post-workshop and focus group feedback were also reviewed.
Assumptions of normality in differences between pre- and post-course means were tested using the Shapiro–Wilk test. Internal consistency at baseline was tested using Cronbach’s coefficient alpha and assessed using criteria for short scales54. Post-course scores for three students with extremely large increments for the S12 were excluded due to the improbability that magnitude of change was associated with the course alone, which also corrected normality of data.
Relationships between variables were explored using Pearson’s correlations, homogeneity of variances tested using Levene’s test and differences between baseline means for each scale examined by course using analysis of variance.
Pre- and post-course scale and subscale means were compared using matched paired sample t-tests and for individual items using related-samples Wilcoxon signed-rank tests (p<0.05). Analysis and reporting was by individual course as well as ‘combined’ (Perspectives and Lifespan together). Magnitudes of group-level change are reported, with effect size calculated from paired differences (Cohen’s dz)55, with a small effect suggested by dz=0.2, medium by dz=0.5, and large by dz=0.8 standard deviations.
Ethics approval
This study received ethics approval from UNSW’s Medical and Community Human Research Ethics Advisory Panel (2010-07-28; 2012-7- 22; 2014-7-25) and was guided by the National Health and Medical Research Council’s Aboriginal and Torres Strait Islander Values and Ethics56.
Results
Student feedback
Qualitative feedback revealed a majority of students found the pre-course workshops ‘very interesting’, ‘valuable’, ‘relevant to their work’ and ‘beneficial to their future endeavours’. Insights into ‘working with, not for’ Aboriginal people, identity, empowerment, strengths-based approaches and relationships were frequently reported. Some students felt discomfort yet weighed this against valued learning from each other and support from facilitators. Opportunities to interact, establish trust and reflect in a safe environment were highly valued and frequently reaffirmed. As one regional manager in NSW described, she was fundamentally reassessing her team’s approach to program development:
We can’t work that way, it’s inappropriate … we have to sit back and work with [name of Aboriginal community controlled health service] at their pace and be mindful of not taking over … And that’s worked really well. I actually think it’s quite successful. It’s changed the way we work. It’s been very rewarding. And I got that out of the course … about how to build partnerships.
Baseline Growth and Empowerment Measures
Among the total 194 student workshop attendances, 147 baseline GEMs (75.8%) were collected from 138 consenting participants. Nine participants attended both courses. Participant mean age was 36.7 (range 21–78) years. Most were female (n=102, 74.5%), non-Indigenous (n=126, 92.6%), studying part time (n=103, 75.7%) and enrolled externally (n=79, 58.1%).
Most participants (n=70, 60.2%) were living in Sydney at the commencement of their studies. A further 23 (18.0%) were living in other places in NSW, 27 (21.1%) elsewhere in Australia, and one (0.8%) lived overseas. Forty-four students (31.7%) had lived in regional Australia at some time in their lives.
Nearly one-third (n=35, 29.9%) reported their occupation as doctor, nurse, dentist or psychiatrist, and a further 24 (20.5%) worked in allied health. Most students were completing single (n=74, 41.3%) or various double degrees in the Master of Public Health program (47, 26.2%), while 13 (7.3%) came from the Master of Forensic Mental Health program.
At baseline, the EES14 and S12 achieved modest average inter-item correlations (0.34 and 0.26) and an acceptable Cronbach’s alpha (0.88 and 0.79 respectively) (Table 1). Distributions among scales and subscales were generally normal.
Average Scenario scores (out of a possible 7) were lowest for ‘developing my spirituality’ (4.44), ‘appreciating empowerment in my community’ (4.64), ‘responding constructively to judgement’ (4.76) and ‘gaining voice and being heard’ (4.99). Mean scores were highest for ‘gaining skills to make change’ (5.76), ‘creating safety for self and family’ (6.21) and ‘engaging in learning’ (6.38).
Average EES item scores (out of a possible 5) were lowest for ‘feel calm and relaxed even when busy’ (3.43), ‘feel strong and full of energy to do what is needed’ (3.94) and ‘feel that other people admire and value me’ (3.94). They were highest for ‘can speak out, explain my views and people listen’ (4.19), ‘have confidence in myself’ (4.20), ‘feel satisfied with opportunities and what I am doing’ (4.21) and ‘am hopeful for a better future’ (4.53).
A slight positive correlation was observed between participants’ age and baseline means for most scales and subscales, with Pearson’s r ranging from 0.23 to 0.36 (p<0.05).
No significant difference was observed in baseline scores of pre-course GEMs between the two courses.
Differences pre- and post-course
Post-course survey returns yielded a total of 55 matched pre- and post-course pairs, allowing analysis of change from 29 students completing Perspectives (from a total of 95, 30.5%) and 26 students completing Lifespan (from a total of 75, 34.7%).
Data from three students who returned matched pairs from two course experiences remain included (exclusion had no impact on the findings). Similar to the overall sample of participants, a majority of the matched pairs were completed by females (81.5%), studying part-time (72.2%), with a mean age of 37.9 years.
Statistically significant increases (p<0.01) were observed between the pre- and post-course scores on all GEM scales and subscales in the combined courses (Table 2). Effect sizes on various subscales were moderate, ranging from 0.43 to 0.72.
Furthermore, baseline scores were an important predictor of change increments, such that participants with lower baseline scores had significantly greater increments on all scales and subscales compared to those with higher baseline scores. Correlation coefficients between starting scores and increments of change ranged from –0.40 (EES Inner Peace) to –0.62 (Connection and Purpose scenario subscale) (Table 3).
Table 2: Pre- and post-course means, magnitude of change and effect size for the Emotional Empowerment Scale (EES14), 12 Scenarios (S12) and its short form Core6, and subscales, among students providing paired Growth and Empowerment Measures in Perspectives, Lifespan and combined courses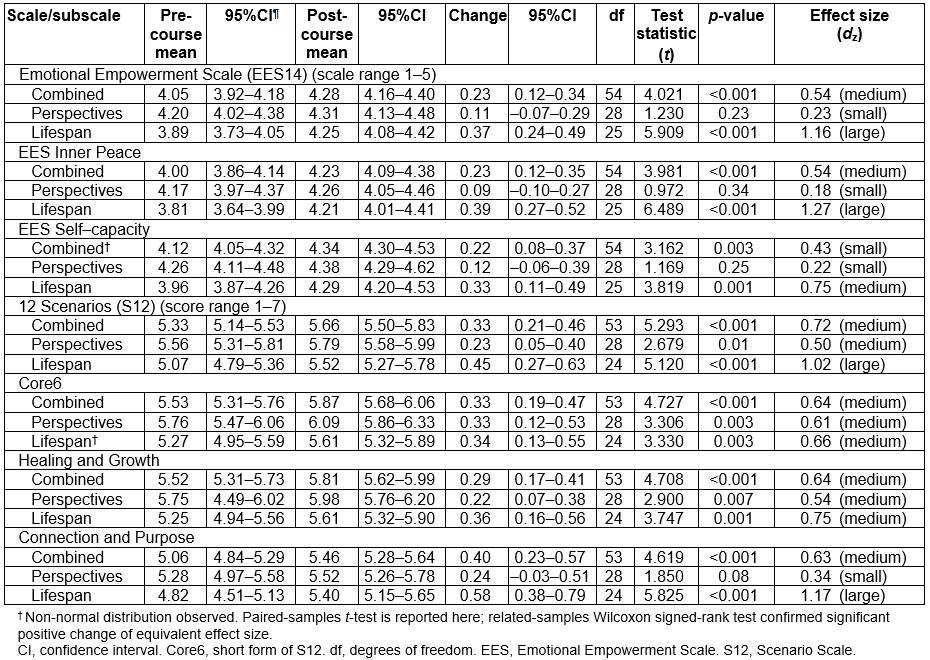
Table 3: Correlations (Pearson’s r) between baseline scores and pre- and post-course increments in Growth and Empowerment Measure (GEM) scales and subscales among 54 paired GEMs from all participants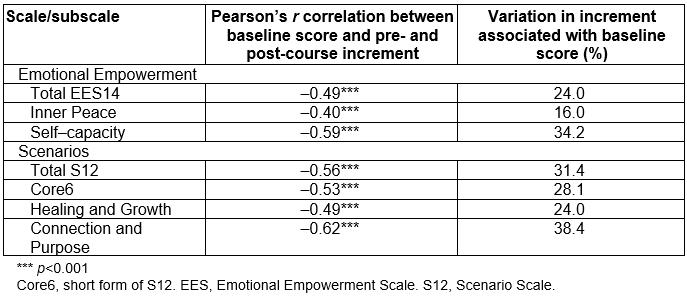
Course-specific outcomes
Examination of post-course GEMs revealed evidence of self-selection among those received from Lifespan participants. Participants in the Lifespan course who returned a post-course GEM had significantly lower baseline means compared to those who did not return a post-course GEM for S12, its subscales and Core6 (F(1,67)=12.67; 9.88; 11.48; 9.45 respectively, p<0.01) as well as EES14 and its subscales (F(1,67)=8.23; 7.94; 6.98 respectively, p<0.01). In contrast, no difference in baseline means was observed among Perspectives participants who did or did not return a post-course GEM.
Stratification by course revealed different patterns of change among subscales (Table 2). While participants taking either course reported similar significant positive change in Core6 and the scenario subscale Healing and Growth, the increments for EES Inner Peace and the scenario subscale Connection and Purpose were markedly larger for Lifespan students compared to those taking Perspectives. In Lifespan, effect sizes for Inner Peace and Connection and Purpose were large (dz=1.27 and 1.17, respectively) compared to absent-to-low for Perspectives (dz=0.18 and 0.34, respectively).
Individual scale items by course: Differences in change between each course for individual scenario items are shown in Figure 2a. Perspectives students reported highly significant change from pre to post in two scenarios, ‘voice’ and ‘identity’, of medium and large effect size respectively (p<0.01). Students completing Lifespan reported statistically significant change (p ranging from 0.03 to <0.001) in five scenarios (ordered here from moderate to largest effect size): ‘identity’, ‘community’, ‘make change’, ‘judgement’ and ‘spirituality’.
Substantial differences in change related to the two courses were also observed for individual EES items (Fig2b). Comparison of pre- and post-course scores found no statistically significant change in any item among Perspectives students, whereas students completing Lifespan reported statistically significant change (p ranging from 0.05 to <0.001) of medium to large effect size in 11 items (p<0.05), along with change in ‘self-confident’ approaching significance (p=0.05). ‘Satisfied’ and ‘calm’ showed no significant change.
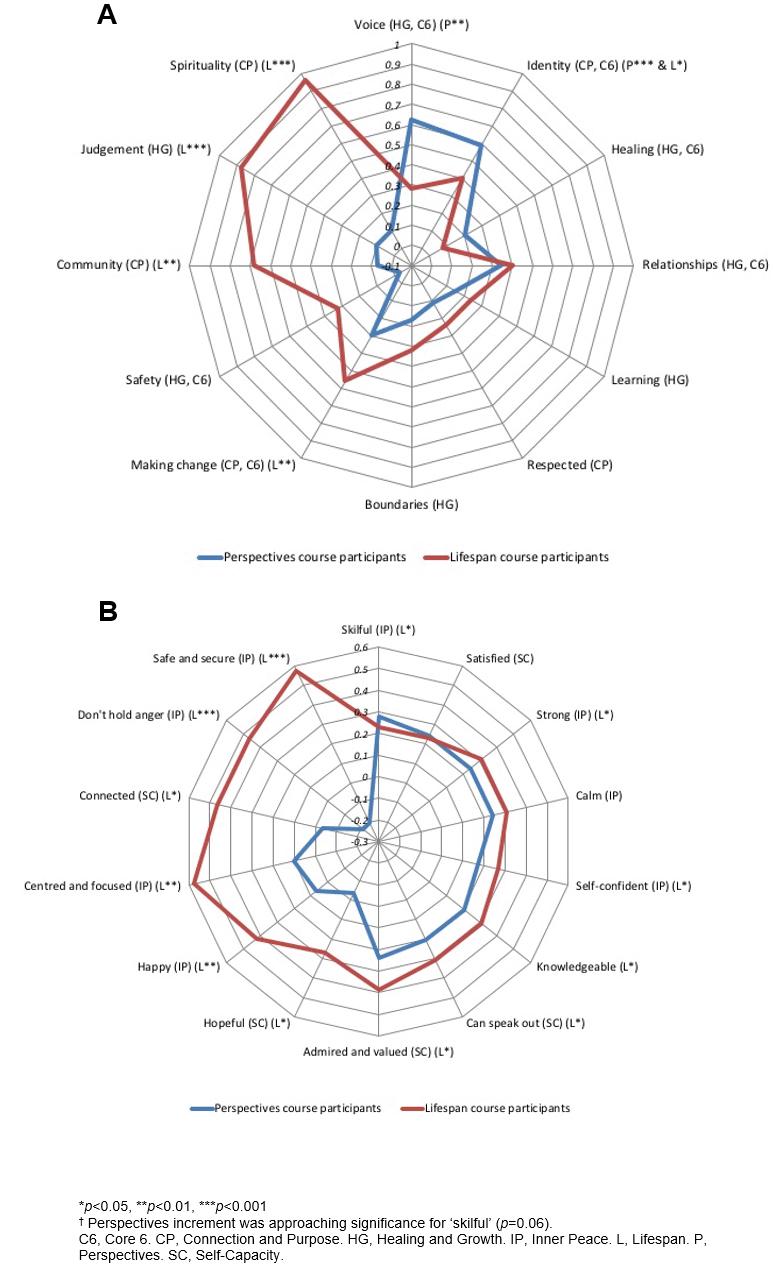 Figure 2: A. Increments of change (post-course minus baseline scores) across 12 individual scenario items reported by students following completion of each course. B. Increments of change (post-course minus baseline scores) across 14 individual Emotional Empowerment Scale items reported by students following completion of each course.
Figure 2: A. Increments of change (post-course minus baseline scores) across 12 individual scenario items reported by students following completion of each course. B. Increments of change (post-course minus baseline scores) across 14 individual Emotional Empowerment Scale items reported by students following completion of each course.
Discussion
The Perspectives and Lifespan courses were designed to foster transformative learning experiences through dialogue and reflection within safe and empowered social environments11,13. Congruent with the multi-level nature of empowerment, bonds formed between students within the face-to-face workshops were carried into subsequent online discussion groups that continued to challenge students to reflect on themselves, their roles in organisations and their capacity to contribute to changing disempowering structures in Australian institutions and society57,58.
Significant positive change in the GEM’s process (S12; dz=0.72) and impact measures (EES14; dz=0.54) for the combined courses supports the authors’ primary hypothesis that the GEM is sensitive to changes stimulated by participation in these courses.
The findings also confirm that the GEM appears to be both sensitive and specific to the different types of changes sought within each individual course, supporting the authors’ second hypothesis. The large effects on the EES Inner Peace subscale and the scenario subscale Connection and Purpose suggest that the inclusion of the Aboriginal Family Well Being Program within Lifespan stimulated a deeper sense of social and emotional wellbeing and connection59, compared to the small effect observed in the Perspectives sample (dz=1.27 and 0.18 for Inner Peace and dz=1.17 and 0.34 for Connection and Purpose, respectively). As well as confirming the GEM’s predictive validity in measuring the impact of empowerment programs, this study extends earlier work25,46 by using the scenarios to explore 12 aspects of change in everyday life processes behind such growth. Feedback from Lifespan workshop participants corroborated some of these changes, for example in responding constructively to judgement, through frequent references to the value of the FWB sessions on relationship dynamics and conflict resolution.
Interestingly, the Core6 subset of scenarios captured the most consistent change shared by participants of the two courses, and did not capture differences between them. This finding suggests the value of using the full 12 scenarios when maximum analytical power is desired for understanding the nuances of personal change.
Mindful of both similarities and differences across cultures in the conception of wellbeing59, findings at baseline provide a unique profile into factors contributing to the wellbeing of study participants and their sense of wider engagement in their community. Given the importance of student mental health, the finding of higher scores in the ‘making change’, ‘safety’ and ‘learning’ scenarios, as well as the generally positive correlation with age, align well with earlier research that suggests better coping skills among postgraduate than undergraduate students60. However, the low baseline for the ‘spirituality’ and ‘community’ scenarios is concerning, given collective good is a core principle of public health61. The large increase in these components within Lifespan demonstrates that it is possible to boost students’ sense of connection and collective purpose within education62.
The significant change in students’ ‘identity’ observed across both courses suggests students have embraced self-reflection, become more self-aware and have potentially experienced learning that is transformative38,63,64. This suggestion is supported in the course feedback; for example, ‘It is making me think about everything I do at work and all my attitudes ...’ (female, general practitioner). This finding potentially informs the long-standing question held by learning theorists as to ‘what form transforms?’47, which Illeris has suggested is identity64. It also recalls Wenger’s ‘Learning is a social becoming’ (p. 181)65, where new ideas have been engaged through the practice of collaborative reflection and meaning making, explored through participation in dialogue, and reified through the production of assessments.
Within-course changes in individual scenarios were largely reflective of the different aims of each course. In Perspectives there was significant increase in ‘voice’, suggesting high student engagement in the course’s action-oriented, scenario-building activity, as well as growing understanding of structural impediments to Aboriginal peoples’ health and students’ resolve to advocate for change. Furthermore, slightly negative increments associated with the EES items ‘don’t hold anger’ and ‘safe and secure’ may reflect students’ growing appreciation of social injustice. In contrast, Lifespan’s psychosocial development focus was linked to striking increases in the ‘spirituality’, ‘judgement’, ‘community’ and ‘making change’ scenarios. This suggests enhanced awareness of higher values such as altruism33, which FWB is known to stimulate66, and which were then integrated through further dialogue and reflection over the semester, a process not unlike psychosynthesis67.
The findings provide insight into the inner qualities of postgraduate students opting into two different Aboriginal health and wellbeing coursework experiences. Students were in a facilitated, Aboriginal-led context, learning about Aboriginal health through learning about themselves. This provokes questions about how this self-awareness may drive leadership in the collective endeavour of health system reform through transforming structures and organisations4,26. Further qualitative analysis is underway to understand key components of student learning.
Changes were observed across the GEM despite important challenges during the analysis, which limited the authors’ ability to precisely estimate and compare effect sizes. Firstly, there was a high loss to follow-up, a well-recognised pattern in evaluations involving university students. Sample sizes among pilot studies are often small68, and while the paired-sample size of 55 was sufficient to detect significant change, potential for bias in returning post-course surveys limited generalisability of findings. Furthermore, the finding that pre- and post-course increments of change were smaller among students who commenced the courses with higher baseline scores suggests a possible ceiling effect within the GEM for many postgraduate students. Nevertheless, consistently positive workshop feedback encourages the authors to believe the benefits of the courses were widely felt. Administering the paper-based form of the GEM was resource-intensive and an electronic version would enhance feasibility in university contexts.
This study also highlights the importance of researcher awareness about how individual starting points may influence comparisons of change processes in different circumstances. Like Whiteside et al25, the authors observed greater change among participants who started at lower levels of self-reported empowerment compared to those starting at higher levels. However, participants in Lifespan who started with lower scores were found to be more likely to return a post-course GEM, whereas baseline scores did not predict their return in Perspectives. This observation might suggest the empowerment experience itself is an effect modifier, increasing the desire and confidence of those most consciously aware of their personal growth to have their experience recorded.
Conclusion
This study is the first time the GEM’s S12 and EES14 have been used together to explore components of the process and impact of teaching Aboriginal-informed aspects of empowerment to postgraduate students. The 12 scenarios allowed exploration of rarely measured domains of psychosocial empowerment, with important findings observed at baseline as well as from studying Aboriginal health. It is tempting to suggest that the experience of Lifespan helped to correct initial psychosocial inequities, enabling the most disempowered students to experience profound growth over the semester. It is important to remember here how unique it is to measure these aspects of student learning, and that just as they relate to student empowerment and positive wellbeing, they also relate to Aboriginal peoples’ concepts of how health is understood59.
The GEM is proposed as a potentially useful tool for also measuring transformative learning valued in Aboriginal and rural health education7. For example, strengthened identity (scenario 7), self-efficacy (scenario 4) and an understanding of empowering relationships (scenarios 11 and 12) are closely aligned with outcomes sought in transformative education. The findings support the potential usefulness of the 12 scenarios in understanding the impact of empowering change and evaluating the wider goal of educators to promote enhanced social competencies and sustainability in public health practice. To explore this further, mixed methods studies using in-depth qualitative analysis of student experience and electronic media to enhance post-course response rates is recommended.
Acknowledgements
Special thanks to Aunty Ali Golding and the late Alan Hodgkinson for their vision and leadership in promoting Aboriginal health and wellbeing education, to Rachelle Arkles and our reviewers and editors for their feedback on this paper, to Sarah Gaskin for data entry and to Stats Central UNSW for early advice. This study is a component of a professional doctorate being undertaken by Sally Fitzpatrick as part of UNSW’s Future Health Leaders Program, and contributes in-kind to the Lowitja Institute and to the Aboriginal Health and Wellbeing Stream of Maridulu Budyari Gumal (the Sydney Partnership for Health, Education, Research & Enterprise).